ER Mortality and Morbidity Conference review 2004 10

ER Mortality and Morbidity Conference review 2004 -10 -05 case Speaker : R 2 劉雨欣 Supervisor: VS 陳俊宇醫師 Date: 2011. 06. 15
 Chart No: 4241956 Age:")
¡ 2004. 09. 13 15: 01 (0 hr 00 min) Chart No: 4241956 Age: 82 y/o Gender: female Vital signs: ¡ BT: 37’C; Pulse: 73/min; RR: 20/min; BP: 112/71 cm Hg

Chief complain: Abdominal pain for 1 hour

¡ Present illness ¡ Loose stool 2 days ago, had been to LMD for help, diarrhea seized after medication, mild abdominal pain persist and exacerbate in recent 1 hour Nausea / Vomit : +/+ Fever / Chills : +/+ at home No diarrhea at ER Allergy History NKA

¡ Past History No DM, no HTN 1994. 8 CIN III, s/p ATH + BSO 2003. 10 Admission to GI Ileus, r/o terminal ileum inflammation ¡ CBD dilation ¡ post ERCP pancreatitis ¡ GU ¡ duodenal diverticulum ¡ 2003. 12. 31 ER: Adhesion ileus

2004. 1. 11 ER: ¡ 2004. 1. 26 ER: obstruction ¡ 2004. 2. 25 ER: ileus ¡ 2004. 3. 31 ER: ¡ 2004. 5. 30 ER: impaction ¡ 2004. 6. 23 ER: ¡ FGID Partial intestinal Abdominal pain, r/o ileus, AGE ileus with stool r/o adhesion ileus

¡ Physical Exam: Appearance: ill-looking HEENT: supple Chest: breath sound clear; RHB Abdomen: soft; peri-umbilical tenderness; no muscle guarding; bowel sound: active Extremities: free

What else do you need to know? ¡ ¡ ¡ ¡ CHaracter: sharp? crampy? Dull? Location: RUQ/LUQ, RLQ/LLQ, epigastric/suprapubic Onset: progress/sudden Radiation Intensity Duration: acute or chronic Events associated: Fever/chills, N/V/D/C, Bloody/Tarry stool, Hematuria/dysuria, MC/↑Vaginal discharge

Frequency: persistent/intermittent ¡ Palliative factor ¡ Provocative factor ¡ Past medical/surgery history ¡

PE HEENT: icteric sclera/ pale conjunctiva ¡ Abd: shifting dullness, rebounding pain, Mc. Burney point/Murphy’s sign, Hernia ¡ Skin: veicle/skin rash ¡

What is Your Impression?

7 th tintinalli’s

7 th tintinalli’s

6 th tintinalli’s

Impression ¡ ¡ ¡ ¡ ¡ 1. Adhesion ileus 2. Ischemia bowel disease 3. Hallow organ perforation 4. Cholangitis 5. Pancreatitis 6. AAA rupture/Aortic dissection 7. Diverticulitis 8. PUD 9. AGE
 ¡ Initial order Buscopan 1")
2004. 09. 13 15: 17 (0 hr 16 min) ¡ Initial order Buscopan 1 amp IM stat Check CBC/DC, Na, K, Cr, Amylase, Lipase KUB(supine) IVF: N/S run 100 ml/hr Do you agree with that?

NPO ¡ DC Buscopam and give pain killer ¡ Check Sugar, ALT/ALk-P, Bilirubin, U/A ¡ Arrange Standing CXR (if could) ¡ Perform Bed-side echo ¡

Buscopan-scopolamine ¡ Mechanism of Action: Blocks the action of acetylcholine at parasympathetic sites in smooth muscle, secretory glands and the CNS; increases cardiac output, dries secretions, antagonizes histamine and serotonin; dilates pupils

¡ Contraindications: Hypersensitivity to scopolamine, other belladonna alkaloids, or any component of the formulation; narrow-angle glaucoma; acute hemorrhage; paralytic ileus; tachycardia secondary to cardiac insufficiency; myasthenia gravis


¡ KUB showed: Lumbar spondylosis Mild ileus of abdomen Retention of fecal material in colon

¡ ¡ ¡ ¡ WBC: 18400/cmm RBC : 4. 47 milon/cmm Hg. B: 12. 9 g/d. L Hct: 38. 7 % MCV: 86. 6 umm MCH : 28. 9 pg/Cell MCHC : 33. 3 g/d. L RDW: 13. 6 % Platelet: 178 K/cmm Segment: 87% Lymphocyte: 8% Monocyte: 4% Eosinophil : 1% ¡ ¡ ¡ Cr: 0. 9 mg/d. L Amylase: 79 U/L Lipase: 39 U/L Na: 133. 3 meq/L K: 3. 88 meq/L

¡ ¡ ¡ ¡ ¡ 1. Adhesion ileus more likely 2. Ischemia bowel disease can’t R/o 3. Hallow organ perforation can’t R/o 4. Cholangitis can’t R/o 5. Pancreatitis less likely 6. Diverticulitis can’t R/o 7. AAA rupture/Aortic dissection can’t R/o 8. PUD less likely 9. AGE less likely


¡ ¡ Patient complain persist abdominal pain after the initial treatment. What will you do?
 Demerol 50 mg IM stat")
2004. 09. 13 17: 10 (2 hrs 09 min) Demerol 50 mg IM stat Abdominal CT 迷之聲: (某主治醫師)再次重申,就算是 世界末日也不要在我的班打Demerol

What is Your Impression Now?

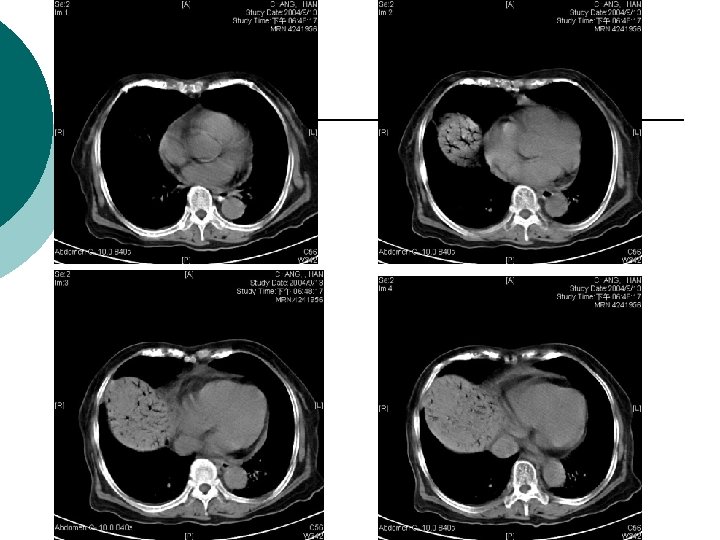
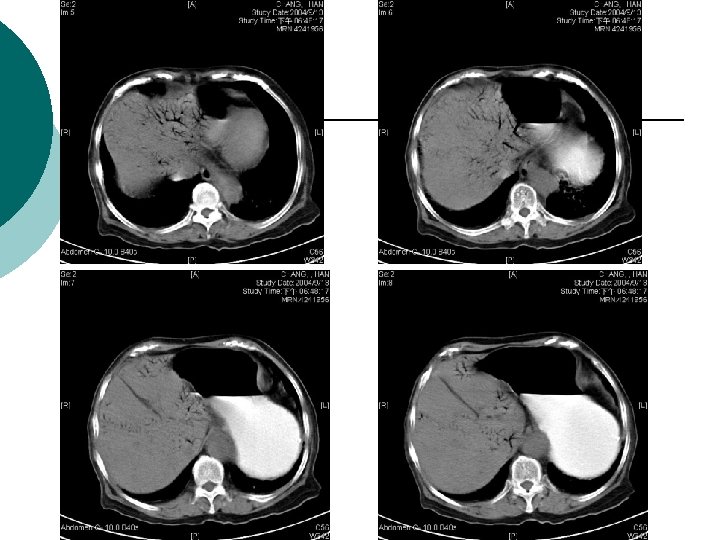
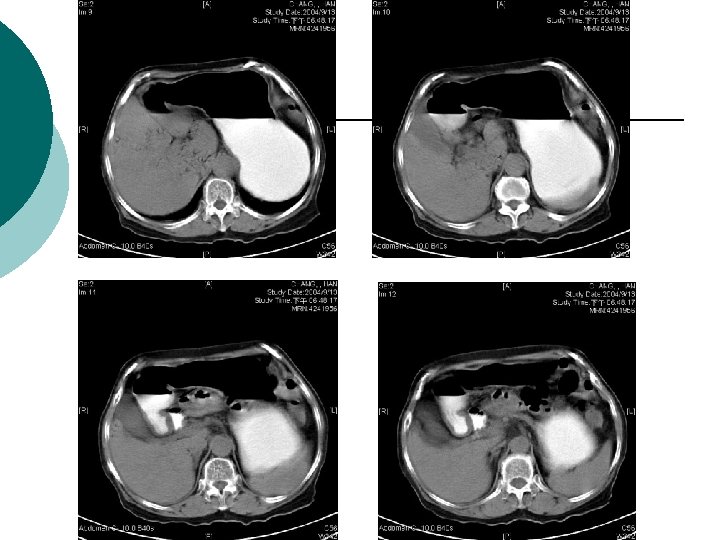
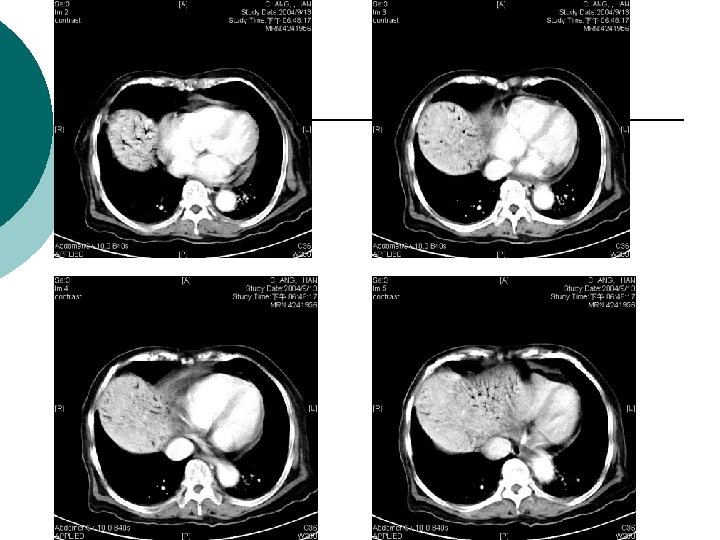
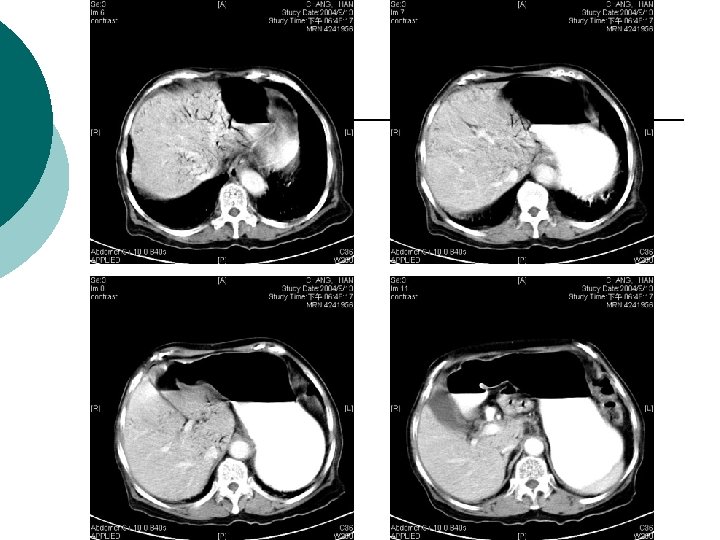
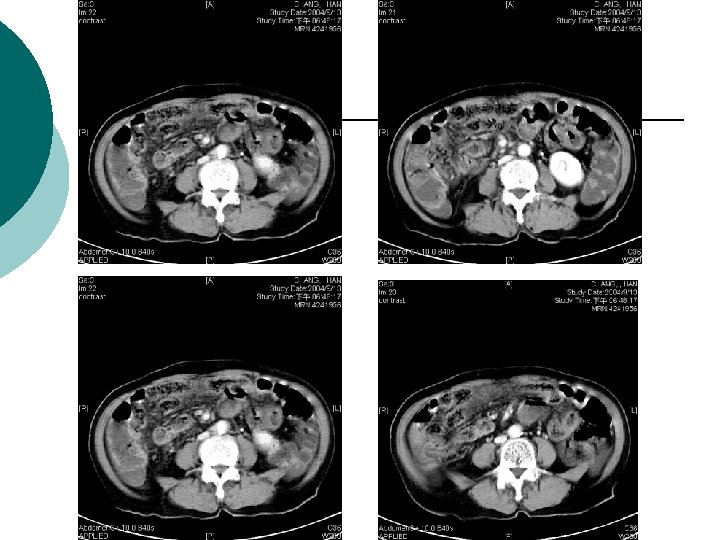
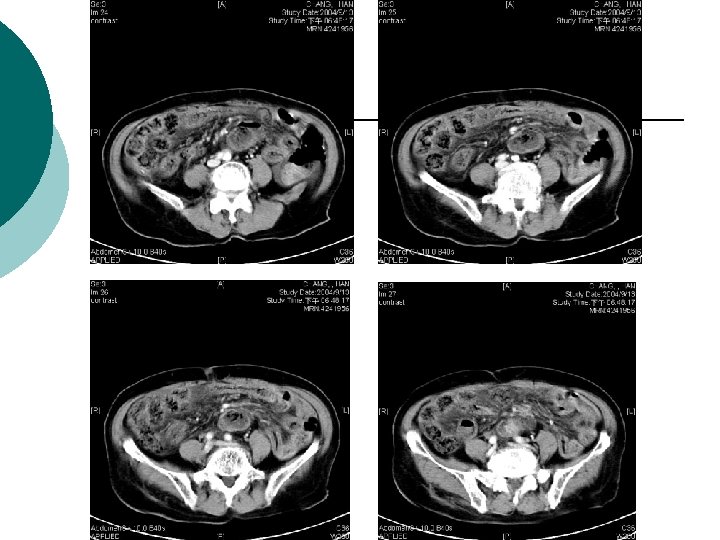
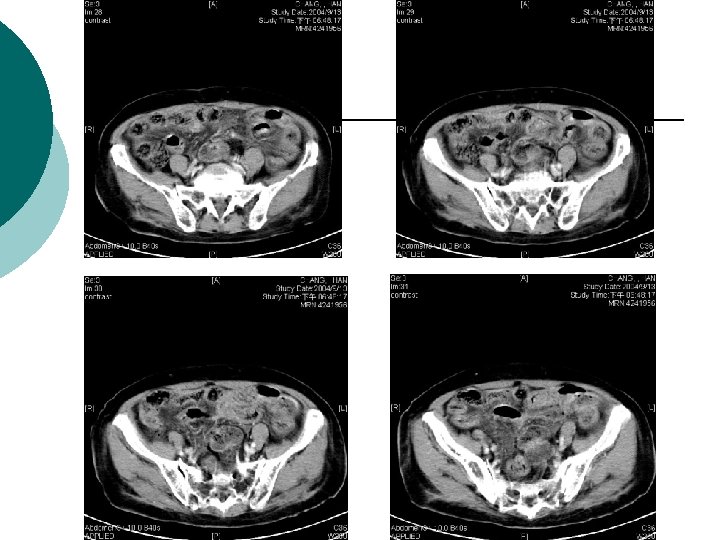
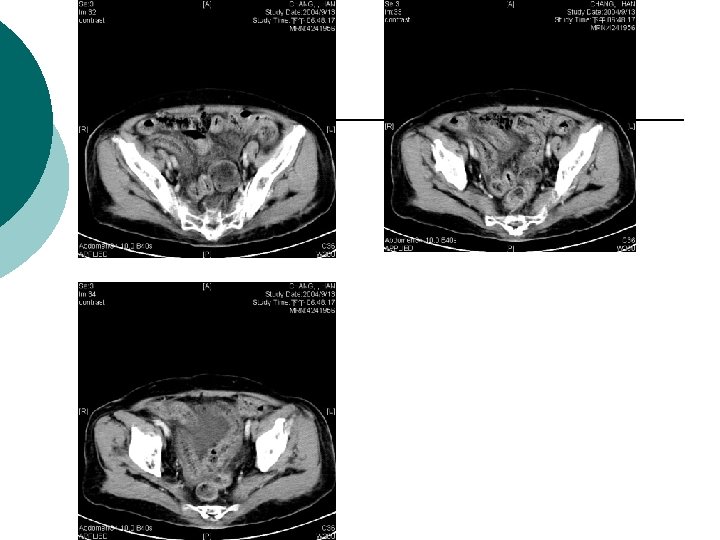
¡ Abdominal CT report: ¡ 1. There is abnormal tree-like air densities in the bil. sides of the liver, air in the portal system is highly compatible. 2. Irregular abnormal wall thickening are noted in the ileum and colon. 3. Possible air densities to be considered in the wall of the ileum. 4. Increased in density in the mesentery is also marked in the right abdomen. Impression: Peritonitis in the abdomen, more on the right side. Necrotizing enterocolitis is highly suspected. DDx: ischemic colitis. Air in the portal system.

What’s your next step?
 Consult GS Impression: Ischemic")
¡ 2004. 09. 13 20: 00 (4 hrs 59 min) Consult GS Impression: Ischemic bowel disease is suspect ¡ Plan: Surgical intervention is indicated ¡ ¡ Family hesitate about OP 2004. 09. 13 21: 30 (6 hrs 29 min) Cefazolin 1 g IV q 8 h and stat Gentamicin 80 mg IVF stat and 60 mg q 12 h Metronidazole 500 mg IVF stat and q 8 h

996 2454 1521 2448 5520 + 371 + 518 + 1580 + 1638 + 1306 + 1244 + 1248 + 5108 1580 3308 中央健保局 collect by Dr. 徐 40
 ¡ 2004. 09. 14")
¡ 2004. 09. 14 0: 51 (9 hrs 50 min) ¡ 2004. 09. 14 1: 26 (10 hrs 25 min) ¡ BT: 36. 9’C; Pulse: 86/min; RR: 18/min; BP: 87/60 cm. Hg N/S challenge 500 ml stat On critical, on EKG and BP monitor Pulse: 79/min; RR: 18/min; BP: 105/62 cm. Hg 2004. 09. 14 2: 05 (11 hrs 04 min) Bloody stool noticed Family agree to received OP

OP Finding ¡ Small bowel and colon: edematous change and congestion no gangrenous poor peristasis and weak pulsation no diverticulum from jejunum to sigmoid colon no palpable mass lesion mesentary lymphadenopathy mild turbid ascites: 150 ml R/O secondary peritonitis

¡ 2004. 09. 27 Discharge under stable condition

Discussion-

Hepatic portal venous gas: Physiopathology, etiology, prognosis and treatment World J Gastroenterol 2009 August 7; 15(29): 3585 -3590
, an ominous radiologic sign, was first described by Wolfe")
Hepatic portal venous gas (HPVG), an ominous radiologic sign, was first described by Wolfe and Evens in infants with necrotizing enterocolitis ¡ Ranging from benign causes to potentially lethal diseases ¡
 escape of gas produced by gasforming organisms in the bowel lumen or")
Mechanism (1) escape of gas produced by gasforming organisms in the bowel lumen or in an abscess which then circulate into the liver or ¡ (2) the presence of gas-forming organisms in the portal venous system with passage of gas into the circulation. ¡

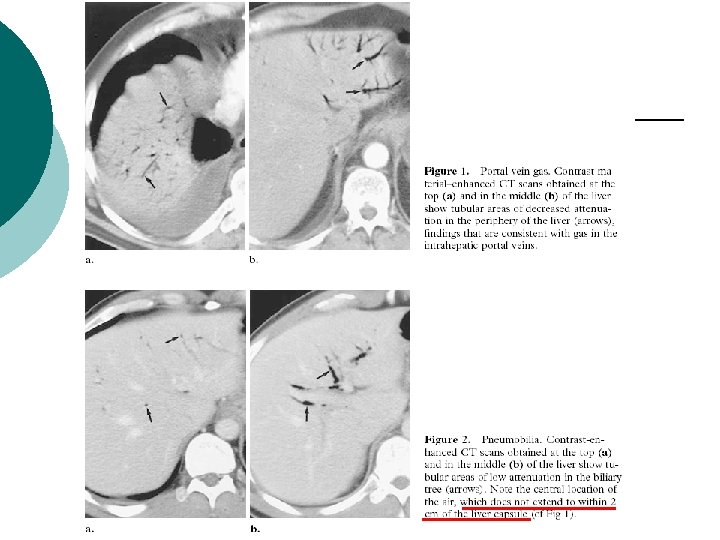
Criteria on CT images: peripheral gas lucencies, which branch out and are noted even within the last 2 cm beneath the liver capsule. ¡ It is crucial to differentiate it from pneumobilia, which is centrally located ¡ Pneumobilia and portal vein gas may coexist ¡

Etiology NEC ¡ **Ischemia bowel ¡ Diverticulitis ¡ Gastric dilatation ¡ Inflammatory bowel disease ¡ Liver transplatation ¡ Chemotherapy ¡

Etiology-other: ¡ ¡ ¡ ¡ Pancreatitis ostructive pyelonephritis after extracorporeal shock wave lithotripsy acute appendicitis Cholangitis gastro-jejunal anastomotic leak after laparoscopic gastric bypass uterine gangrene percutaneous endoscopic gastrostomy tube placement
 ¡ ulcerative colitis (8%) ¡ intra-abdominal abscess (6%) ¡ small bowel")
bowel necrosis (72%) ¡ ulcerative colitis (8%) ¡ intra-abdominal abscess (6%) ¡ small bowel obstruction (3%) ¡ gastric ulcer (3%) ¡ This explains the high mortality rate (56%-90%) reported in association with HPVG ¡ Hepatic--portal venous gas in adults: etiology, pathophysiology and clinical significance. Ann Surg 1978; 187: 281 -287

Management ¡ ¡ ¡ *A radiologic finding of HPVG does not necessarily indicate a severe underlying pathology. *HPVG is not by itself a surgical indication and the treatment depends mainly on the underlying disease. *The prognosis is related to the pathology itself and is not influenced by the presence of HPVG
: 575 -81; discussion 581. Hepatic portal venous gas: the")
Arch Surg. 2009 Jun; 144(6): 575 -81; discussion 581. Hepatic portal venous gas: the ABCs of management

Thanks for your attention!
- Slides: 56