Erythropoiesis RBC production Hemoglobin heme globin Heme a

Erythropoiesis • RBC production • Hemoglobin = heme + globin • Heme = a porphyrin ring + an iron atom

Iron • Critical element of cell function • Free iron : highly toxic – Transferrin, ferritin, hemosiderin • Carry O 2 : hemoglobin, myoglobin • Iron containing enzyme : cytochrome system in mitochodria • Iron deficiency : – Decreased Hb synthesis : anemia, hypoxia – Impaired cell function : electron transport, energy
 Male(80 kg) Female(60 kg) Hemoglobin Myoglobin/enzyme Transferrin iron")
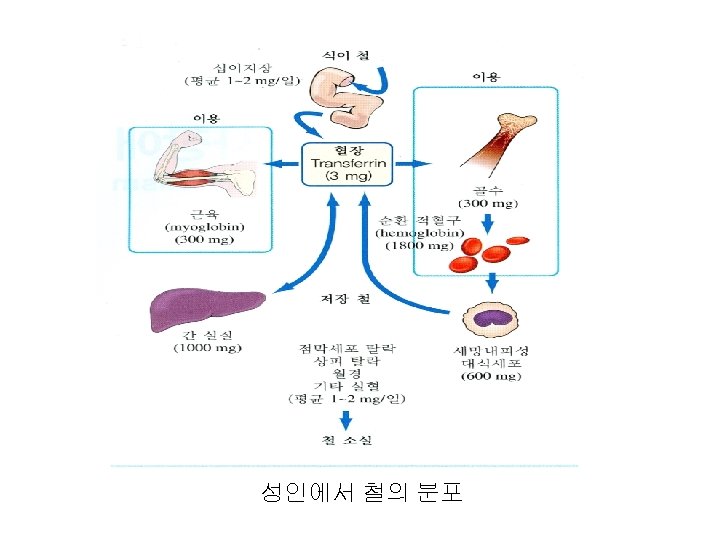
Body iron distribution Iron content (mg) Male(80 kg) Female(60 kg) Hemoglobin Myoglobin/enzyme Transferrin iron Iron stores 2, 500 3 600 – 1, 000 1, 700 3 0 - 300

Iron cycle • Gain : absorption – diet, medicine • Loss : the loss of epithelial cells from the skin, gut, and genitourinary tract blood loss (via gastrointestinal bleeding, menses, or other forms of bleeding) and • Male : 1 mg/d ; Female : 1. 4 mg/d • RBC : 1 mg/m. L • Daily 0. 8 – 1% destruction • Fe turnover : 16 – 20 mg/day

Iron absorption • Proximal small intestine • Stomach : acidic content • Gut cell : DMT-1(divalent metal transporter-1) --- ferritin --ferroportin (negatively controlled by hepcidin) • Erythroid hyperplasia : low hepcidin

Hepcidin • The central regulator of iron absorption, plasma iron levels, and iron distribution • Hepatocyte, macrophage, adipocyte • Inhibit iron flows into plasma from macrophage, duodenal enterocyte, hepatocyte • Bind to the ferroportin (major entryway for iron into plasma) and causing its degradation • Hepcidin production is regulated by iron and erythropoietic activity • hepcidin levels are elevated in a range of inflammatory disease including rheumatologic diseases, inflammatory bowel disease, a variety of infections, critical illness, and malignancies


Nutritional Iron • • • 6 mg/ 1, 000 calories Red meat M : 6 mg – 15% absorption F : 11 mg – 12% Iron deficiency : – meat-containing diet iron : 20% absorption – Vegetarian diet iron : 5 – 10% – Phytates and phosphates reduce absorption

Food iron absorption • Compare to ferrous sulfate • • Iron in vegetables : Egg iron : Liver iron : Heme iron : 1/20 1/8 1/2 - 2/3

Increased iron requirement • • • Infant Children Adolescent Pregnancy : last trimesters : 5 -6 mg Increased erythropoiesis

Anemia classification • Etiologic – Excessive destruction or loss • Blood loss : acute, chronic • Hemolysis – Inadequate production • Nutritional • Marrow failure • Others • Morhologic – Macrocytic : • megaloblastic • nonmegaloblastic – Normochromic normocytic – Hypochromic microcytic

normocytic normochromic hypochromic microcytic

Iron deficiency anemia • One of the most prevalent forms of malnutrition • Globally 50% of anemia • 841, 000 deaths annually • Africa and part of Asia : 71% • North America : 1. 4%
,")
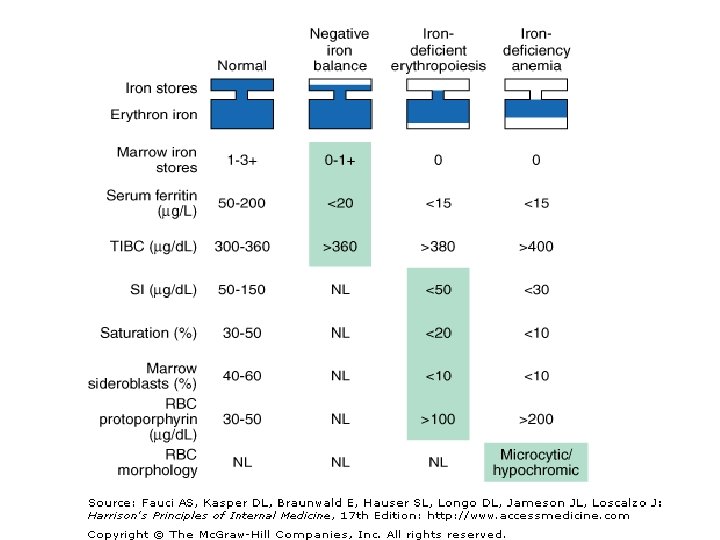
Stages of iron deficiency • Negative iron balance : blood loss(10 -20 m. L/day), pregnancy, rapid growth spurt, inadequate dietay iron • Iron-deficient erythropoiesis : microcytic cells, hypochromic reticulocytes • Iron-deficiency anemia
 Women’s health Pregnancy/breast feeding Menstrual blood losses Chronic blood")
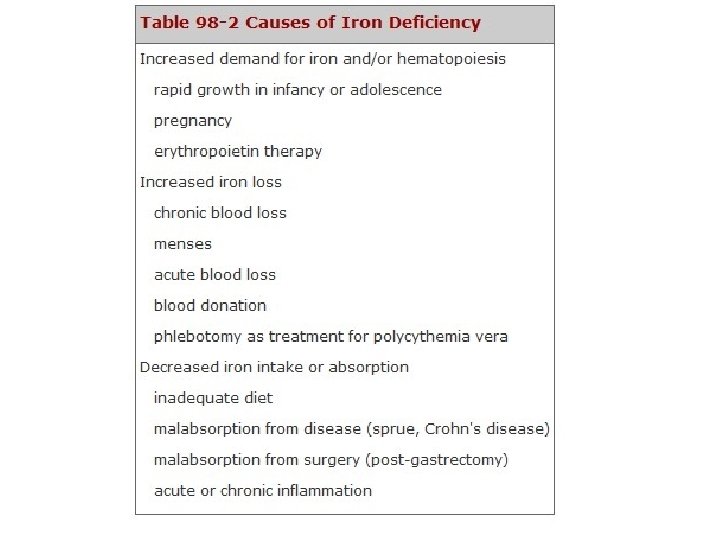
Absolute iron deficiency Dietary (growth/development) Women’s health Pregnancy/breast feeding Menstrual blood losses Chronic blood loss Blood donation Nonsteroidal anti-inflammatory drugs (NSAIDs) Gastrointestinal neoplasms Gastrointestinal parasites (developing countries) Decreased iron absorption Celiac disease Helicobacter pylori infection Autoimmune atrophic gastritis Functional iron deficiency ESA therapy

Iron-sequestration syndromes Anemia of chronic disease/inflammation Autoimmune diseases Infections Malignancies Chronic kidney disease Hepcidin-producing adenomas Iron refractory iron deficiency anemia (IRIDA) Copper deficiency Molecular defects in iron transport, recycling, and utilization Divalent metal transporter 1 (DMT 1) mutations Hypotransferrinemia Ferroportin disease Aceruloplasminemia Hereditary sideroblastic anemias (ALAS 2 mutations) Heme oxygenase deficiency

Clinical presentation of iron deficiency • Signs of anemia – Fatigue – Pallor – Reduced exercise capacity • Cheilosis • Koilonychia
 / Total iron-binding capacity(TIBC) : 50 -150/300 -360")
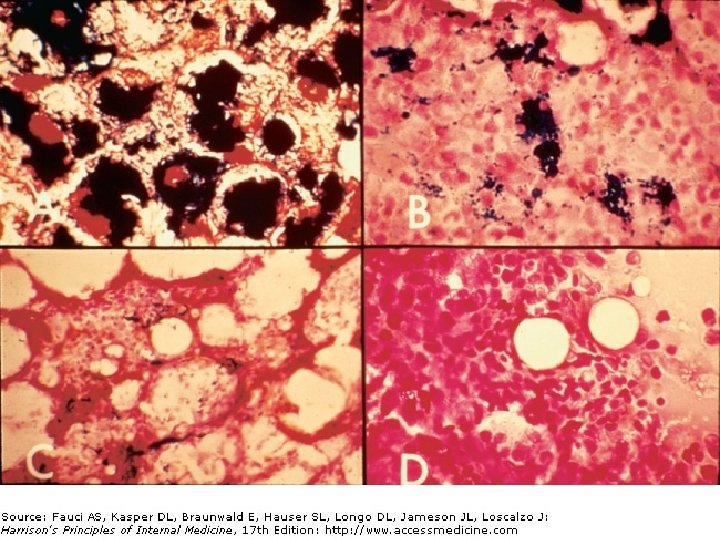
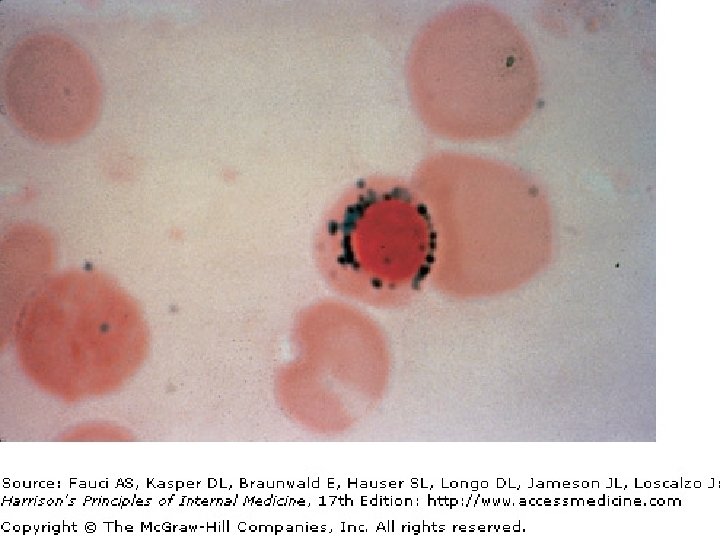
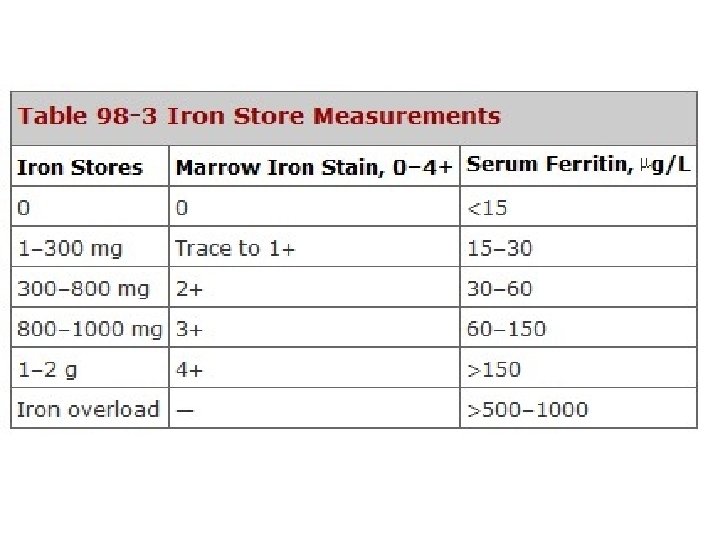
Laboratory iron studies • Serum iron(SI) / Total iron-binding capacity(TIBC) : 50 -150/300 -360 µg/d. L (N) • Serum ferritin : < 15 µg/L • Bone Marrow iron stores : stainable iron, sideroblast, ringed sideroblast (MDS) • • Red cell protoporhyrin levels : > 100 µg/d. L Soluble transferrin receptor (s. Tf. R) : 4 -9 µg/L (N) Percent hypochromic red cell (% Hypo) Hepcidin

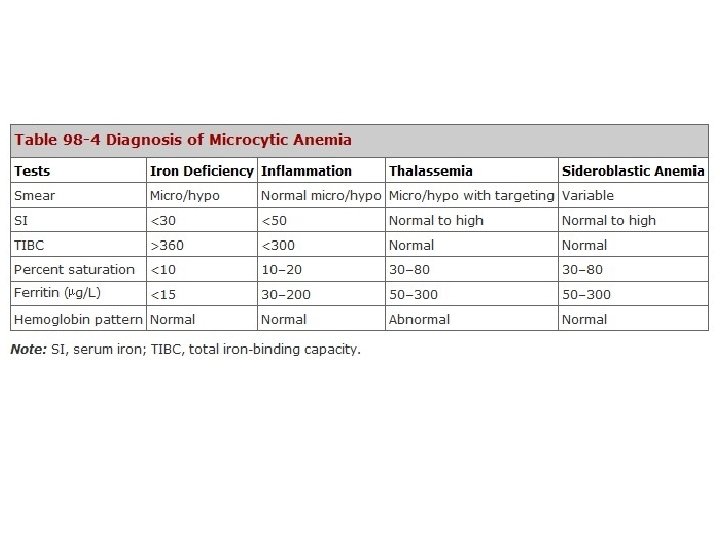
Differential Diagnosis Hypochromic microcytic anemia – Thalassemia – Anemia of chronic inflammation – Myelodysplastic syndrome

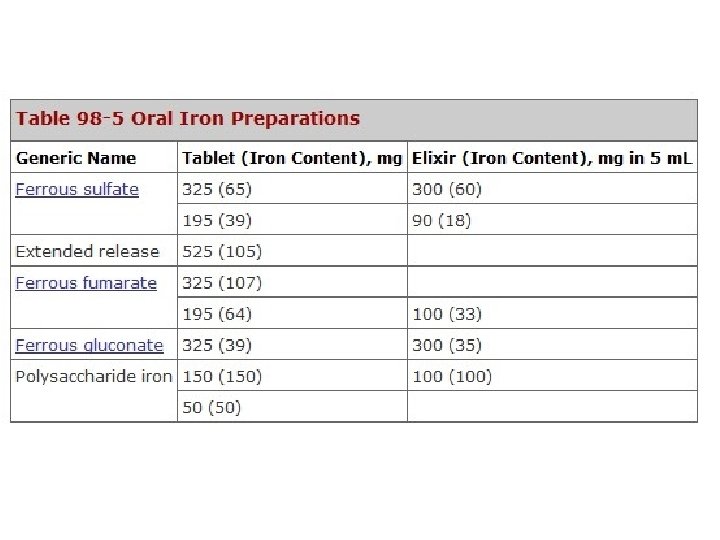
Treatment of iron-deficiency anemia • • Diet : heme iron RBC transfusion Oral iron therapy Parenteral iron therapy – Iron dextran – Sodium ferric gluconate – Iron sucrose – Ferric chloride
 X 2. 3 X (15 –")
Amount of iron needed Ganzoni’s fomula : BW(kg) X 2. 3 X (15 – pt’s Hb, g/d. L) + 500 or 1, 000 mg (for stores)

Parenteral iron therapy • • Unable to tolerate oral iron Absorbtion defect Whose need are relatively acute Epo therapy • Iron dextran : severe side effect Sodium ferric gluconate Iron sucrose Ferric chloride
 • Ferrous sulfate – Feroba-You : 256 mg (80 mg) /")
Iron prep. (본원) • Ferrous sulfate – Feroba-You : 256 mg (80 mg) / tab • Iron acetyl-transferrin hydroglycerin – Bolgre Soln : 2 m. L (40 mg) / 15 m. L • Iron protein succinylate – Hemo-Q : 800 mg (40 mg) / 15 m. L • Ferric chloride – Blutal : 197 mg (40 mg) / 10 m. L Amp

1 st Case 25세, 여자; 주소: 창백한 피부 • P. I. : 서서히 시작된 운동시 호흡곤란, 불규칙한 월경, 채식 위주로 식사 • CBC : RBC : 3, 200, 000/u. L, Hb : 7. 4 g/d. L, Hct : 23% MCV : 72 f. L(81 -99), MCH : 23. 1 pg/cell(27 -31), MCHC : 32. 1 g/d. L(33 -37) WBC : 8, 500/u. L, Platelet : 485, 000/u. L • Peripheral blood smear : Hypochromic, microcytic, anisocytosis (++), pikilocytosis (+) • Chemistry : serum Fe : 26 ug/d. L, TIBC : 460 ug/d. L Ferritin : 15 ng/m. L

Normocytic normochromic Hypochromic microcytic

진단 • Hypochromic, microcytic anemia – Fe deficience – Inflammation – Thalassemia – Sideroblastic • Fe deficiency anemia – Causes
, diet (+), demend (? )")
진단 • 1 st case : blood loss (mense), diet (+), demend (? ) • 2 nd case: blood loss (mense), diet (? ), demend (-): gynecological problem • 3 rd case : blood loss (-), diet (+), demend (-) : absorption (gastrectomy) • 4 th case : blood loss (? ), diet (-), demend (-) : cause of blood loss

Treatments of Cases • 1 st Case : • 2 nd Case : • 3 rd Case : • 4 th Case :

Iron-sequestration syndromes Anemia of chronic disease/inflammation Autoimmune diseases Infections Malignancies Chronic kidney disease Hepcidin-producing adenomas Iron refractory iron deficiency anemia (IRIDA) Copper deficiency Molecular defects in iron transport, recycling, and utilization Divalent metal transporter 1 (DMT 1) mutations Hypotransferrinemia Ferroportin disease Aceruloplasminemia Hereditary sideroblastic anemias (ALAS 2 mutations) Heme oxygenase deficiency

Anemia of Chronic Disorders • • • Anemia Anemia of Chronic Inflammation of Uremia due to Endocrine Failure of Liver Disease of Protein Deprivation

진단 • Unequivocal diagnosisis often difficult • Diagnosis of exclusion (infiltration by tumor, fibrosis, or infection, MDS) • Dx with reticulocyte, Fe, TIBC, serum ferritin, in systemic illness • R/O nutritional def, hemolysis, sequestration. BM usually not helpful • DDx of IDA (serum ferritin? , serum transferrin receptor? )

Anemia of Hypometabolism: 산소요구량 감소에 의한 적혈구조혈 감소 • Anemia due to Endocrine Failure – hypothyroidism, Addison'sdisease, hypogonadism, panhypopituitarism, hyperparathyroidism – Addison'sdisease 치료시 plama volume 감소가 교정되면서 잠시 혈색소 치는 감소하기도 한다. • Anemia of Liver Disease – – – • Anemia of Protein Deprivation: – • Cholesterol 증가: Burrcell, stomatocyte RBC 수명 단축, 골수 보상 활동 저하 alcohol: 골수에 독성, 엽산결핍, 철결핍(위장관 출혈, 식이 부족) volume depletion으로 masking 가능 치료: – – 수혈: 증상에 따라 결정. CV or pulm disease, elderly , risk of transfusion Erythropoietin(EPO) w/o iron: 4 -6주에 Hb 10 -12 g/d. L 도달. Decreased response: infection, iron del[etion, Al toxicity, hyperparathyroidism Long actin EPO
- Slides: 50