Epidemiology of NonCommunicable Diseases Dr Jasim Naeem AlAsadi

Epidemiology of Non-Communicable Diseases Dr. Jasim Naeem Al-Asadi

Definition of NCD l Chronic prolonged illnesses that do not resolve spontaneously, and are rarely cured completely. l They are usually due to individual lifestyle and habits. l One feature common to them is that, when they do not kill immediately they may cause prolonged impairment or disability, requiring care perhaps for the remainder of the affected person’s life.

Non Communicable Diseases Include The Following Major Diseases l l l Cardiovascular diseases Cancer Diabetes Chronic rheumatic & respiratory disease Oral diseases Genetic disorders & genetic predisposition to disease l Mental illnesses l Injuries

Hunting and Gathering l Hunter-gatherers: l Live in conditions that minimize exposure to human infection (small groups of 25 to 50) l Do not degrade environment l Do not enhance environment l Live as nomads: men obtaining food by hunting, women obtained food by gathering l Diet consists of insects, vegetables, fruit

Hunter-gatherer health and disease: l Life was short, death rates were high. l Main causes of death include: accidents, food shortage, parasitic disease, and infections. ¡ TB from ~ 3000 BC ¡ Leprosy from ~500 AD ¡ Syphilis from ~1500 AD l Relationship between food shortage and parasitic disease. l Non-communicable diseases are rare to non-existent. l Early nomads lived in small bands, infrequently contacting others. Numbers were not large enough and bands were not dense enough to maintain (spread) acutely infectious diseases. Spread either by fomites or by zoonoses.

Agriculture l transition from a nomadic to a settled way of life l an increase in food supply l expansion of populations l creation of first ‘urban’ areas with large populations in continuous close contact.

Agriculture l Agriculturalists: l Lacked mechanized power l Were physically active l Domesticated plants and animals l Diet was different from that of hunter-gatherer, but still based mainly on unrefined plant foods. Dairy products consumed for the first time.

Agriculturalist health and disease l Life was short, death rates were high. l Main causes of death include: acute infectious diseases, accidents, food shortage, parasitic diseases, dietary insufficiency. l Non-communicable diseases are rare to non-existent. l Acutely infectious diseases are spread either by fomites or by zoonoses. l Connection between public health and infection control/spread.

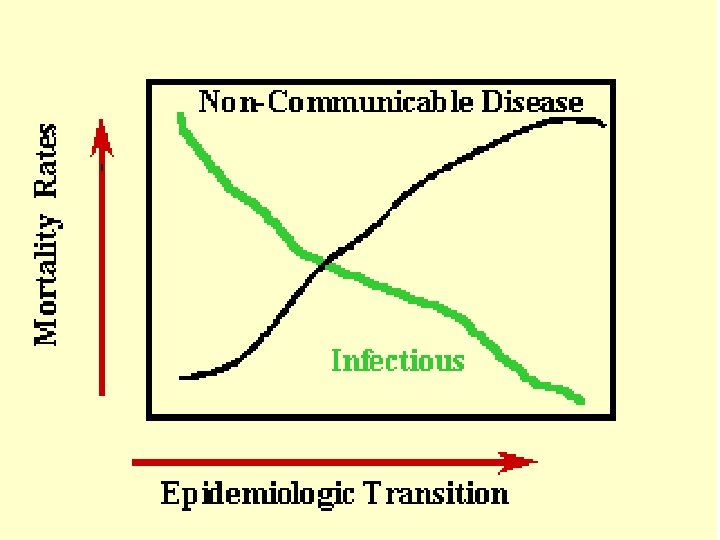
Industry l Change from agriculture to industry takes place over a few hundred years. Effect on health is profound, with the decline of infectious diseases and the rise on non-communicable diseases. l Modern rise in population is distinguished from all previous increases by its size, continuity and duration. l A major contributor is the decline in death rate, increase in normal longevity of modern man

Industry Industrialists: l Sedentary lifestyle l Longer life l Abundant food l Processed food l Degraded environment l Increase in medical technology

Industrialist health and disease: l Life is extended, death rates fall significantly. l Main causes of death include: non-communicable diseases (cancer, CVD, diabetes, hypertension). l Although much in decline, acutely infectious diseases are spread either by fomites or by zoonoses. l Connection between public health and infection control/spread. l Acute infections decline because of improved public health, improved medical treatment, increased resistance to infection.

It is of interest that for the 15 -54 year olds in developing and developed countries, the causes of death are very much the same.
")
Death, by Broad Cause Group 2000 Total deaths: 55, 694, 000 Injuries (9. 1%) Non-communicable conditions (59. 0%) Communicable diseases, maternal and perinatal conditions and nutritional deficiencies (31. 9%) Source: WHO, World Health Report 2001

urban 1960 Rural urban Rural USA Rural urban Rural 2006 urban Developing

Non-communicable Disease The Multicausative Disease Model Environment Behaviors Genetic makeup

Causes of the Chronic Non-Communicable Diseases Genetics: 16% Medicine: 10% Environment: 21% Lifestyle: 53% Smoking, Bad Diets, Lack of Exercise, Obesity

Emerging importance of NCDs: l The second half of the 20 th century showed major health transitions in the world, propelled by socioeconomic and technological changes which profoundly altered life expectancy and ways of living through creating a human capacity to use science to both prolong and enhance life. Among these health transitions, the most globally widespread change has been the rising burden of NCDs including CVD, cancers, D. M. , traffic injuries, neuropsychiatric conditions, and other chronic diseases.
 l Although many developing countries currently face a double")
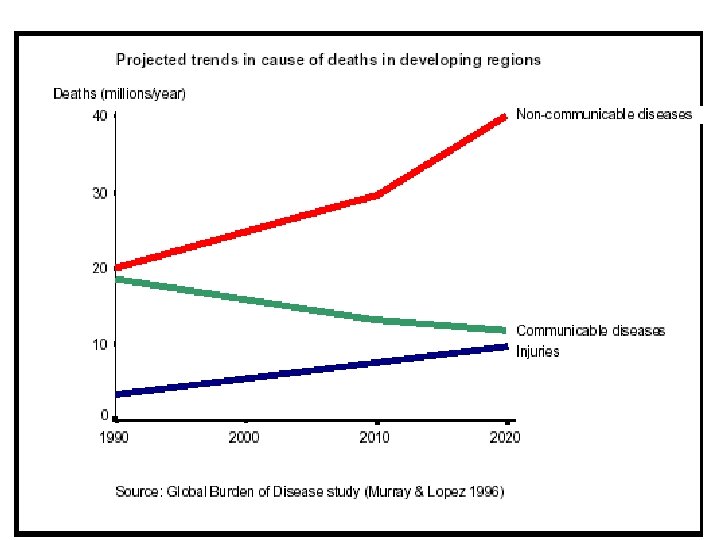
Emerging importance of NCDs(cont. ) l Although many developing countries currently face a double burden of infectious diseases and NCDs, the latter are fast replacing the traditional enemies of infectious diseases and malnutrition as the leading causes of disability and premature death. This trend will continue and by the year 2020, NCDs are expected to account for seven out of every ten deaths in the developing region, compared to less than a half today.

The reasons for this change are: l 1. The decline of infections as a cause of premature death in the affluent industrial nations. The reasons for this decline have been primarily ecological, altered environmental and living conditions, improved nutrition, and smaller family size, reducing the chance of exposure to infection of younger siblings by older ones. These collectively played a more important role than advances in medical science and technology such as the development of antibiotics.
 l 2. Demographic transition or aging of")
The reasons for this change (Contin. ) l 2. Demographic transition or aging of the population. Demographic transition is characterized by a decline in mortality and a drop in fertility. Fewer children are being borne, but more of those borne are surviving to reach old age. Therefore the proportion of persons aged 65 years or above has risen to over 15% in some developed countries and it will continue to rise reaching 20% or more early in the 21 st century. The overall results of these demographic changes are that the prevalence of diseases that occur mainly in the older age group rises.
 l 3. Lifestyle changes: Many countries have")
The reasons for this change (Contin. ) l 3. Lifestyle changes: Many countries have experienced economic growth and development over the past decades. This socioeconomic development has brought about benefits such as improved access to health care, education, safe drinking water and sanitation. Unfortunately, it has also brought about changes in lifestyle, nutrition and traditional social and family structures. Of these lifestyle changes are:
 l A. Smoking or tobacco addiction: It")
The reasons for this change (Contin. ) l A. Smoking or tobacco addiction: It is estimated that about 30% of all cancers are attributable to tobacco addiction. In addition, smoking is implicated as a risk factor for coronary heart diseases (CHD), and chronic obstructive pulmonary diseases.
 l B. Physical inactivity: Another striking characteristic")
The reasons for this change (Contin. ) l B. Physical inactivity: Another striking characteristic of modern affluent industrial nations is the lack of physical activity and the prevalence of obesity particularly among teenagers. A trend attributable to the many hours spent watching television and snacking while doing so.
 l C. High fat intake: The high")
The reasons for this change (Contin. ) l C. High fat intake: The high intake of fat in the diet of modern western countries is associated with the rising incidence of many NCDs such as CHD and cancers. l D. Social & behavioral factors: Some sociocultural factors such as occupation, and education may play a role as risk factors for NCDs. Attitudes towards aggressive and violent behavior seem to vary greatly between cultures and countries. Hostility and anxiety, components of type–A personality are suggested as a risk factor for CHD.
 l E. Impact of cars: The increase")
The reasons for this change (Contin. ) l E. Impact of cars: The increase in the number of private cars as the principal means of transport for work and recreation resulted in rising incidence of traffic related injuries. In addition to their role in air pollution.

Socioeconomic burden of NCDs l Death or disability from NCDs in the productive Middle Ages results in major economic burdens on the affected individuals, their families and society as a whole. The management of established NCDs (diagnosis & treatment) is often technology-intensive and expensive. Individual as well as societal resources are already being drained, at a disproportionately high level by the care management of NCDs, often drawing scarce resources away from the unfinished agenda of infectious diseases and nutritional disorders control.
 l Though NCDs epidemics usually originate in the")
Socioeconomic burden of NCDs (Cont. ) l Though NCDs epidemics usually originate in the upper socioeconomic strata, they diffuse across the social spectrum, with the social gradient ultimately reversing and the poor becoming predominately afflicted. Indeed, in the more mature stages of these epidemics, the poor are the often worst afflicted in terms of disease and usually the most marginalized in terms of care.
 In")
Health services today will not be able to meet the challenges of (NCDs) In developing countries l No or weak national data are available on the overall incidence and prevalence of NCDs in most countries. l In general we depend on mortality data to estimate the impacts of these diseases. l No classification by age or gender. No any information on disabilities resulting from any of the chronic diseases l The current system counts mainly the visits of the patients to PHC centers, which does not reflect the real prevalence and incidence. l Fragmentation in reporting and managing system regarding NCDs. This lack of information leads to: - Inability to estimate the direct and indirect cost; resources required e. g. drugs, policy; and decision making regarding prevention and treatment

Some Continuing Challenges l Lack of national policies for NCD prevention and control l Low resources - only 1/3 of countries have a budget line for NCD prevention & control. l Lack of NCD surveillance systems l Fragmented and uncoordinated care l PHC capacity to deal with NCDs is poor

NCD CHALLENGES Cost Pressures Disease burden, interventions, drugs Quality of Care CHANGES NEEDED l Comprehensiveness ¡ With policy/legislation support l Coordination ¡ Information flows Care teams, medical records & financial incentives l Continuity Prevention l Communication Fragmentation, lack of protocols, lack of financial incentives/support Poverty ¡ Organized Care ¡ Orientation on self management l Community linkages
- Slides: 32