Epidemiology and Prevention of Vaccine Preventable Diseases Meningitis

Epidemiology and Prevention of Vaccine. Preventable Diseases Meningitis Meningococcal Disease and Meningococcal Vaccines By: Dr. Yossra K. Al-Robaiaay Assistant professor FICMS (FM)

Meningitis: is a disease caused by the inflammation of the protective membranes covering the brain and spinal cord known as the meninges. The inflammation is usually caused by an infection of the fluid surrounding the brain and spinal cord.

Meningitis may develop in response to a number of causes, usually bacteria or viruses, but meningitis can also be caused by physical injury, cancer or certain drugs.

The severity of illness and the treatment for meningitis differ depending on the cause. Thus, it is important to know the specific cause of meningitis.

There are 5 "types" of meningitis 1. Bacterial Meningitis Caused by bacteria, like Neisseria meningitidis and Streptococcus pneumoniae. It can be a life-threatening infection that needs immediate medical attention. There are vaccines to prevent some kinds of bacterial meningitis.

2. Viral Meningitis Caused by viruses, like enteroviruses and herpes simplex viruses. It’s serious, but rarely fatal in people with normal immune systems. There are vaccines to prevent some kinds of viral meningitis.

3. Fungal Meningitis Caused by fungi like Cryptococcus and Histoplasma. Usually acquired by inhaling fungal spores from the environment. People with certain medical conditions like diabetes, cancer, or HIV are at higher risk of fungal meningitis.

4. Parasitic Meningitis Caused by parasites. less common in developed countries. Parasites, like Angiostrongylus cantonensis can contaminate food, water and soil

5. Non-infectious Meningitis Not spread from person to person, but can be caused by cancers, systemic lupus erythematosus (lupus), certain drugs, head injury, and brain surgery.

Bacterial Meningitis: Most frequent in children age 2 months to 2 years of age Higher incidence during winter and spring Neisseria meningitidis, Streptococcus pneumoniae and Hemophilus influenza type b cause more than 75% of all cases of bacterial in most studies and 90% of bacterial meningitis in children.

Previously Hemophilus influenza type b is the most common cause of bacterial meningitis. It has been largely eliminated by immunization programs.
 of polysaccharide capsule")
Haemophilus influenzae Aerobic gram-negative bacteria Polysaccharide capsule Six different serotypes (a-f) of polysaccharide capsule 95% of invasive disease caused by type b

Haemophilus influenzae type b Meningitis Accounted for approximately 50%-65% of cases in the pre-vaccine era. Hearing impairment or neurologic sequelae in 15%-30% Case-fatality rate 2%-5% despite of effective antimicrobial therapy.

Epidemiology of Haemophilus influenzae type b Reservoir Human Asymptomatic carriers Transmission Respiratory droplets Temporal pattern Peaks in Sept-Dec and March-May Communicability Generally limited but higher in some circumstances

Haemophilus influenzae type b Risk Factors for Invasive Disease Exposure factors ◦ household crowding ◦ child care attendance ◦ low socioeconomic status ◦ low parental education ◦ school-aged siblings Host factors ◦ race/ethnicity ◦ chronic disease

Neisseria meningitidis Aerobic gram-negative bacteria At least 13 serogroups based on characteristics of the polysaccharide capsule Most invasive disease caused by serogroups A, B, C, Y, and W-135 Relative importance of serogroups depends on geographic location and other factors (e. g. age)

Neisseria meningitidis Severe acute bacterial infection. Cause of meningitis, sepsis, and focal infections. Epidemic disease in sub-Saharan Africa Current polysaccharide vaccine licensed in 1978 Conjugate vaccine licensed in 2005

Meningococcal Disease Pathogenesis Organism colonizes in nasopharynx Nasal carrier in 25% of 18 y-25 y. In some persons organism invades bloodstream and causes infection at distant site Antecedent URI may be a contributing factor

Epidemiology International Serogroups A, B, and C account for most cases worldwide. Serogroups A and C predominate in Asia and Africa, and serogroups B and C predominate in Europe, North America, and South America.

Epidemiology International For more than a century, serogroup A meningococcal disease has been endemic in the African Meningitis Belt, which extends from Ethiopia in eastern Africa to Senegal in West Africa.
 in Saudi Arabia")
Outbreaks of meningococcal disease occurred during the annual hajj (pilgrimage) in Saudi Arabia in 2000 and 2001 among pilgrims and household contacts. Outbreaks have also occurred in Africa, parts of Asia, South America.

Serogroup A is usually implicated in these epidemics. Outbreaks are also occasionally reported in the United States.

Meningococcal disease may be significant but under-reported problem in developing Asian countries. Serogroup W-135 has been associated with pilgrims returning from the hajj.

Up to 95% of patients with meningococcal disease have meningococcemia and/or meningitis. Up to 50% have meningococcemia without meningitis. Fulminant meningococcemia occurs in up to 20%. Nosocomial transmission to patient care personnel and laboratory staff is rare.

Risk 1. Age: Factors: Infants have the highest risk of the disease. Rates decrease after infancy and then increase in adolescence and young adulthood. In some countries : male are at higher risk than female 2. Certain medical conditions ◦ There are certain diseases, medications, and surgical procedures that may weaken the immune system or increase risk of meningitis in other ways :
. , functional")
Like: ◦ Terminal complement pathway deficiency ◦ Asplenia( absence of the spleen). , functional asplenia impaired reticuloendothelial function of the spleen, as seen in children with sickle cell anemia. Concurrent upper respiratory tract infection 3. Genetic risk factors

◦ 4. Active and passive smoking. 5. Poor living conditions. ◦ Infectious diseases tend to spread more quickly where larger groups of people gather together. College students living in dormitories and military personnel are at increased risk for meningococcal meningitis.

6. Working with meningitis-causing pathogens ◦ Microbiologists who are routinely exposed to meningitis-causing pathogens are at increased risk. 7. Travel ◦ Travelers to the meningitis belt in sub-Saharan Africa may be at risk for meningococcal meningitis, particularly during the dry season. Also at risk for meningococcal meningitis are travelers to Mecca during the annual Hajj and Umrah pilgrimage

Meningococcal Disease Epidemiology Reservoir Human Transmission Respiratory droplets Temporal pattern Peaks in late winter–early spring Communicability Generally limited
 Abrupt")
Meningococcal Disease Clinical Features Incubation period 3 -4 days (range 2 -10 days) Abrupt onset of fever, meningeal symptoms, hypotension, and rash Fatality rate 9%-12%; up to 40% in meningococcemia

Meningococcal Meningitis Most common pathologic presentation Result of hematogenous dissemination Clinical findings: ◦ fever ◦ headache ◦ stiff neck ◦ petechial/purpuric rash ◦ hypotension ◦ multiorgan failure
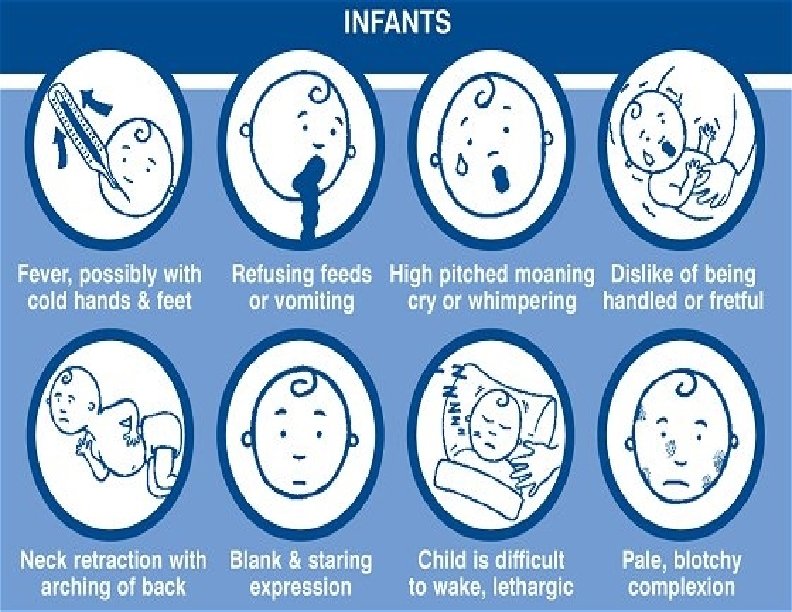
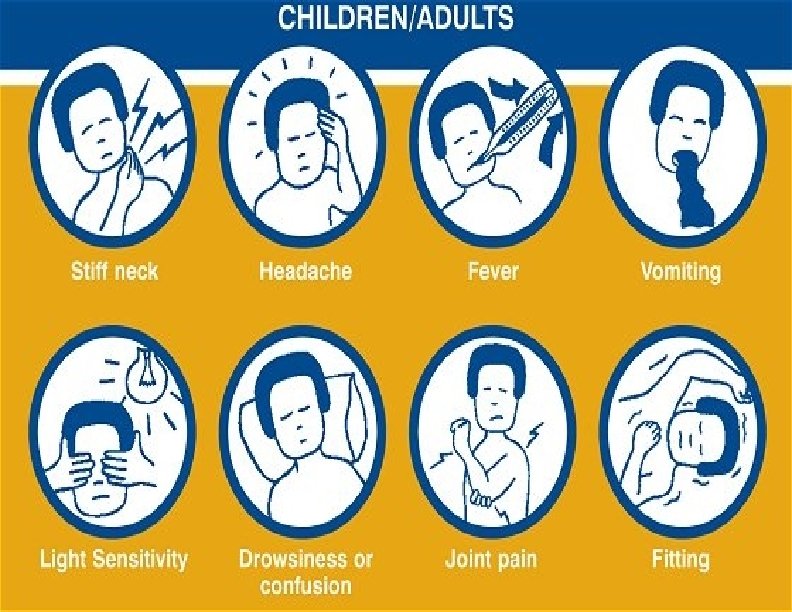

Clinical manifestations Meningococcal meningitis LOGO www. themegallery. com

Clinical manifestations Meningococcal meningitis LOGO www. themegallery. com

Patient placed supine with hips flexed 90 degrees. Examiner attempts to extend the leg at the knee Positive test elicited when there is resistance to knee extension, or pain in the lower back or thigh with knee extension

Patient placed in supine position and neck is passively flexed towards the chest Positive test is elicited when flexion of neck causes flexion at knees and/or hips of the patient

Jolt Accentuation Patient rotates head in horizontal plane two to three times per second, and the test is considered positive if this worsens the headache pain.

Meningococcemia is defined as dissemination of meningococci into the bloodstream and is a medical emergency, making early recognition of the disease.

Meningococcemia Patients with acute meningococcal infection can present clinically with one of 3 syndromes: meningitis, meningitis with meningococcemia, or meningococcemia without obvious meningitis. Prior to the advent of antibiotics, almost all cases resulted in death or marked morbidity.

Meningococcal Disease Laboratory Diagnosis The gold standard for diagnosis is recovery of meningococci from a sterile site( CSF, OR BLOOD) Bacterial culture Gram stain Non-culture methods ◦ Antigen detection in CSF ◦ Serology

Locate L 3 -L 4 disk space using superior iliac crests as landmarks

Medical Management Initial empiric antibiotic treatment after appropriate cultures are obtained Treatment with penicillin alone recommended after confirmation of N.

Methods of control Preventive measures: 1. Educate the public on the need to reduce direct contact and exposure to droplet infection. 2. Quadrivalent meningococcal polysaccharide vaccine containing groups (A, C, Y, W-135) , ( bivalent AC) two polysaccharide vaccine currently available on the market Administered by subcutaneous injection 10 -dose vial contains thimerosal as a preservative

Meningococcal vaccines protect against most types of meningococcal disease, although they do not prevent all cases. There are two kinds of vaccines that protect against Neisseria meningitidis : meningococcal polysaccharide vaccine (Menomune®), and meningococcal conjugate vaccine (Menactra® and Menveo®).

Meningococcal Vaccine Recommendations Recommended for persons at increased risk of meningococcal disease: ◦ Microbiologists who are routinely exposed to isolates of N. meningitidis ◦ Military recruits ◦ Persons who travel to countries in which N. meningitidis is hyperendemic or epidemic ◦ terminal complement component deficiency ◦ functional or anatomic asplenia

Meningococcal Vaccine Recommendations Both MCV and MPSV recommended for control of outbreaks caused by vaccinepreventable serogroups Outbreak definition: ◦ 3 or more confirmed or probable primary cases ◦ Period <3 months ◦ Primary attack rate >10 cases per 100, 000 population.

MPSV Recommendations Approved for persons 2 years of age and older Not recommended for routine vaccination of civilians Should be used only for persons at increased risk of N. meningiditis infection who are 56 years of age or older, or if MCV is not available

Meningococcal Vaccine Revaccination may be indicated for persons at increased risk for infection Revaccination may be considered 5 years after receipt of the MPSV MCV is recommended for revaccination of persons 2 through 55 years of age although use of MPSV is acceptable Revaccination after receipt of MCV is not recommended at this time

Meningococcal Vaccines Adverse Reactions MPSV Local MCV reactions 4%-48% 11%-59% for 1 -2 days Fever 3% 5% Systemic reactions 3%-60% 4%-62% (headache, malaise fatigue)

Meningococcal Vaccines Contraindications and Precautions Severe allergic reaction to vaccine component or following prior dose of vaccine Moderate or severe acute illness

Meningitis- Prevention Chemoprophylaxis for close contacts of index case of Neisseria; treat contacts less than 4 years of age. Vaccinate all children, especially those at risk or those with a splenia

Meningitis- Prevention Control of patient, contacts and the immediate environment: 1. Report to local health authority. 2. Isolation : for 24 hours after start chemotreatment. 3. Concurrent disinfection. 4. Protection of contacts: close surveillance of household day care and other intimate contact for early signs of illness

Specific treatment: penicillin given paranterally in adequate dose is the drug of choice, ampicilline and chloramphinicol are also effective.

Pneumococcal Disease Clinical Syndromes Pneumonia Bacteremia Meningitis

Pneumococcal Disease in Children Bacteremia without known site of infection most common clinical presentation S. pneumoniae leading cause of bacterial meningitis among children younger than 5 years of age Highest rate of meningitis among children younger than 1 year of age Common cause of acute otitis media

Pneumococcal Disease Epidemiology Reservoir Human carriers Transmission Respiratory Temporal pattern Winter and early spring Communicability Unknown Probably as long as organism in respiratory secretions
 Persons")
Pneumococcal Disease Outbreaks not common Generally occur in crowded environments (jails, nursing homes) Persons with invasive disease often have underlying illness May have high fatality rate

Pneumococcal Vaccines 1977 14 -valent polysaccharide vaccine licensed 1983 23 -valent polysaccharide vaccine licensed (PPV 23) 2000 7 -valent polysaccharide conjugate vaccine licensed (PCV 7)

Aseptic meningits

Aseptic meningitis: General Definition Aseptic meningitis – refers to patients who have clinical signs and laboratory evidence for meningeal inflammation with negative routine bacterial cultures

Common Symptoms Fever Headache Altered mental status Stiff neck Photophobia Nausea/vomiting
 Lymphocytic Choriomeningitis virus (LCM) Mumps May")
Viral Meningitis Enteroviruses Herpes HIV Simplex virus (HSV) Lymphocytic Choriomeningitis virus (LCM) Mumps May also accompany primary VZV, outbreaks of herpes zoster, EBV, CMV, and adenoviruses.
")
Bacterial Infections that can present with negative cultures Parameningeal bacterial infections (epidural, subdural abcess) Partially treated bacterial meningitis or patients who develop meningitis while already on antibiotics Leptospira species. M. Tuberculosis (look for signs of disease elsewhere in the body as a clinical clue) Bacterial endocarditis

Malignancy as a cause of meningitis It is also important to keep in mind that lymphoma, leukemia, and metastatic carcinomas and adenocarcinomas can occasionally present with an aseptic meningitis syndrome.

Thank you
- Slides: 66