Erythrocyte metabolism Alice Skoumalov Erythrocytes deliver oxygen to

Erythrocyte metabolism Alice Skoumalová

Erythrocytes Ø deliver oxygen to body tissues and remove carbon dioxide and protons Ø biconcave 7. 7μm Ø lack cell organelles Ø 120 days Ø women 4, 2 -5, 4 million/μl, men 4, 6 -6, 2 million/μl
 50% proteins SDS-PAGE: separation of proteins")
The erythrocyte membrane 50% lipid bilayer (phospholipids, cholesterol) 50% proteins SDS-PAGE: separation of proteins (band 1 -7) isolation and analysis (10 main proteins) Integral: Anion exchanger protein, Glycophorin A, B, C Peripheral: Spectrin, Ankyrin, Actin
")
Spectrin: the most prominent component (two isoforms α, β; a tetramer; a meshwork ) fixed to the membrane- ankyrin binding sites for several other proteins (glycophorin C, actin, band 4. 1, adducin) This organization keeps the erythrocyte shape.

Haemoglobin 4 protein chains + 4 haem groups

Haem

Movements of the heme and the F helix during the T – R transition in hemoglobin:

Hemoglobin saturation curves:

Hemoglobin autooxidation • • O 2 binds Fe 2+ - an intermediate structure - an electron is delocalized between the iron ion and the O 2 the side effect - every so often a molecule of oxyhaemoglobin undergoes decomposition and release superoxide Hem - Fe 2+- O 2 • Hem - Fe 3+ - O 2 • - 3% of the haemoglobin undergoes oxidation every day Methemoglobin (Fe 3+) is unable to bind O 2 (methaemoglobin reductase)

Erythrocyte exceptions They lack organelles • no ATP production in oxidative phosphorylation • no ability to replace damaged lipids and proteins (low metabolic activities, with no ability to synthesize new proteins or lipids) Free radicals exposure • haemoglobin autoxidation (O 2 • - release) • a cell membrane rich in polyunsaturated fatty acids (susceptible to lipid peroxidation) • deformation in tiny capillaries; catalytic ions leakage (cause of lipid peroxidation)

Erythrocyte metabolism • Glucose as a source of energy • Glycolysis generates ATP and 2, 3 -bisphoglycerate • The pentose phosphate pathway produces NADPH • Glutathione synthesis- the antioxidant defence system
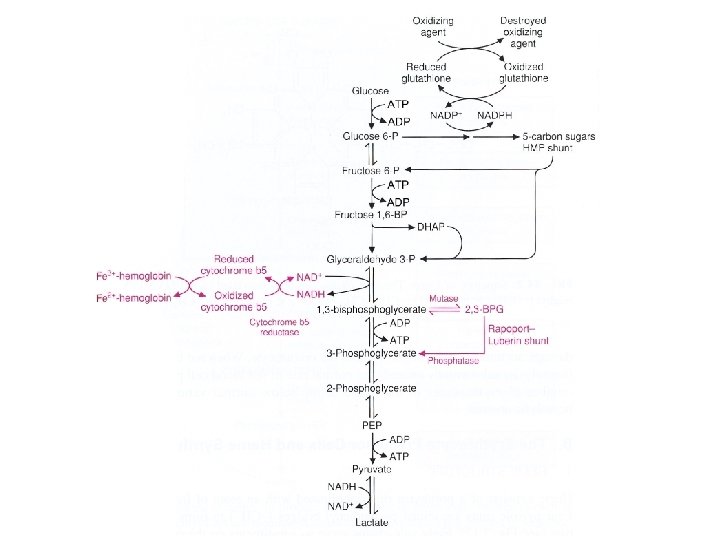

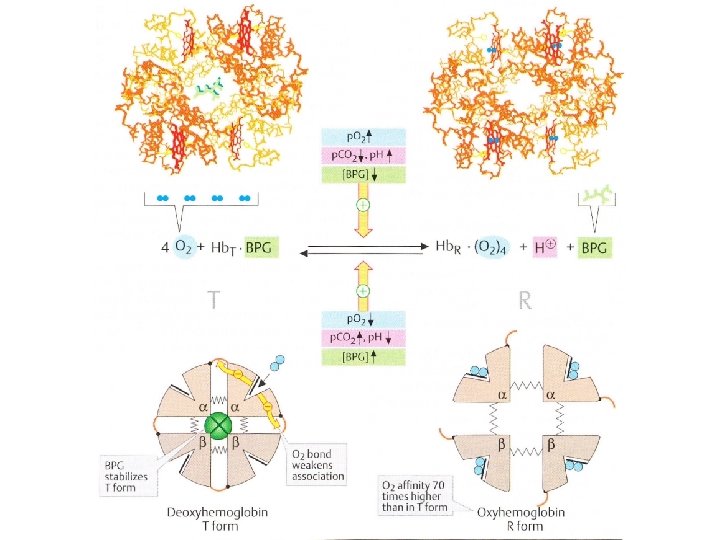
Glucose- source of energy Glucose transporter: • • • integral membrane protein (12 membrane-spanning helices) a channel for the glucose transport insulin-independent transporter Glycolysis in erythrocytes 1. Source of ATP • • Lactate- the end product Cover energy requirement 2. Generate 2, 3 -bisphoglycerate (2, 3 -BPG) • • a major reaction pathway for the consumption of glucose in erythrocytes the specific binding of 2, 3 -BPG to deoxyhemoglobin decreases the oxygen affinity of hemoglobin and facilites oxygen release in tissues

2, 3 -bisphoglycerate • Allosteric effector of haemoglobin: – binds to deoxyhaemoglobin (a central cavity capable of binding 2, 3 BPG) – decreases haemoglobin‘s O 2 affinity • Clinical aspects: – In people with high-altitude adaptation or smokers the concentration of 2, 3 -BPG in the blood is increased (low oxygen supply) – Fetal haemoglobin has low BPG affinity - the higher O 2 affinity facilitates the transfer of O 2 to the fetus via the placenta

Glutathione synthesis in erythrocytes

Glutathione Elimination of H 2 O 2 and organic hydroperoxides 1. Cofactor for the glutathione peroxidase (removes H 2 O 2 formed in erythrocytes) 2. Involved in ascorbic acid metabolism 3. Prevents protein –SH groups from oxidizing and cross-linking Glutathione peroxidase Gly Cys Gly + R-O-O-H Cys SH + NADPH Glutathione reductase Glu S S Cys + H 2 O Glu Reduced form of glutathione Oxidized form of glutathione (monomer) (dimer, disulphide)

The pentose phosphate pathway in erythrocytes • Generates NADPH - reduction of glutathione (eliminates H 2 O 2 formed in erythrocytes) Clinical apect: • Glucose-6 -phosphate dehydrogenase deficiency – Causes hemolytic anemia (decreased production of NADPH - reduced protection against oxidative stress - haemoglobin oxidation and Heinz bodies formation, membrane lipid peroxidation and hemolysis) – Hemolytic crises are evocated by drugs (primaquine, sulphonamide antibiotics) and foods (broad beans) – The most common enzyme deficiency disease in the world (100 million people)

Oxyhaemoglobin O 2 Superoxide dismutase Haemoglobin Superoxide H 2 O 2 Catalase Methaemoglobin reductase Methaemoglobin Pentose phosphate NADP+ pathway Glutathione reductase NADPH ½ O 2+H 2 O GSH Glutathione peroxidase GSSG H 2 O GSH-reduced form; GSSG-oxidized form of glutathione
 • large number of haemoglobin mutations,")
Haemoglobinopathy • abnormal structure of the haemoglobin (mutation) • large number of haemoglobin mutations, a fraction has deleterious effects • sickling, change in O 2 affinity, heme loss or dissociation of tetramer • haemoglobin M and S, and thalassemias Haemoglobin M • replacement of the histidine (E 8 or F 7) in α or β-chain by the tyrosine • the iron in the heme group is in the Fe 3+ state (methaemoglobin) stabilized by the tyrosine • methaemoglobin can not bind oxygen Thalassemias • genetic defects- α or β-chains are not produced (α or β-thalassemia)
 • • Causes a sickle-cell anemia Erythrocytes adopt an elongated sickle")
Haemoglobin S (sickle-cell) • • Causes a sickle-cell anemia Erythrocytes adopt an elongated sickle shape due to the aggregation of the haemoglobin S

• Replacing Glu with the less polar amino acid Val - forming „an adhesive region“ of the β chain • Hg proteins aggregate into a long rodlike helical fiber Cross section

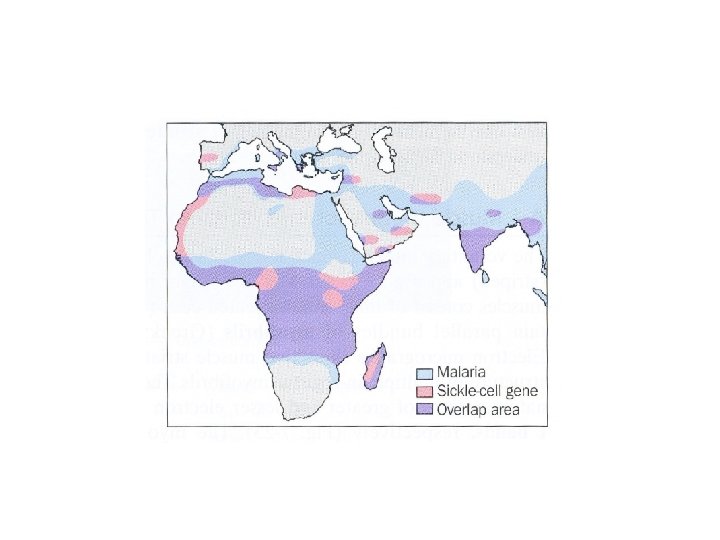
• • • Red blood cells adopt a sickle shape in a consequence of the forming haemoglobin S fibers The high incidence of sickle-cell disease coincides with a high incidence of malaria Individuals heterozygous in haemoglobin S have a higher resistance to malaria; the malarial parasite spends a portion of its life cycle in red cells, and the increased fragility of the sickled cells tends to interrupt this cycle Scanning electron micrograph of a sickled erythrocyte. The haemoglobin S fibers can be seen within the distorted cell. The cell has ruptured and haemoglobin fibers are spilling out.

Hemoglobin switching:
 • • formed by hemoglobin's exposure to high plasma")
Glycosylated haemoglobin (Hb. A 1) • • formed by hemoglobin's exposure to high plasma levels of glucose non-enzymatic glycolysation (glycation)- sugar bonding to a protein normal level Hb. A 1 - 5%; a buildup of Hb. A 1 - increased glucose concentration the Hb. A 1 level is proportional to average blood glucose concentration over previous weeks; in individuals with poorly controlled diabetes, increases in the quantities of these glycated hemoglobins are noted (patients monitoring) Sugar CHO Sugar CH + NH 2 N CH 2 Protein Schiff base Amadori reaction Sugar CH 2 NH CH 2 Protein Glycosylated protein
 The erythrocyte membrane 2) Haemoglobin –O 2 binding 3) Haemoglobin – allosteric")
Summary 1) The erythrocyte membrane 2) Haemoglobin –O 2 binding 3) Haemoglobin – allosteric efectors 4) Free radicals in erythrocytes 5) Metabolic pathways in erythrocytes 6) Haemoglobinopathy 7) Glycosylated haemoglobin

Pictures used in the presentation: Marks´ Basic Medical Biochemistry, A Clinical Approach, third edition, 2009 (M. Lieberman, A. D. Marks) Principles of Biochemistry, 2008, (Voet D, Voet J. G. , and Pratt C. W) Color Atlas of Biochemistry, second edition, 2005 (J. Koolman and K. H. Roehm)
- Slides: 28