Eur Heart J 2013 34 3478 3490 Heterozygous

 Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490")







 Diagnosed FH (estimated) 33, 300 Netherlands 71%")














 • <3. 5 mmol/L(<135 mg/d. L) for")







- Slides: 33
Eur Heart J 2013; 34: 3478 -3490.
Heterozygous familial hypercholesterolaemia (FH) Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Pathophysiology & genetics Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Pathophysiology of heterozygous familial hypercholesterolaemia. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490 Elevated LDL cholesterol Atherosclerosis Coronary heart disease Liver with only 50% functional LDL receptors Myocardial infarction Angina pectoris Mutations in LDL receptor, apolipoprotein. B or PCSK 9 Heterozygous familial hypercholesterolaemia
LDL cholesterol burden in individuals with or without familial hypercholesterolaemia as a function of the age of initiation of statin therapy. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Coronary disease & death before age 20 Homozygous FH 12. 5 yrs Untreated coronary disease before age 55/60 Heterozygous FH Threshold for CHD 53 yrs 35 yrs Female sex 48 yrs 55 yr Start high dose statin Start low dose statin Smoking Hypertension Diabetes Triglycerides HDL-C Lipoprotein(a) Without FH Age in years Adapted from Steve Humphries 2013
Underdiagnosis & undertreatment Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Estimated per cent of individuals diagnosed with familial hypercholesterolaemia in different countries/territories, as a fraction of those theoretically predicted based on a frequency of 1/500 in the general population. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Number of FH (estimated based on 1/500) Diagnosed FH (estimated) 33, 300 Netherlands 71% 9, 900 Norway 43% 600 Iceland 19% 15, 600 Switzerland 13% 123, 600 UK 12% 92, 200 Spain 6% 22, 200 Belgium 4% 10, 900 Slovak Republic 4% 11, 100 Denmark 4% 100, 000 South Africa 3% 45, 000 Australia 1% 14, 100 Hong Kong 1% 130, 900 France 1% 46, 300 Taiwan <1% Nordestgaard et al. Eur 121, 000 Italy <1% Heart J 2013; 34: 3478 -3490 5, 700 Oman <1% 621, 200 USA <1% ~ 200 countries or 68, 600 Canada <1% 254, 800 Japan <1% territories in the World 34, 300 Chile <1% Numbers from Livingston, 381, 500 Brazil <1% Descamps & Humphries 214, 900 Mexico <1% 0 25 50 75 100 Diagnosed FH (estimated), % of estimated number in country
Prevalence of definite or probable familial hypercholesterolaemia according to Dutch Lipid Clinic Network Criteria in the Copenhagen General Population Study by 20 -year age groups and by gender. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Dutch Lipid Clinic Network criteria: Definite or probable FH Screening 69, 000 persons from the Copenhagen General Population Study Adapted from Benn et al J Clin Endocrin Metab 2012; 97: 3956 -3964
Estimated millions of individuals worldwide with familial hypercholesterolaemia by WHO regions and by income groups. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
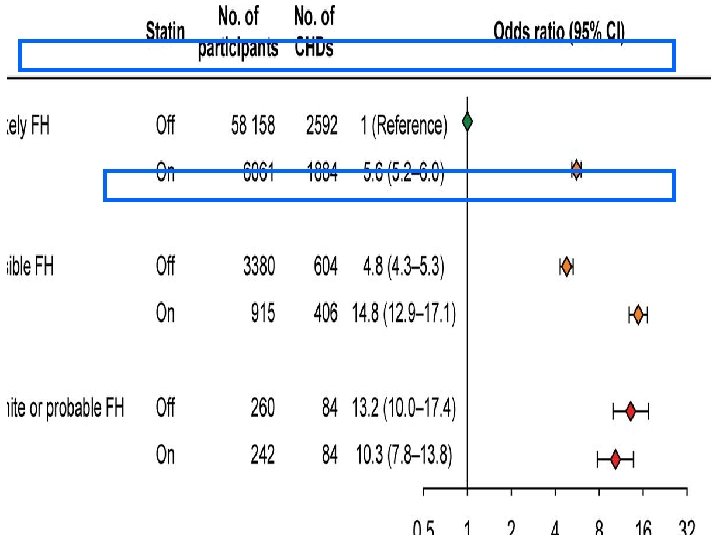
Risk of coronary heart disease as a function of the Dutch Lipid Clinic Network Criteria for a diagnosis of familial hypercholesterolaemia in individuals on or off statin from the general population. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Whom to screen: how to find index cases? Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
We recommend: children, adults, and families should be screened for FH if • • • Family member presents with FH P-cholesterol in adult ≥ 8 mmol/L (≥ 310 mg/d. L) P-cholesterol in child ≥ 6 mmol/L (≥ 230 mg/d. L) Premature CHD Tendon xanthomas Sudden premature cardiac death Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Family pedigree Man Woman FH Death 76 yrs No CHD LDL 3. 8 mmol/L Age 78 yrs CHD 58 yrs LDL 7. 4 mmol/L Index case: start of cascade screening FH Age 50 yrs No CHD LDL 3. 3 mmol/L Age 48 yrs CHD 48 yrs LDL 8. 3 mmol/L Age 47 yrs No CHD LDL 2. 4 mmol/L FH Age 18 yrs LDL 2. 2 mmol/L Age 15 yrs LDL 6. 1 mmol/L Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490 FH Age 8 yrs 5. 6 mmol/L LDL
DUTCH FH CRITERIA
Clinical diagnosis versus mutation diagnosis Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Overlap of clinical and mutation diagnosis of heterozygous familial hypercholesterolaemia. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Mutation without clinical diagnosis Mutation diagnosis Clinical diagnosis without mutation Patient: treat LDL Family: monitor LDL & consider treatment Patient: treat LDL Family: mutation test, monitor LDL, & consider treatment Patient: monitor LDL & consider treatment Family: monitor LDL & consider treatment Adapted from Luis Masana
Cascade screening preferred method Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Pedigree of a family with familial hypercholesterolaemia. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Family pedigree Man Woman FH Death 76 yrs No CHD LDL 3. 8 mmol/L Age 78 yrs CHD 58 yrs LDL 7. 4 mmol/L Index case: start of cascade screening FH Age 50 yrs No CHD LDL 3. 3 mmol/L Age 48 yrs CHD 48 yrs LDL 8. 3 mmol/L Age 47 yrs No CHD LDL 2. 4 mmol/L FH Age 18 yrs LDL 2. 2 mmol/L Age 15 yrs LDL 6. 1 mmol/L Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490 FH Age 8 yrs 5. 6 mmol/L LDL
LDL cholesterol targets: (heterozygous & homozygous FH) • <3. 5 mmol/L(<135 mg/d. L) for children • <2. 5 mmol/L(<100 mg/d. L) for adults • <1. 8 mmol/L(<70 mg/d. L) for adults with known CHD or diabetes Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
LDL lowering treatment Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Based on a consensus of • opinions of experts • small studies, retrospective studies, and registries However • effect of LDL cholesterol lowering in individuals without FH based on: randomised trials and meta-analyses Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Kaplan–Meier curve estimates of cumulative CHD-free survival among individuals with familial hypercholesterolaemia according to statin treatment (P < 0. 001 for difference). Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Adapted from Vermissen et al. BMJ 2008; 337: a 2423
In addition to lifestyle and dietary counselling, treatment priorities are Children (from age 8 -10): 1. Statin 2. Ezetimibe 3. Bile acid binding resin 4. Lipoprotein apheresis in homozygotes Adults: 1. Maximal potent statin dose 2. Ezetimibe 3. Bile acid binding resins 4. Lipoprotein apheresis in homozygotes & treatment-resistant heterozygotes with CHD Nordestgaard et al. Eur Heart J 2013; 34: 3478 -3490
Summary of diagnostic and treatment strategies. Nordestgaard B G et al. Eur Heart J 2013; 34: 3478 -3490 © The Author 2013. Published by Oxford University Press on behalf of the European Society of Cardiology.
Disclosures Supported by unrestricted educational grants to EAS from Amgen, Aegerion, Astra. Zeneca, Genzyme, Hoffman-La Roche, Kowa Europe, Novartis, and Sanofi-Aventis/Regeneron. These companies were not present at the Consensus Panel meetings, had no role in the design or content of the Consensus Statement, and had no right to approve or disapprove the final document. Eur Heart J 2013; 34: 3478 -3490.