EUS Unit Hospital Clnico Concepcin CHILE Univ Concepcin

. • Gastrointestinal")

")

 19731999: 13715 cases Modlin et")



















 “Clinical manifestations, diagnosis,")





 is a more sensitive marker than urinary")




- Slides: 39
EUS Unit Hospital Clínico Concepción, CHILE Univ Concepción Fac Med - Int Med Dpt Sept 26 -27 2009 SANTOS - BRAZIL EUS in diagnosis and Staging Rectal Carcinoid. Al Francisco Llanos P. - Al Pedro Pablo Guerra Q. Fernando Itaro Kawaguchi MD Ph. D. M. Ocares MD(1), L Rios EU(3), V Salas TP(2), J Madariaga MD(4), K. Caamaño EU(3), A Sepulveda ING(3), Benavides MD(1), C Zuñiga MD(1), C Santander MD(1), JL Castillo , Ms. C(5), O Venegas MD(5), J Schalper(4), R Gutierrez(4), D Esteban(2), R Branada(2), K Palma EU(2), K Kawaguchi(6), R Luco(7), V Sawada(8), A Fernandez(9), I Ruiz QF(10), E Eriz (11), A Guzman(3). 1. - UNIDAD COLOPROCTOLOGIA. 2. - UNIDAD EUS 3. - CENTRO GI BIOARRAYANES, 4. - SECCION ANAT. PATOLOGICA. 5. - UNIDAD CITOMETRIA FLUJO. 6. - OTORRINO U DE C. 7. - UNIDAD PENSIONADO, HCRC 8. - DIRECCION HOSPITAL REG CONCEPCION. - 9. - SERV ONCOLOGIA HCRC. - 10. - FARMACIA HCRC. - 11. - UNIDAD APOYO DOLOR.
Colo-rectal Cancer • Increasing incidence(> 900 patients per year in last decade). • Gastrointestinal cancer is prevalent in Chile. • GI cancer is the third cause of death in our country: males and females. • In males, rectal cancer is the most frequent colo-rectal cancer. • Encouraging prognosis. • Found in 8 per 100, 000 post-mortem analysis. R. Avendaño, P. Fernández, M. Deichler, “Poliposis de colon” published in “Cuadernos de cirugía v. 21 n. 1” 2007, Universidad Austral de Chile.
Distribution of 13, 715 NETs I. Modlin et al 2007 Am J Gastro
CARCINOID INCIDENCE All sites Digestive system Modlin, SEER 9 Registry (1973 -2002)
Incidence – 2003 GI Carcinoids and Adenocarcinomas Carcinoids
Carcinoid Tumors SEER data (Surveillance Research Programme of NCI) 19731999: 13715 cases Modlin et al Cancer 2003 Incidence per 100, 000 population: Third National Cancer Survey 1969 -71 and SEER 1992 -99 White males White females Black females 1992 -1999 (1969 -1971) 2. 47 (1. 31) 2. 58 (1. 63) 4. 48 (2. 16) 3. 98 (1. 87) ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Carcinoid Tumor: USA: The age-adjusted incidence has increased in the last 35 years. • 55% Gastrointestinal location. • 30% Broncho pulmonary location. Gut tumors 13 to 34% are carcinod tumors. • Inside GI tract (SEER database): v v v 45% Distal small intestine, mainly: ileum. 20% Rectum. 16% Vermiform appendix. 11% Colon. 7% Stomach. ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Rectal Carcinoid Summary • Arises from etherochromaffin cells. • NET 5 HIAA urinary test. • No sexual or age related susceptibility. • Over-represented among the black and Asian populations. ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Rectal Carcinoid • Mainly asymptomatic, however , decreases fecal quantity , causes rectorragy, pain and rectal tenesmus. • When sickness becomes symptomatic (Carcinoid sindrome) metastases become more frequent: ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Rectal Carcinoid Staging T and Metastases: v Less than 1 cm, metastases are infrequent. v Among 1 - 1. 9 cm, 10% metastases v Larger than 2 cm, 70% metastases v Another criterion: -Muscularis propria invasion. -Lympho-vascular invasion. -High mitotic rate. ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Rectal Carcinoid ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Rectal Carcinoid ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Rectal Carcinoid Differents classifications Typical: Atypical: Uniform cell patterns, rare mitotic activity, no evidence of local invasive growth, bloodstream, lymphatic vessels or neuronal structures. Local invasion or cell pleomorphism. T 1 Mucosa or submucosa T 2 Muscularis propria T 3 Full rectal wall T 4 Surrounding tissue WHO clasification(NETs): Well-differentiated : -Benign Behaviour: -Uncertain Behaviour -Low Grade Malignant Behaviour: Poorly differentiated -High Grade Malignant Potential NET = benign/uncertain behavior NEC = some degree of malignancy ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Rectal Carcinoid Staging &Prognosis Proposed Staging for Rectal Carcinoid Tumors 5 years survival T 1 < 2 cm, without muscularis propria invasion 100% T 2 > 2 cm, without muscularis propria invasion 77% T 2 < 2 cm with muscularis propria invasion 77% T 3 > 2 cm with muscularis propria invasion 43% T 4 M 1 18% SEER database 1977 -2004 pts: 4704, Landry MD, ELSEVIER GLOBAL MEDICAL NEWS ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Francisco Llanos Prado - Pedro Guerra Quintana Fernando Kawaguchi P.
Francisco Llanos Prado - Pedro Guerra Quintana Fernando Kawaguchi P.
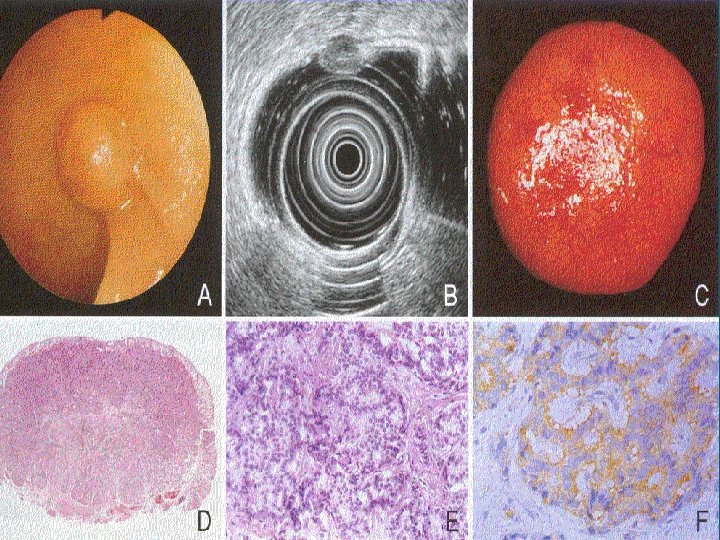
Rectal Carcinoid “Many carcinoid tumors are discovered incidentally during endoscopy or radiographic procedures planned for other purposes” ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
“Many carcinoid tumors are discovered incidentally during endoscopic or radiographic procedures planned for other purposes” AMERICAN GASTROENTEROLOGICAL ASSOCIATION GUIDELINES: “Endoscopy alone is not reliable for detecting the etiology of a subepithelial gastric mass. ” “Cross-sectional imaging techniques such as transabdominal ultrasonography, computed tomography, and magnetic resonance imaging are adequate for detecting the presence of normal or abnormal structures outside the gastric wall but do not reliably distinguish between the various causes of masses arising within the gastric wall ” “Endosonographic characterization of subepithelial lesions of the upper gastrointestinal tract” published in www. uptudate. com february 11, 2009. Mary Lee Krinsky, DO & Kenneth Binmoeller, MD” ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Traditionally, the diagnosis of rectal carcinoid tumors mostly depends on digital examinations, barium enema and colonoscopy. Using these procedures, it is difficult to determine the real size, layer of the origin, and histological nature of the tumor. Zhou PH, Yao LQ, He GJ, Gao WD, Qin XY. Clinical. application of ultrasonic probing for preoperative staging of colorectal carcinoma. Asia J Surg 2003; 26: 18 -20. Federspiel BH, Burke AP, Sobin LH, Shekitka KM. Rectal and colonic carcinoids: a clinicopathologic study of 84 cases. Cancer 1990; 65: 135 -140. ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Ultrasound Endoscopy • It is a medical procedure which combines endoscopy and ultrasound to obtain images of internal organs in chest and abdomen • It can be used to visualize the wall of these organs, and adjacent structures • Combined with Doppler imaging, nearby blood vessels can also be evaluated. • It allows biopsies and associate with FNA. • Approximate 10 - 15 minutes. • Allows intraoperative monitoring and follow up. • Allows endoscopic excision by itself. ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Ultrasound Endoscopy • It provides an understanding of whether the lesion arises from the bowel wall (intramural) or from a structure outside the bowel wall (extramural) compressing the gastrointestinal wall. • It can determine the originating layer of intramural lesions, an important clue for achieving a diagnosis. • The echogenicity, vascularity, margins, size of the lesion, and absence or presence of adjacent lymphonodes also helps to narrow the differential diagnosis. • Provides a minimaly invasive treatment for these tumors. ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
AMERICAN GASTROENTEROLOGICAL ASSOCIATION GUIDELINES: “EUS is the most accurate imaging test for detecting the component of the gastric wall from which the mass arises, information which, combined with the echogenicity of the mass, helps narrow the differential diagnosis ” “Endosonographic characterization of subepithelial lesions of the upper gastrointestinal tract” published in www. uptudate. com february 11, 2009. Mary Lee Krinsky, DO & Kenneth Binmoeller, MD” ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Accuracy in staging T EUS TC scan 80 to 95 % 65 to 75 % MRI 75 to 85 % “TEUS correctly identified 62 percent of patients with T 3/4 disease that were missed by CT” Sensitivity and specificity TEUS T 1 88 and 98 % T 2 88 and 98 % T 3 96 and 91 % T 4 95 and 98 % Endoscopic ultrasound in rectal cancer Gavin C Harewood, MD & Mauritis J Wiersema, MD, may 2009 ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
“The Endosonography exceeds the capacity of other tests to identify the degree of depth of transmural invasion and the presence of peri-rectal nodes involved in rectal cancer. ” EUS TC scan MRI (T) 80 - 95% 65 -75% 75 -85% (N) 70 -75% 55 -65% 60 -65% EUS FNA Biopsy “Clinical manifestations, diagnosis, and staging of colorectal cancer” Published www. uptudate. com april 17, 2009. Dennis J Ahnen, MD & Finlay A Macrae, MD ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
EUS together FNA increases even more the accuracy in staging (N) “Clinical manifestations, diagnosis, and staging of colorectal cancer” Published in www. uptudate. com en abril 17, 2009. Dennis J Ahnen, MD & Finlay A Macrae, MD ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Comparative cost-time requests Required time MRI 20 – 90 mins TC scan 15 – 60 mins EUS 10 – 20 mins Costs MRI $735 CT scan $275 EUS(rectal) $92 ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
• According to the guidelines for treating rectal carcinoid tumors, less than 10 mm with SM involvement have a low risk of metastases, and endoscopic excision is considered curative. • As for the lesions measured between 10 mm and 15 mm with SM involvement, local excision and regional lymphadenectomy is desirable. • As a minimally invasive technique, endoscopic resection offers the promise of localized treatment of these tumors, with relatively few complications and rare mortality. • Various endoscopic Rectal Carcinoid resection, such as endoscopic polypectomy, strip biopsy, aspiration resection, band-snare resection have been described as effective treatments Francisco Llanos Prado - Pedro Guerra Quintana Fernando Kawaguchi P.
EUS RECTAL CARCINOID RESECTION However, complete resection of carcinoid tumors of the rectum is difficult with conventional polypectomy, because nearly 75% of the tumors extend into the submucosa. Fujimura Y, et al. A carcinoid tumor of the rectum removed by strip biopsy. Endoscopy 1993; 25: 428 -430. 8. Kobayashi K, et al. Indications of endoscopic polypectomy for rectal carcinoid tumors and clinical usefulness of endoscopic ultrasonography. Dis Colon Rectum 2005; 48: 285 -291. 9. Jung IS, Ryu CB, Kim JO, . Rectal carcinoid treated by EMR. Gastrointest Endosc 2003; 58: 253 -255. 10. Matsumoto T. EUS in rectal carcinoid tumors: contribution to selection of therapy. Gastrointest Endosc 1991; 37: 539 -542. ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
“This is the most accurate scan to assess tumor size, and ideal for showing the indemnity of the muscularis propria, being these two factors seem to conditionate the possibility of distant metastases. Thus, we will be able to direct accurate therapeutic strategies, in both presurgical management, and neoadjuvant therapy as also postsurgical monitoring. In other hand offers the promise of localized treatment for these tumors. ” ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D
Chromogranin A • Plasma chromogranin A (CGA) is a more sensitive marker than urinary 5 -HIAA in patients with: -carcinoid tumors -functioning pancreatic islet cell tumors -nonfunctioning pancreatic islet cell tumors -higher level; in patients with diffuse metastases Plasma CGA levels also have prognostic value Urinary 5 -HIAA • Serial measurement of 5 -HIAA in 24 -hour urine for carcinoid tumors • Elevated urinary 5 -HIAA levels are highly specific for carcinoid tumors • 5 -HIAA levels are most useful with primary midgut carcinoid tumors • Foregut and hindgut carcinoids only rarely secrete serotonin PATHOLOGY CLASSIFICATION SYSTEMS NOT UNIFORM NO VALIDATED PROGNOSTIC SYSTEM STAINING, EXTENT, Ki 67, MITOTIC COUNT, HORMONE PRODUCT PAUCITY OF PATHOLOGICAL AWARENESS
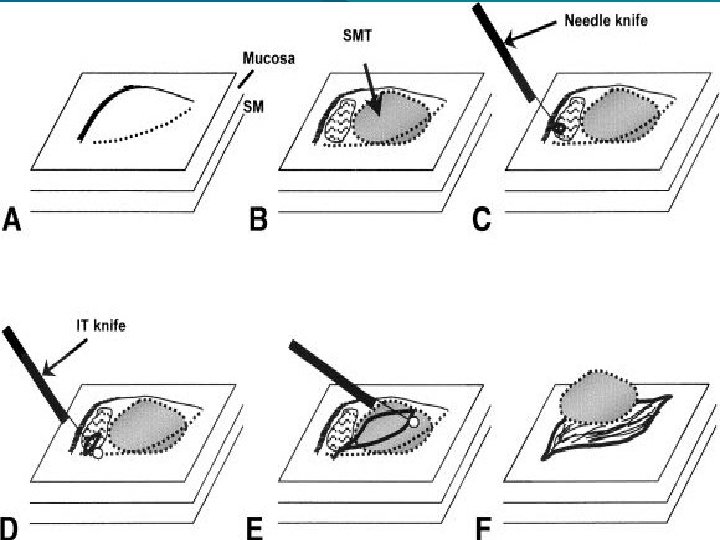
EUS SM SIMPLE MINIMALLY INVASIVE TREATMENT SM EUS lesions requires special treatment for deeper resection to achieve clear margins. This can be done by lifting the lesion, either with SM injection of saline solution (conventional EMR) or by aspiration and banding (ESMR), followed by snare resection. Kajiyama T, et al. Endoscopic resection of gastrointestinal submucosal lesions: a comparison between strip biopsy and aspiration lumpectomy. Gastrointest Endosc 1996; 44: 404 -410. Oshitani N, et al. Endoscopic resection of small rectal carcinoid tumors using an aspiration method with a transparent overcap. J Int Med Res 2000; 28: 241 -246. Nagai T, et al. Saline-assisted endoscopic resection of rectal carcinoids: cap aspiration method versus simple snare resection. Endoscopy 2004; 36: 202 -205. Ono A, et al. Endoscopic submucosal resection of rectal carcinoid tumors with a ligation device. Gastrointest Endosc 2003; 57: 583 -587. Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P.
EUS SM SIMPLE MINIMALLY IMVASIVE TREATMENT Placing the snare below the band, ESMR provides a significant deeper vertical resection margin and, theoretically, a higher rate of curative resection. In a word, EUS offers new possibilities for the diagnosis of rectal carcinoid tumors. ESMR is a simple, minimally invasive, and safe procedure for rectal carcinoid tumors. Kajiyama T, et al. Endoscopic resection of gastrointestinal submucosal lesions: a comparison between strip biopsy and aspiration lumpectomy. Gastrointest Endosc 1996; 44: 404 -410. Oshitani N, et al. Endoscopic resection of small rectal carcinoid tumors using an aspiration method with a transparent overcap. J Int Med Res 2000; 28: 241 -246. Nagai T, et al. Saline-assisted endoscopic resection of rectal carcinoids: cap aspiration method versus simple snare resection. Endoscopy 2004; 36: 202 -205. Ono A, et al. Endoscopic submucosal resection of rectal carcinoid tumors with a ligation device. Gastrointest Endosc 2003; 57: 583 -587.
Tissue markers with diagnostic and prognostic use in GEP-NET AGENT Role Use Sensitivity Chromogranin-A 90%, synaptophysin, neuron-specific enolase Histopathological identification and classification Identification of neuroendocrine neoplasia High KI-67 antigen Proliferation index Assessment of rate of cell proliferation High Protein families of; transforming growth factor β; vascular endothelial growth factor; and epidermal growth factor Growth factors and regulators of proliferation Assessment of regulatory mechanisms and potential targets of novel therapeutic agents Intermediate Receptors for: somatostatin (subtypes 1 – 5); cholecystokinin; vasoactive intestinal peptide; pituitary adenylate cyclase-activating polypeptide; tachykinin; serotonin; and dopamine Hormone receptors Assessment of receptor-specific treatment; for somatostatin, assessment of therapeutic effectiveness with somatostatin analogues (either cold or radioisotopically labelled) Somatostatin receptors: high; serotonin receptors: intermediate; other receptors: low to unproven AF-10, insulin-like growth factor binding protein 3, P 21 (cyclin-dependent kinase inhibitor 1), P 27, CD 99 antigen, transcription factor jun-D Oncoproteins or cell-cycle control proteins Indicators of proliferation and potential for aggressive behaviour and metastasis Low to unproven Neural cell adhesion molecule 1, CDX 2, transcription termination factor 1, synaptic vesicle glycoprotein Regulators of cell function Indicators of neuroendocrine differentiation and potential for aggressive behaviour Low to unproven Modlin et al. Lancet Oncology 2008; 9(1): 61 -72
EUS Unit Hospital Clínico Concepción, CHILE Univ Concepción Fac Med - Int Med Dpt Sept 26 -27 2009 SANTOS - BRAZIL EUS in diagnosis and Staging Rectal Carcinoid. M. Ocares MD(1), L Rios EU(3), V Salas TP(2), J Madariaga MD(4), A Heisser EU(3), A Sepulveda ING(3), Benavides MD(1), C Zuñiga MD(1), C Santander MD(1), JL Castillo , Ms. C(5), O Venegas MD(5), J Schalper(4), R Gutierrez(4), D Esteban(2), R Branada(2), K Umaña EU(2), K Kawaguchi(6), R Luco(7), V Sawada(8), A Fernandez(9), I Ruiz QF(10), E Eriz (11), A Guzman(3). 1. - UNIDAD COLOPROCTOLOGIA. 2. - UNIDAD EUS 3. - CENTRO GI BIOARRAYANES, 4. - SECCION ANAT. PATOLOGICA. 5. - UNIDAD CITOMETRIA FLUJO. 6. - OTORRINO U DE C. 7. - UNIDAD PENSIONADO, HCRC 8. - DIRECCION HOSPITAL REG CONCEPCION. - 9. - SERV ONCOLOGIA HCRC. - 10. - FARMACIA HCRC. - 11. - UNIDAD APOYO DOLOR. ALS: Francisco Llanos Prado - Pedro Guerra Quintana - Fernando Kawaguchi P. MD Ph. D