EPILEPSY SLIME TEACHING Dr Rochelle Velho FY 1












 Conservative � Avoid triggers, sleep deprivation, Dx/Alcohol � Counselling lifestyle,")


: Happened last year after crazy golf party and at Guy Fawkes")

 Conservative � Avoid triggers, sleep deprivation, Dx/Alcohol � Counselling parents,")


 � Tailored information and discussion on a person’s")



 - more common in")
 •")
 Major malformations are during first few weeks")
 Vitamin K given last month; � Haemorrhagic disease of newborn more prevalent")
- Slides: 29
EPILEPSY SLIME TEACHING Dr Rochelle Velho FY 1
OVERVIEW Epilepsy Case Based Discussions
EPILEPSY
SEIZURE VS EPILEPSY LINK SEIZURE: A seizure is a temporary disturbance of brain function due to abnormalities in the brain’s electrical circuitry Abnormal metabolic state Other EPILEPSY: Epilepsy is defined as a tendency to recurrent seizures
EPIDEMIOLOGY Common in LEDCs and MEDCs Global prevalence: � 0. 5 -1% - active epilepsy UK: � 65 people probable 1 st seizure every day � Lifetime risk = 5%
AETIOLOGY Metabolic Structural Dx 50% EPILEPSY
ILAE CLINICAL CLASSIFICATION Partial seizures Generalised primary and secondary seizures Unclassifiable seizure See references [2] and [3]
ELEMENTS OF A SEIZURE Prodrome Aura Postictal
CASES DIAGNOSIS AND MANAGEMENT
CASE 1 80 y old female presented to A and E with her son. She was ‘feeling off’ since breakfast and ‘had a funny taste in her mouth’. During lunch, he observed that she LOC, became ‘stiff all over’ and then started ‘jerking all over’ for a 2 -3 minutes. Since the episode his mum has been ‘acting confused and has been drowsy’ (~2 hours). She doesn’t remember.
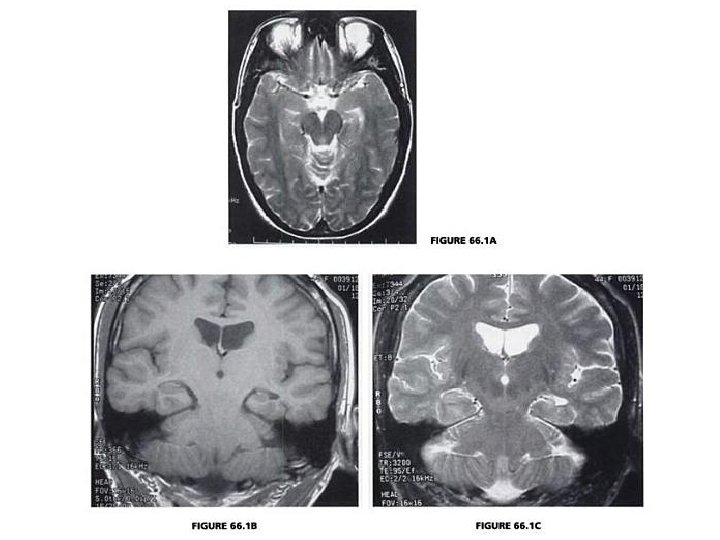
MANAGEMENT Examination �Obs, Cadio, Respiratory, Abdo �Neuro UL, LL and CNs Investigations �Bedside: Bloods, BM, Urine dip, (BCM) �EEG �Radiology: consider CT, MRI for new epileptic ? tumours ? hippocampal sclerosis
? GENERALISED SEIZURE TONIC CLONIC
MANAGEMENT (CONTINUED. . ) Conservative � Avoid triggers, sleep deprivation, Dx/Alcohol � Counselling lifestyle, Driving (DVLA), work Pharmacological � Anti-epileptic drugs Surgical � Neurosurgical resection e. g. medical refractory TLE
PHARMACOLOGICAL MANAGEMENT AED Sodium Valproate Route PO, IV Uses Side-effects/cautions Generalised > Vomiting, Alopecia, Liver toxicity, Pancreatitis/Pancytopenia, Retention of focal fat, Oedema, Ataxia, epilepsies Tremor/Teratogenic, Encephalopathy VALPROATE Carbamazepine PO Leviteracetam PO, IV Generalise/ Focal/Status Epilepticus Phenytoin PO, IV Generalise/ Focal/Status Epilepticus Ataxia, deranged liver function Benzodiazepine PO, IV Generalise/ Focal/Status Epilepticus Sedation, respiratory depression Focal/ Cross-Dx reactivity, nausea, vomiting, bone marrow dysfunction Aggression, deranged liver function
CASE 2 7 y old girl presented to A and E with her teacher. She was in art class this morning and suddenly fell onto the floor, no warning. Then after 10 s she got up and carried on painting. Since the episode, the girl cannot remember. She has a history of not concentrating in class.
MANAGEMENT Hx (mum): Happened last year after crazy golf party and at Guy Fawkes night. Examination �Obs (apyrexial), Cadio, Respiratory, Abdo �Neuro UL, LL and CNs Investigations �Bedside: Bloods, BM, Urine dip, (BCM) �EEG photosensitivity and sleep studies
GENERALISED SEIZURE ABSENCE ?
MANAGEMENT (CONTINUED. . ) Conservative � Avoid triggers, sleep deprivation, Dx/Alcohol � Counselling parents, school, fertility when older Pharmacological � Anti-epileptic drug – 1 st Valproate and 2 nd Lamotrigine
THANK-YOU FOR LISTENING! ANY QUESTIONS? ?
REFERENCES Oxford Handbook 8 th Edition Kumar and Clarke Clinical Medicine The diagnosis and management of the epilepsies in adults and children, national institute Primary care NICE guidelines for epilepsy in adults MRI of the brain, Volume 2 y William G. Bradley, Michael Brant-Zawadzki, Jane Cambray-Forker Crawford P, et al. Best practice guidelines for the management of women with epilepsy. The Women with Epilepsy Guidelines Development Group. Seizure 1999; 8: 201– 17.
SUDDEN UNEXPECTED DEATH IN EPILEPSY (SUDEP) � Tailored information and discussion on a person’s relative risk of SUDEP should be provided. � The risk of SUDEP can be minimised by optimising seizure control and being aware of potential consequences of nocturnal seizures. � Where families/carers have been affected by SUDEP, healthcare professionals should contact them to offer their condolences and referral to bereavement counselling. [2004]
EPILEPSY IN WOMEN
EPILEPSY IN WOMEN Sexuality Fertility Contraception Pregnancy Rare Catamenial epilepsy
SEXUALITY Libido may be affected Minority of epileptic women
FERTILITY < fertility in epileptic women Polycystic ovary syndrome (PCOS) - more common in epileptic women Especially on Sodium Valproate §PCOS (hyperandrogenism syndrome) §Multiple ovarian cysts §Anovulatory cycles §Obesity etc §Cause of female subfertility. .
CONTRACEPTION Contraindicated ×Hormonal forms of contraception affected by enzyme-inducing AEDs (e. g. Phenytoin) • >dose of COCP may be ineffective • POP and Levonorgestrel implants ineffective ×COCP decreases effect of Lamotrigine Recommended üNonenzyme-inducing AEDs (e. g. sodium valproate) do not affect hormonal contraception üNon-hormonal methods (copper coil) and IUD üCan use morning after pill if not on enzyme inducing AED
PREGNANCY Preconception Counselling (5% Risk feotal abnormality) Major malformations are during first few weeks so. . . Highly Teratogenic AEDs changed before conception (Valproate) Folic acid 5 mg/day periconceptially and throughout pregnancy
PREGNANCY (CONTINUED) Vitamin K given last month; � Haemorrhagic disease of newborn more prevalent (AED exposure) Majority – normal vaginal deliveries Review AED dose post-partum Breast feeding encouraged, no AEDs proven to be harmful to baby