Epidemiologia Analtica No inferioridade ou equivalncia Site www






")







- Slides: 24
Epidemiologia Analítica Não inferioridade ou equivalência Site: www. epi. uff. br
Ensaios clínicos randomizados • Ensaios clíncos; – Superioridade: São desenhados para mostrar a superioridade de uma “nova” intervenção sobre um placebo ou uma intervenção “de referência” (maioria). – Não inferioridade busca estabelecer se uma “nova” intervenção não é pior que a intervenção “de referência”. – Equivalência busca estabelecer se uma “nova” intervenção equivale à intervenção “de referência”.
ECR • Superioridade – Efeito da “nova” intervenção é maior que o efeito da intervenção “de referência” e a diferença é estatisticamente significativa => há superioridade – Efeito da “nova” intervenção é maior que o efeito da intervenção “de referência” mas a diferença não é estatisticamente significativa => não se pode concluir que há superioridade mas NÃO SE PODE AFIRMAR QUE SÃO EQUIVALENTES!
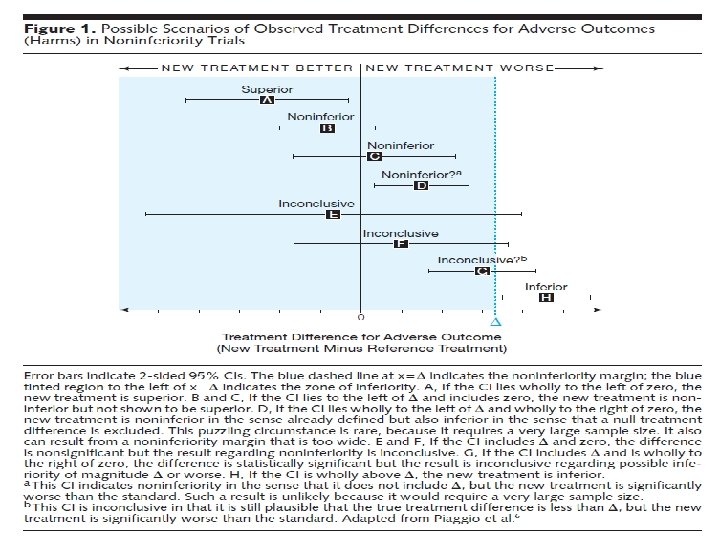
ECR de não inferioridade • Premissa: “nova” intervenção tem vantagem sobre a intervenção “de referência” – ou é melhor tolerada, ou implica em um número menor de doses, ou tem menor custo, ou a via de administração é menos invasiva. • Cada vez mais utilizada pela indústria farmacêutica • Estabelece-se antes do início do ensaio, que diferença máxima (margem) se aceitará para se admitir a não inferioridade (igualdade é impossível de se encontrar) quanto ao desfecho principal.
Effects of nebivolol or irbesartan in combination with hydrochlorothiazide on vascular functions in newly-diagnosed hypertensive patients: the NINFE (Nebivololo, Irbesartan Nella Funzione Endoteliale) study. Vitale e colegas. Int J Cardiol. 2012 Mar 8; 155(2): 279 -84. BACKGROUND: Arterial hypertension affects endothelial function and arterial stiffness. The angiotensin (AT 1) receptor antagonist irbesartan improves endothelial function and arterial stiffness in hypertensive patients. Nebivolol, a beta(1)-selective beta blocker, reduces systemic vascular resistance and stimulates nitric oxide release thus exerting positive effects on vascular function. However, comparative studies on the vascular effects of third generation beta-blockers and AT 1 receptor blockers are lacking. Aim of this randomized, double-blind study was to test the hypothesis of non-inferiority of nebivolol to irbesartan, both in association with hydrochlorothiazide, on endothelial function, arterial stiffness and central hemodynamic parameters in patients with arterial hypertension naïve on therapy.
METHODS: Sixty-five patients were randomized to receive irbesartan/hydrochlorothiazide. . . or nebivolol/hydrochlorothiazide. . . for 8 -weeks. Endothelial function, pulse wave velocity, augmentation index, central and brachial blood pressures were measured at baseline and at the end of the study. The sample size for the study was calculated on the hypothesis of non inferiority between the two treatment groups on endothelial function assessed by post-ischemic reactive hyperemia. Assuming an effect of Irbesartan of 6. 7% after 8 weeks of treatment and a SD for both treatment groups of 0. 9% estimates the relative margin for non inferiority was set at 9% of the mean percentage variation measured in the Irbesartan group (0. 6% in absolute terms). Assuming equality of Nebivolol and Irbesartan and setting the type-I error rate at 5%, it was estimated that 29 subjects per treatment group were needed to demonstrate non inferiority of Nebivolol with a power of 80%, using one-sided t-test for independent samples. Six percent of the study subjects were expected to experience major protocol violations, and considering a drop-out rate of 8%, the sample size was raised to 34 individuals per treatment group (68 overall).
(alguns resultados)
Ensaios clínicos randomizados de equivalência • Premissas: A mesma dos ensaios de não inferioridade • Estabelece-se antes do início do ensaio, que o efeito da “nova” intervenção estará entre (- ) e (+ ) em relação à intervenção “de referência”, definido clinicamente. • As duas intervenções podem ser consideradas equivalentes se o IC 95% da diferença dos efeitos estiver completamente contido entre ( - ) e (+ ).
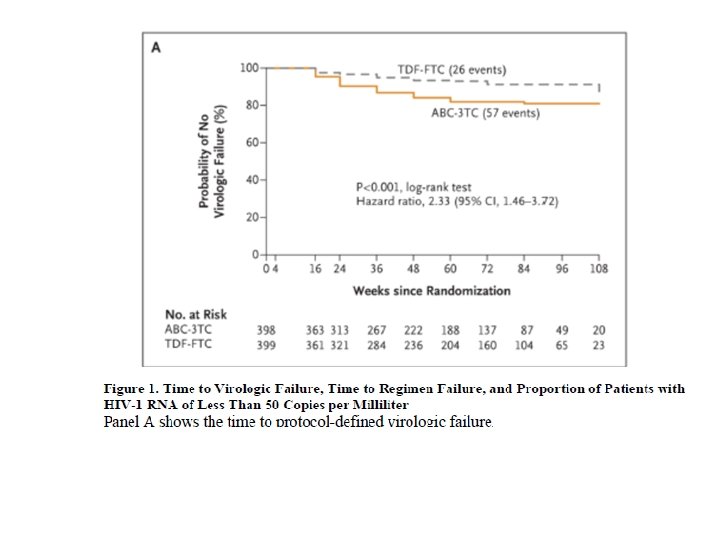
Sax e colegas. Abacavir–Lamivudine versus Tenofovir– Emtricitabine for Initial HIV-1 Therapy. N Engl J Med. 2009 December 3; 361(23): 2230– 2240. BACKGROUND. The use of fixed-dose combination nucleoside reverse-transcriptase inhibitors (NRTIs) with a nonnucleoside reverse-transcriptase inhibitor or a ritonavir-boosted protease inhibitor is recommended as initial therapy in patients with human immunodeficiency virus type 1 (HIV-1) infection, but which NRTI combination has greater efficacy and safety is not known.
METHODS. In a randomized, blinded equivalence study involving 1858 eligible patients, we compared four once-daily anti retroviral regimens as initial therapy for HIV-1 infection: abacavir– lamivudine or tenofovir disoproxil fumarate (DF)–emtricitabine plus efavirenz or ritonavir-boosted atazanavir. The primary efficacy end point was the time from randomization to virologic failure (defined as a confirmed HIV-1 RNA level ≥ 1000 copies per milliliter at or after 16 weeks and before 24 weeks, or ≥ 200 copies per milliliter at or after 24 weeks). Regimens were considered equivalent if the two-sided 95% confidence interval for the hazard ratio was between 0. 71 and 1. 40. A planned sample size of 1800 subjects (450 per group) would provide an 89. 8% probability of declaring equivalence if two regimens were the same, assuming uniform accrual, exponential virologic failure, and lost-to-followup time istributions among the four groups, with event probabilities of 17. 46% and 10. 00%, respectively, at 48 weeks.
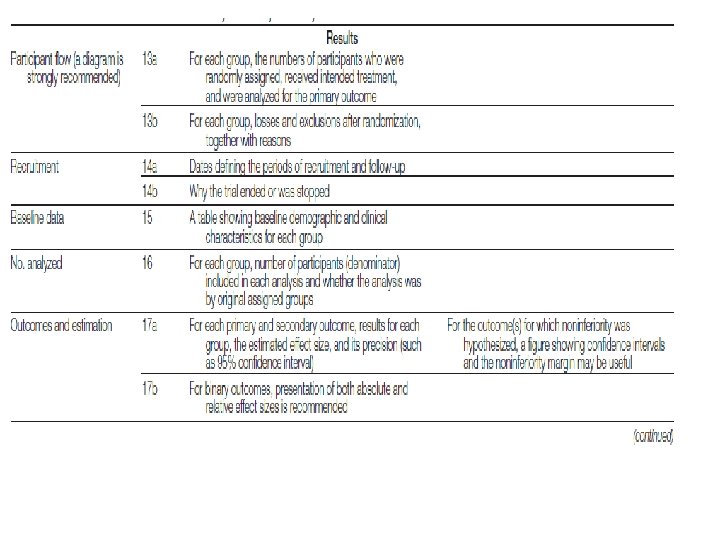
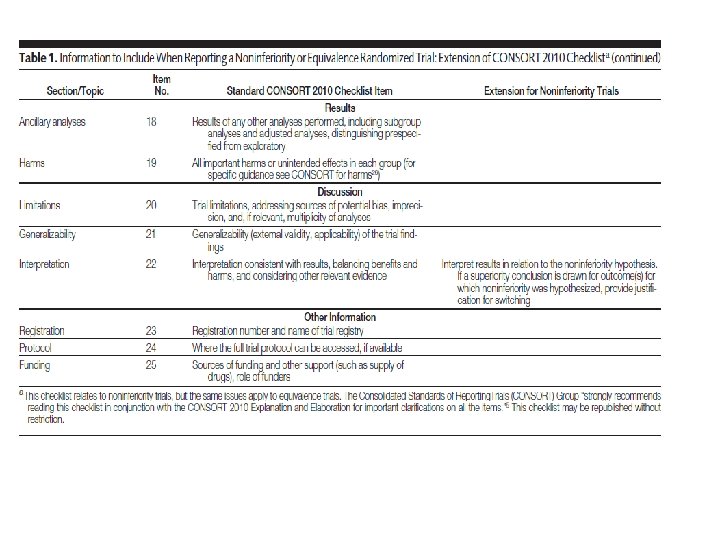
O que um bom artigo de ECR de não inferioridade ou equivalência deve conter CHECL LIST DO CONSORT Consolidated Standards of Reporting Trials
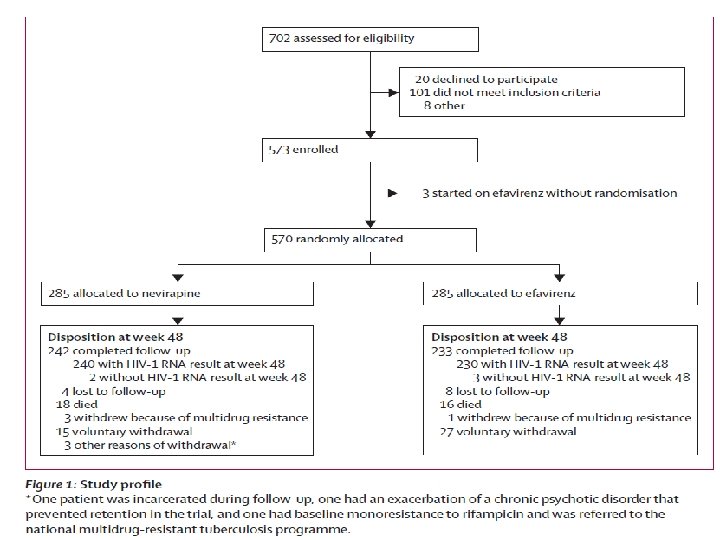
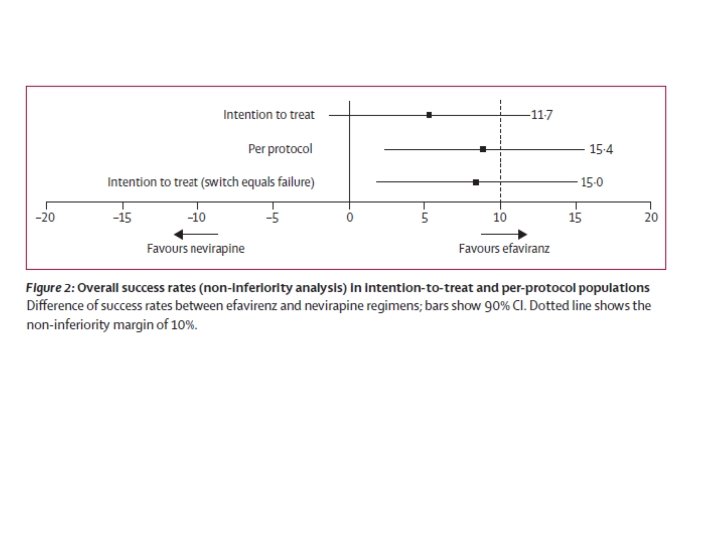
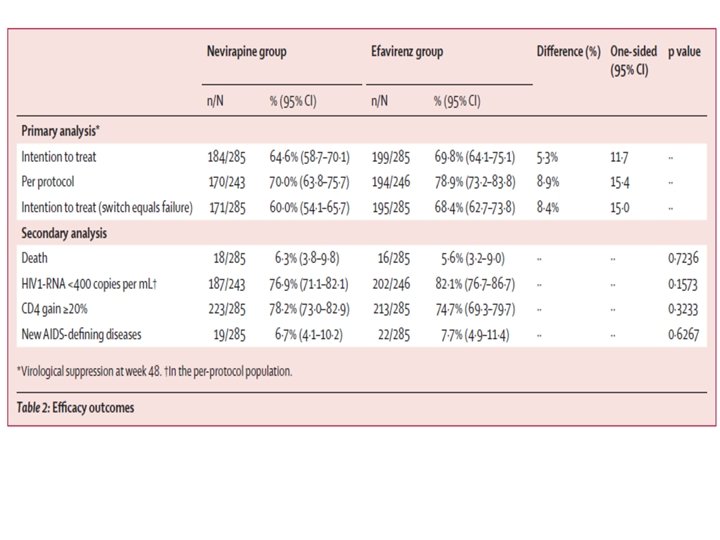
Análise do artigo: Nevirapine versus efavirenz for patients co-infected with HIV and tuberculosis: a randomised non-inferiority trial
Análise do artigo: Nevirapine versus efavirenz for patients co-infected with HIV and tuberculosis: a randomised non-inferiority trial