ERJ 2015 The risk of tuberculosis in TST

ERJ 2015

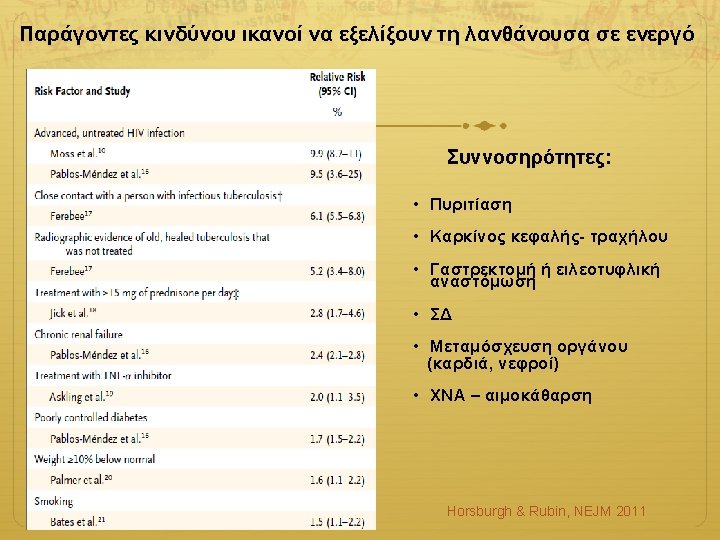
The risk of tuberculosis in TST +ve individuals Am J Epidemiol 1974
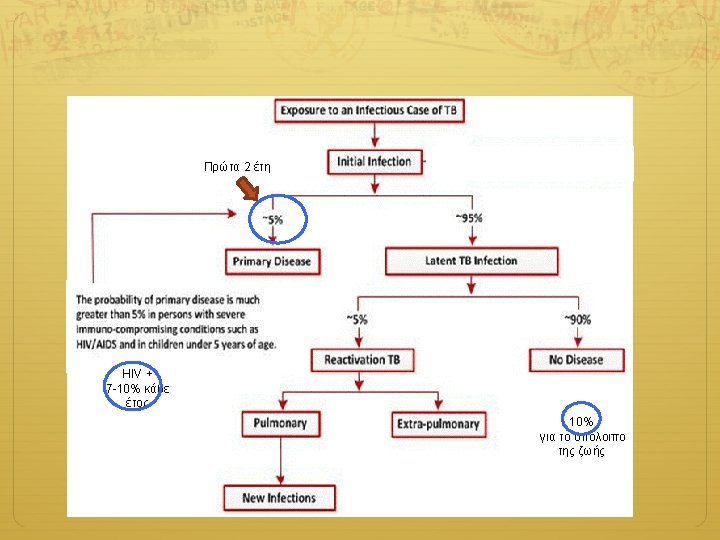

ERJ 2015

Targeted testing LTBI Tx X-ray Inpatient care Medical evaluation and follow-up Non-TB medical services Home evaluation Pharmacy Laboratory Social HIV testing and Interpreter/ services counseling Occupational health, translator school, jail, shelter, services Patient LTCF screening Data collection education Coordination of Documentation Epidemiology medical care Contact DOT investigation and Surveillance Housing Isolation, detention Guidelines Clinical Services Case Management Follow-up/treatment of contacts evaluation & QA, QI for case planning management Consultation on Data for local, state, national Training difficult cases surveillance reports Federal TB Control Program National surveillance Technical assistance Training Funding Outbreak Data analysis Investigation Program State TB Control Program Funding Information State statutes, for public regulations, policies, guidelines VDH/DDP/TB Jan 2007

LTBI vs. Pulmonary TB Disease Latent TB Infection Pulmonary TB Disease Positive TST or IGRA TST or IGRA result is usually positive Chest radiograph is normal usually abnormal

LTBI vs. Pulmonary TB Disease Latent TB Infection No symptoms or physical findings suggestive of TB If done, respiratory specimens are smear negative Pulmonary TB Disease Symptoms may include one or more of the following: fever, cough, night sweats, weight loss, fatigue, hemoptysis, decreased appetite Respiratory specimens are usually culture and culture positive (smear positive in 50% of patients )
 Eναιώρημα εξασθενημένων στελεχών του βακίλλου φυματίωσης M. bovis")
Εμβόλιο φυματίωσης Βacillus Calmette-Guerin Vaccine (BCG) Eναιώρημα εξασθενημένων στελεχών του βακίλλου φυματίωσης M. bovis Ενήλικες & Παιδιά >1 έτους 0, 1 ml Βρέφη <1 έτους 0, 05 ml USA: PPD-S 0, 1 ml contains 5 TU PPD UK: PPD-RT-23 0, 1 ml contains 2 TU PPD ισοδύναμες με τις 5 TU της PPD-S Effect of BCG vaccination against Mycobacterium tuberculosis infection in children: systematic review and meta-analysis BMJ 2014

Thorax 2002

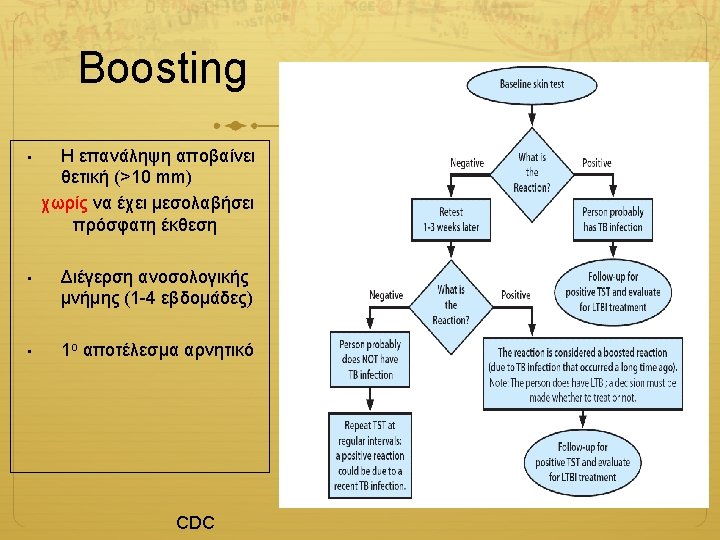
 Positive Negative No treatment Evaluate patient")
Patient with risk factors for LTBI TST (PPD) Positive Negative No treatment Evaluate patient for LTBI testing and treatment regardless of BCG status History/HIV risk, physical exam, chest x-ray Normal Abnormal Refer to TB clinic for evaluation of active TB Candidate for LTBI Treatment Rule out active TB disease before treatment for LTBI Positive Treatment of active TB Negative CDC

Species specificity of ESAT-6 and CFP-10 Tuberculosis complex M tuberculosis M africanum M bovis BCG substrain gothenburg moreau tice tokyo danish glaxo montreal pasteur ESAT-6 CFP-10 + + + - - Environmental strains ESAT-6 CFP-10 M abcessus M avium M branderi M celatum M chelonae M fortuitum M gordonii M intracellulare M kansasii M malmoense M marinum M oenavense M scrofulaceum M smegmatis M szulgai M terrae M vaccae M xenopi + + + -

IGRAs Quantiferon-TB Gold In-Tube Assay ESAT-6, CFP – 10, TB 7. 7 Measure IFN- γ, ELISA T-spot. TB Assay ESAT-6, CFP – 10 Count spots which are related to the number of cells releasing Gamma Interferon.

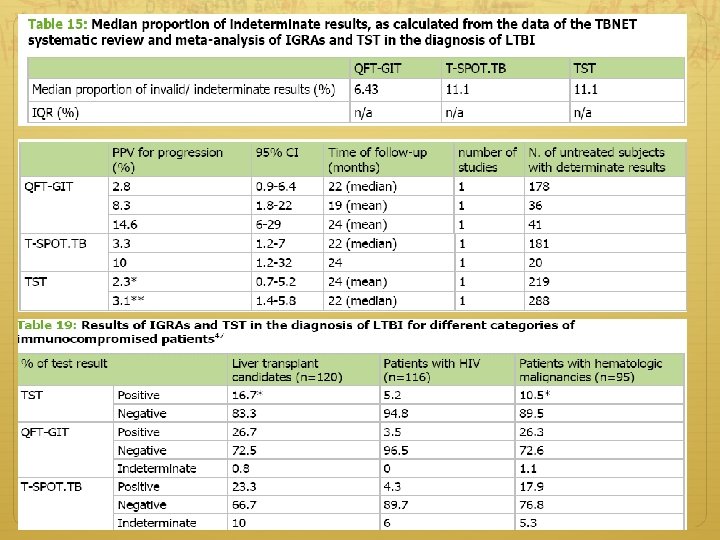
PPV and NPV of the TST and IGRAs for latent tuberculosis Test PPV NPV TST 2. 3 -3. 3 99. 7 QFT-G-IT 2. 8 -14. 3 99. 8 T-Spot. TB 3. 3 -10. 0 97. 8 Diel R et al. Eur Respir J 2011

CDC Canada

CDC Canada
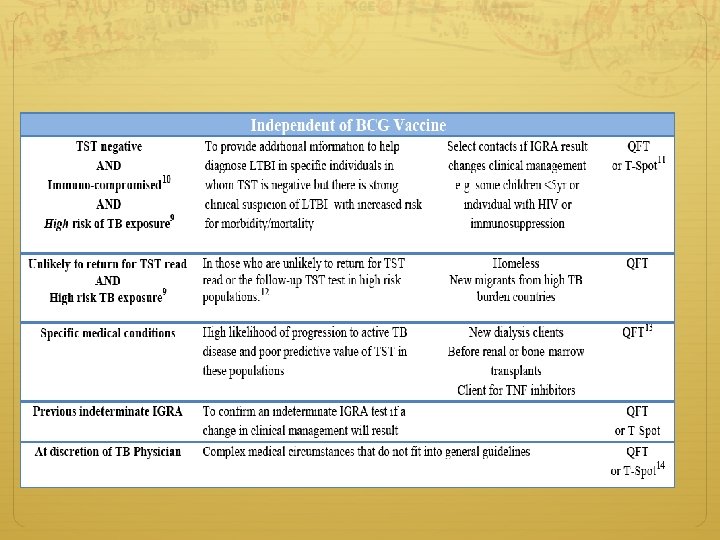

Τι και πότε? Νοr IGRAs - BCG - low rates of return for TST reading - Homeless/IVDA TST - Children <5 Not • Recent contact to case – <8 -10 weeks (like TST) – previous TB – Treatment follow up – LTBI/TB Both is Justifiable* • When 1 st test is neg, but risk for progression is high • When 1 st test is +, but more evidence is needed to encourage compliance • When IGRA is indeterminate, borderline or invalid • If suspect 1 st test is wrong - When other unavailable *PPD may “boost” IGRA response. If you do TST then IGRA, do it within 7 d of TST

TB risk and anti-TNF Agent Adjusted RR Any DMARDs 3. 0 MTX 3. 4 Leflunomide 11. 7 Cyclosporine 3. 8 l Συνήθως τους πρώτους Other 1. 6 6 - 12 μήνες θεραπείας Corticosteroids 2. 5 l κίνδυνος (x 5 - 10) με τους anti-TNF παράγοντες Ανοσοεπαρκείς Aντι-TNF αγωγή Εξω-πνευμονική νόσος 15% 30 -50% Γενικευμένη νόσος 1% 25% Arthritis Rheum. 2009

TB OR NOT TB?

LTBI/ MDR-XDT TB Lack of evidence or guidelines was the main reason for not treating MDR-TB contacts The duration of follow-up was at least 3 years, with a maximum of 6 years Thorax 2009 IJTLD 2010
- Slides: 48