EPDM 566 Epid of CVD The Epidemiology of

 • A disease in itself Ø Has its own ICD code •")


 2. Regular audible")




 -")



individual variability -")












")
")













")






 Design: • 975 men and")













: Diet 2")
 DIET and WEIGHT LOSS Randomized groups: 1. Diet (Wt")

: 12 -1500 mg/day • Median intake Males >")









 In general, low SES is associated with higher BP. Low SES")
- Slides: 78
EPDM 566 – Epid of CVD The Epidemiology of Hypertension Raymond Knutsen MD, MPH
Hypertension (HT) • A disease in itself Ø Has its own ICD code • A risk factor for other diseases Stroke – HT the most important risk factor Ø CHD – HT one of the 3 most important risk factors Ø Renal Disorders Ø Eye Diseases Ø
Blood Pressure Measurements Perceived as: • • SIMPLE ACCURATE RELIABLE EASY TO COMPARE
Blood Pressure Measurements Actually, one of the most difficult biologic measures to standardize
Korotkoffs’ sounds 1. The first audible beat – snapping sound (SBP) 2. Regular audible beats • The murmurs heard between SBP and DBP 3. Not used in BP measurements 4. When sound becomes more muffled 5. When sound disappear (cuff pressure ≤ DBP)
Possible Biases in Blood Pressure Recording • What Korotkoffs’ sound was recorded? - Traditional BP devices - sphygmomanometer - Automatic BP devices - uses oscillometric techniques Measure somewhat lower DBP Not depending on the hearing • Rounding off? – nearest 2, 5 or 10
Possible Biases in Blood Pressure Recording • Random or non-differential misclassification - Usually biases the result toward the null – no difference between treatment and control - Degree of misclassification does not differ between groups being compared • Non-random or differential misclassification: - Only males rounded up? - Only hypertensives rounded down?
Possible Biases in Blood Pressure Recording • What is diastolic pressure? The last audible beat? The pressure at which you would expect to hear the next beat? • Sitting or supine? • How long has the patient been at rest / not smoking before you measure? • What time did the patient have his/her last meal?
Possible Biases in Blood Pressure Recording • Is the bladder empty? • Is the brachial artery kept at heart level during measuring? • What is the room temperature? • Is the blood pressure device adequately adjusted? • Has the person measuring been standardized?
Blood Pressure in Scientific Literature Used either as: • A Risk Factor (Exposure) - Continuous variable - Actual measurement - Dichotomous variable - HT: Yes or No • • Predefined criteria Criteria set during analysis • A Disease (Outcome)
Assessment of Blood Pressure measurements in Scientific Literature • Systolic or Diastolic? • First measurement or the mean of several measures or the 3 rd measurement? • Cut-off points? (Hi, low, normal? ) • How was the measurement done? • Who did the blood pressure recording? • Were the persons doing the blood pressure measurements standardized? • Method – OMRON, Dinamap, Random zero?
Standardization of Blood Pressure measurements • Environment • Measurement Standardized technicians Random zero sphygmomanometer Automatic device
Regression to the Mean in Blood Pressure measurements A continuous variable measured at any given point in time has the tendencies of: • High values to decrease • Low values to increase When repeated measurements are done
Regression to the Mean in Blood Pressure measurements Results from: • Intra-(within-)individual variability - Muscle contraction; Anxiety; Tp Distractions (full bladder) Exercise; Meals “White coat BP” • Random measurement errors
Distribution of Diastolic BP at 3 sequential visits of the Hypertension Detection and Follow-up Program Individuals with DBP≥ 95 mm. Hg Regression to the mean from home screen Individuals with DBP≥ 90 mm. Hg Regression to the mean from clinic screen and/or “white coat BP” J Chron Dis 1978; 31: 651
Definition of Hypertension* Classification of Blood Pressure for Adults Aged 18 years or older BP classification Normal Prehypertension Stage 1 Stage 2 Systolic BP, mm Hg < 120 -139 140 -159 ≥ 160 Diastolic BP, mm Hg and or or or <80 80 -89 90 -99 ≥ 100 Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of high Blood Pressure. * JAMA, 2003; 289: 2560 -72.
Management of Hypertension* Recommended Threshold for Hypertension Diagnosis <60 yrs ≥ 60 yrs 140/90 150/90 Recommended Blood Pressure Treatment Goals With DM With chronic renal failure > 80 yrs 140/90 ≥ 60 yrs 150/90 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. Report from the Panel Members * 2014 Appointed to the Eighth Joint National Committee (JNC 8). JAMA, 2014; 311(5): 507 -520.
Hypertension – size of problem Varies by place and race Ex. The WHO MONICA project Multinational Monitoring of trends and determinants in CVD 38 population samples in 21 countries Random sampling to assess risk factors Sample sizes: 1000 - 3000 Baseline ages: 35 -64 yrs (25 -34 optional) Surveyed in mid-1980 & followed-up for 10 yrs
Hypertension – size of problem Varies by place and race The WHO MONICA project 10 -year major CVD risk factors - se cholesterol - BP - cigarette smoking vs. 10 -year trend in incidence rate of fatal & non-fatal - CHD - stroke
Age-Standardized Proportions of Categories of Blood Pressure Index WHO MONICA Project. Men (35 -64 Years) % THP* % CHP** Population Catalonia 8. 4 25. 0 Glostrup 15. 0 24. 7 Auckland 20. 2 21. 8 N. Sweden 20. 4 25. 5 Beijing 24. 6 6. 9 Newcastle 25. 7 30. 7 Bremen 26. 0 11. 5 Glasgow 32. 0 14. 0 Malta 33. 1 12. 1 Moscow 36. 6 6. 0 Warsaw 37. 4 4. 5 Kuopio 45. 3 6. 4 0 25 50 Proportion (%) I. SBP<160 & DBP<95, HPTreat + II. SBP>159 &/or DBP >94, HPTreat + III. SBP>159 &/or DBP>94, HPTreat IV. SBP<160 & DBP<95, HPTrea. T World Health Statistics Quarterly, 1988; 41: 128 75 100 * Total Prevalence of Hypertension (%) ** Proportion of Controlled Hypertension (%)
Age-Standardized Proportions of Categories of Blood Pressure Index WHO MONICA Project. Women (35 -64 Years) % THP* % CHP** Population Glostrup 12. 6 50. 0 Catalonia 13. 0 72. 3 Auckland 18. 2 52. 2 N. Sweden 18. 8 32. 4 Beijing 21. 5 24. 2 Bremen 23. 3 14. 2 Newcastle 25. 0 46. 4 Glasgow 25. 4 15. 4 Warsaw 30. 9 10. 4 Malta 36. 2 19. 1 Moscow 37. 7 16. 4 Kuopio 37. 6 17. 3 0. 0 25. 0 50. 0 I. SBP<160 & DBP<95, HPTreat + II. SBP>159 &/or DBP >94, HPTreat + III. SBP>159 &/or DBP>94, HPTreat IV. SBP<160 & DBP<95, HPTrea. T World Health Statistics Quarterly, 1988; 41: 128 75. 0 Proportion (%) 100. 0 * Total Prevalence of Hypertension (%) ** Proportion of Controlled Hypertension (%)
Tracking The strong tendency of each individual, children and adults, to retain their relative position in the distribution of a risk factor throughout life. Tracking has been shown for: • CHD risk factors Lipids, obesity • Lifestyle Diet, smoking, exercise
BP Tracking Time
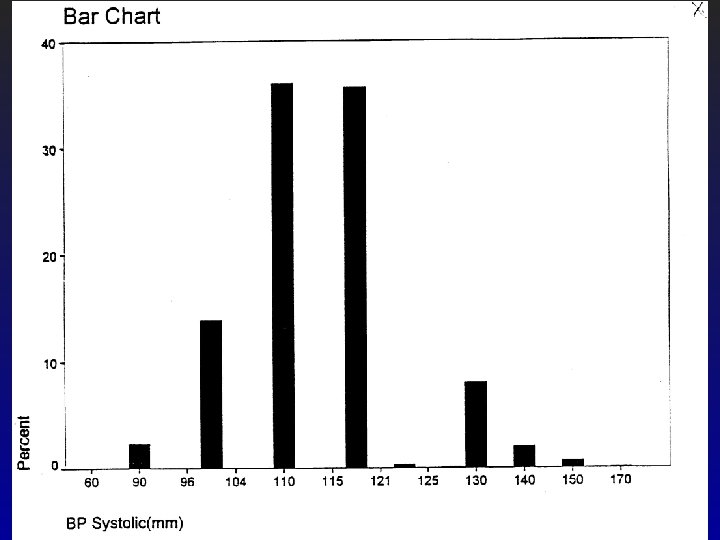
INTERSALT Study Mean SBP % hypertensives in different populations with different mean Systolic Blood Pressure (SBP): 95 -109. 9 5. 2 110 -114. 9 12. 2 115 -119. 9 15. 8 120 -124. 9 23. 1 ≥ 125 26. 8
Epidemiology of Hypertension • Complex and still not fully understood • A number of factors have been linked to hypertension
Factors linked to Hypertension • • Age Race Seasons Geography Obesity Diet Exercise Sosioeconomic Status (SES)
Framingham Study MALES (Bulpitt, 1989)
Framingham Study FEMALES (Bulpitt, 1989)
Is blood pressure increase with age normal?
Populations in which the blood pressure increases little or not at all with age (average of both sexes, in different age groups) Systolic pressure by age group (mm Hg) Population 20 -29 40 -49 60 -69 Brazil (Carajas) 107 100 109 No salt; use lyes of vegetable ash (K salts) New Guinea (Murapins) 126 123 0. 6 gm (24 -hr urine) Botswana 119 (Kung bushmen) 116 122 2. 0 gm (24 -hr urine) Cook Islands (Pukapukas) 116 125 2. 9 -4. 1 gm (24 -hr urine) Jossens JV, 1973 113 Dietary salt
Populations in which the blood pressure increases markedly with age (average of both sexes, in different age groups) Systolic pressure by age group (mm Hg) Population 20 -29 40 -49 60 -69 United States 119 130 140 ± 10 gm/24 hr Portugal 126 134 155 Not measured Sweden 125 138 159 Not measured Belgium 132 143 163 4 -20 gm (24 -hr urine) Cook Island (Rarontongas) 124 151 165 7. 8 -8. 2 gm (24 -hr urine) Norway 130 141 167 Not measured) Wales 120 138 169 8. 0 gm (24 -hr urine) Bahama Islands (blacks) 129 154 176 15 -30 gm (24 -hr urine) Jossens JV, 1973 Dietary salt
Prevalence of Hypertension in the Civilian Noninstitutionalized Adult Poulation of the United States during 1988 -1991 Age % Hypertension* 18 -29 4 30 -39 11 40 -49 21 50 -59 44 60 -69 54 70 -79 64 ≥ 80 65 * Average of three blood pressure measurements ≥ 140/90 mm. Hg on one occation or taking antihypertensive medications Working Group on Primary Prevention of Hypertension, 1993
INTERSALT Study on the relationship between salt intake and blood pressure Started mid-80 ies (Hawaii: 1984 -85) 52 centers worldwide (32 countries) 10, 079 persons, aged 20 -59 years
INTERSALT study
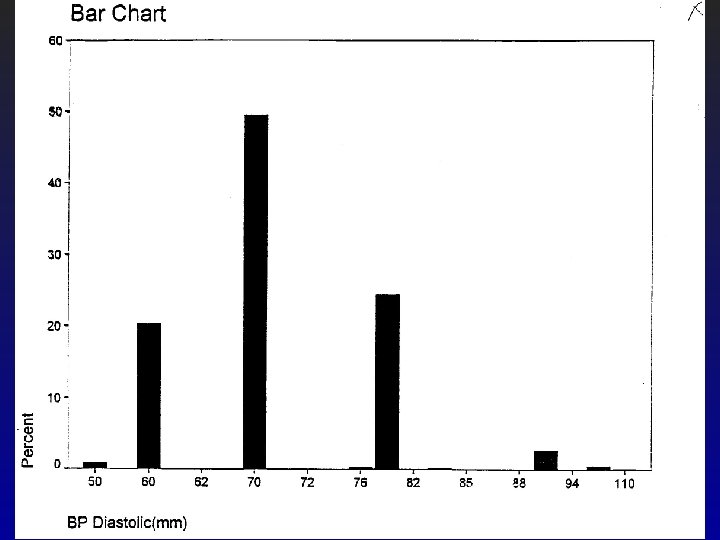
INTERSALT study The spread of both systolic and diastolic blood pressure was small in all 4 populations.
RACE • In the US, blacks have higher BP than nonblacks • This is true for both males and females • The higher prevalence of hypertension among blacks is evident in higher risk of stroke among blacks.
SEASONS Ø BP is higher in the winter than in the summer • Shown in several studies • Similar findings have been made for cholesterol levels Ø Studies at the University of Tromsø, Norway • Seasonal variation was higher in the Spitsbergen Islands than on the mainland
BP: SEASONAL VARIATION Could be due to Ø Ø More sedentary lifestyle in winter Different eating patterns in winter vs. summer Melatonin Vit. D deficiency during winter • Vit. D suppl • Sunlight BP (Intervention studies) Vit. D CHD mortality
Geographic location • England Wales - several studies have shown that BP is higher to the north, in Scotland. • Migration studies indicate that BP in migrants approaches that of the adopting region, supporting environmental causes.
Migration Study
OBESITY Research consistently shows that: • Overweight is associated with higher BP • Losing weight lowers BP
Framingham Study OBESITY (Ann Intern Med 1967; 67: 48)
Obesity & BP - Possible mechanisms Hyperinsulinemia? – Obesity is often accompanied by hyperinsulinemia. – Hyperinsulinemia in turn causes: • increased renal tubular re-absorption of sodium → hypertension. • increased catecholamine turnover in the sympathetic nervous system → vasoconstriction →hypertension
DIETARY factors assoc. with HT • • • Sodium Potassium Na/K ratio Fat – type and amount Fruits and vegetables, fiber, vegetable protein (vegetarian diet) • Other minerals (e. g. Calcium, Magnesium, Phosphorus) • Vitamins (C and D)
INTERSALT Study Main findings: • Positive association between dietary sodium excretion and systolic BP • Inverse relationship between potassium and BP • Na/K ratio directly related to blood pressure • BMI and alcohol intake independently related to BP • Variation in salt intake was much smaller than expected (the high consumption areas of Japan were no longer consuming as much as earlier)
Debate on “salt-sensitivity” • Some studies seem to show that not all persons are “sensitive” to salt intake. E. g. some persons tolerate high intakes of salt without having an elevation in BP. • However, on a population level, a lower salt intake seems to be associated with a lower mean BP, as shown for instance in the INTERSALT study.
INTERSALT study Association between Sodium excretion and SBP Systolic BP
INTERSALT study Association between Sodium excretion and DBP Diastolic BP
TONE study (Trial of Nonpharmacologic Interventions in the Elderly) Design: • 975 men and women • 60 -80 yrs • on one antihypertensive medication • SBP < 145 and • DBP < 85 • Follow-up: 29 months JAMA, 1998; 279: 839 -46. 585 obese persons randomized to: • Control (usual care) • Weight Loss • Sodium reduction • Both weight loss and Na reduction 390 non-obese randomized to: • Control (usual care) • Sodium reduction
TONE study Compliance with sodium restriction was good. JAMA, 1998; 279: 839 -46.
TONE study JAMA, 1998; 279: 839 -46.
TONE study ENDPOINT defined as: • Diagnosed hypertension or • Treatment with anti-hypertensive drugs or • Cardiovascular event JAMA, 1998; 279: 839 -46.
TONE study ENDPOINT defined as: • Diagnosed hypertension or • Treatment with anti-hypertensive drugs or • Cardiovascular event JAMA, 1998; 279: 839 -46.
TONE study All 4 groups JAMA, 1998; 279: 839 -46.
POTASSIUM • Primitive tribal communities have higher potassium consumption than Western societies. • Primitive tribal communities also have lower BP • Potassium (and sodium) content is very different in processed and unprocessed foods.
Sodium and Potassium contents of some natural and equivalent processed foods Natural Food Na K Processed food Na K Mg/100 g Flour, wheat 2. 2 94. 9 White bread 496. 3 122 Rice, raw brown 9. 4 214. 1 Rice, instant fluffed 272. 7 Trace Uncooked peas 2. 1 315. 9 Canned peas (drained) 236. 3 96. 2 Ham, fresh lean 72. 6 332. 5 Ham, light cured 995. 4 311. 2 Beef, lean flank 53. 3 244. 1 Corned beef 942. 1 59. 9 USAD Nutrient Database for Standard Reference
POTASSIUM Chinese randomized, placebo-controlled trial 150 Chinese men and women, aged 35 -64, with initial SBP 130 -159 and/or DBP 80 -94 • Randomly assigned to a 12 week regimen of: – 60 mmol potassium chloride or – Placebo (J of Hypertension 2001; 19: 1325 -31)
POTASSIUM Chinese randomized, placebo-controlled trial RESULTS: Potassium supplemented vs. Placebo • Higher urinary K excretion by 20. 6 mmol/24 hrs (p <. 0001) • Reduction in SBP by 5 mm Hg (95% CI: -2. 13 to 7. 88) • No significant reduction in DBP (J of Hypertension 2001; 19: 1325 -31)
Na/K ratio • Seems important. • Studies indicate a positive association with BP • Ideally, this ratio should be < 1. 0 (J of Hypertension 2001; 19: 1325 -31)
Dietary fat Saturated fat seems to increase risk of BP. • Interesting study conducted some year back in Finland Italy: – Finnish persons randomized to Mediterranean diet (high P/S ratio) and Italian people to a Finnish diet (low P/S ratio). – As a result, the Finnish people reduced their total fat by 25% and increased their P/S ratio to 1. 0. – RESULTS: Significant BP reduction on the Mediterranean diet. (Lancet 1983; 1: 1 -5) (Puska et. al. )
Vegetarian diet Several studies report lower BP among vegetarians and also among person having high intake of fruits and vegetables. • Controlled trials: – Rouse et al– found lower BP while on vegetarian diet. (Lancet 1983; 1: 5 -10) – DASH study – Stamler et. al. (N Eng J Med 1997; 336(16): 1117 -24)
DASH study 459 subjects with SBP<160 and DBP=80 -95 Design: • Run-in period (3 weeks) with the control diet: – Low in fruits, vegetables and dairy products – Fat content typical of average US diet • Randomization to 8 weeks treatment: 1. 2. 3. Control diet (lo fruit + lo vegetables + usual dairy) Diet rich in fruits and vegetables (+ usual dairy) “Combination diet” – diet 2 + low fat dairy products and low saturated fat N Eng J Med 1997; 336(16): 1117 -24
DASH study - results Compared to the control diet (normotensives + hypertensives): Diet 2 Diet 3 SBP -2. 8 (p=. 001) -5. 5 (p=. 001) DBP -1. 1 (p=. 07) -3. 0 (p=. 001) Results according to hypertensive status: Hypertensives Diet 2 Non-hypertensives Diet 3 SBP -11. 4 (p=. 001) -3. 5 (p=. 001) DBP - 5. 5 (p=. 001) -2. 1 (p=. 003) N Eng J Med 1997; 336(16): 1117 -24
HCP study (Hypertension Control Program) DIET and WEIGHT LOSS Randomized groups: 1. Diet (Wt loss, ↓ sodium, ↓ alcohol) 2. No drugs, no diet intervention 3. Continue drugs, no diet intervention JAMA, 1987; 257: 1484 -91
Calcium Several studies report lower BP among persons with high Calcium intake (including those using high levels of low-fat dairy products)
Calcium • Recommended daily allowance (RDA): 12 -1500 mg/day • Median intake Males > 40 years – White: 750 mg – Blacks: < 600 mg • Prevalence of hypertension in Blacks is about 3 x that of whites
Calcium • NHANES study found that hypertensives had lower Ca++ intake than normotensives (N Eng J Med 1982; 307: 226) • Randomized controlled study – Belizan showed that 1 g calcium supplementation per day for 22 weeks reduced DBP by 9% in men and 5. 6% in females. (JAMA 1983; 249: 1161)
Ca++ and Systolic BP Only effect of Ca++ supplementation in hypertensives (Ann Intern Med 1996; 124: 825 -31) DIETARY CALCIUM
Ca++ and Diastolic BP No effect of Ca++ supplementation In any group. (Ann Intern Med 1996; 124: 825 -31) DIETARY CALCIUM
Magnesium Seems to be inversely associated with BP • Cohort Studies which support this: – – – Nurses Health Study (58 218 nurses) Honolulu Heart Study Health Professional Follow-up Study (30 681 men) – (Circulation 1002; 86: 1475 -84) • Randomized controlled trials yield inconsistent results
Average Systolic Blood Pressure Differences Between Categories of intake Using the Lowest Category as Reference. Nurses Health Study, 1984 -1988. Average Syst. BP Difference (mm. Hg) Adjusted for age, BMI and alcohol intake. Nutrients are added one at a time. 0. 6 0. 4 0. 2 0 -0. 2 -0. 4 -0. 6 -0. 8 -1 -1. 2 -1. 4 CA, g/d Mg, g/d K, g/d Fiber, g/d Ca Mg K * Fiber * * * Intake 1 Intake 2 Intake 3 Intake 4 Intake 5 <0. 400 <0. 200 <2. 00 <10. 0 0. 400 -0. 599 0. 600 -0. 799 0. 800 -0. 999 ≥ 1. 000 0. 200 -0. 249 0. 250 -0. 299 0. 300 -0. 349 ≥ 350 2. 00 -2. 39 2. 40 -2. 79 2. 80 -3. 19 ≥ 3. 20 10. 0 -14. 9 15. 0 -19. 9 20. 0 -24. 9 ≥ 25. 0 * P<0. 05
Average Diastolic Blood Pressure Differences Between Categories of intake Using the Lowest Category as Reference. Nurses Health Study, 1984 -1988. Average DIast. BP Difference (mm. Hg) Adjusted for age, BMI and alcohol intake. Nutrients are added one at a time. 0 -0. 2 * -0. 4 * -0. 6 * * * Ca *** Mg * K -0. 8 Fiber * -1 -1. 2 CA, g/d Mg, g/d K, g/d Fiber, g/d * * Intake 1 Intake 2 Intake 3 Intake 4 Intake 5 <0. 400 <0. 200 <2. 00 <10. 0 0. 400 -0. 599 0. 600 -0. 799 0. 800 -0. 999 ≥ 1. 000 0. 200 -0. 249 0. 250 -0. 299 0. 300 -0. 349 ≥ 350 2. 00 -2. 39 2. 40 -2. 79 2. 80 -3. 19 ≥ 3. 20 10. 0 -14. 9 15. 0 -19. 9 20. 0 -24. 9 ≥ 25. 0 * P<0. 05
ALCOHOL Hypertension according to alcohol use in white men and women, age-adjusted Men Number of drinks/day n Women ≥ 160/95 mm. Hg % n None 5, 393 4. 6 10, 353 6. 3 ≤ 2 21, 366 4. 8 31, 165 5. 3* 3 -5 4, 270 8. 2** 2, 074 8. 6** ≥ 6 1, 430 11. 2** 346 11. 3* *P<0. 01 (vs. nondrinkers) **P<0. 001 (vs. nondrinkers) Klatsky AL, et al. Alcohol use, myocardial infarction, sudden cardiac death, and hypertension. Alcoholism: Clin Exp Res 1979; 3: 33
EXERCISE Accumulating evidence supports an inverse association between exercise and BP: • Physical activity BP by an average of 6 -7 mm Hg • Physical activity BP independent of weight loss • Moderate exercise seems to be more effective than vigorous exercise • Daily moderate exercise gives more effect than 3 x/week
EXERCISE and BP Possible mechanisms: • Decreased vascular resistance due to vasodilatation • Increased cardiac output • Decreased sympathetic activity
Socioeconomic Status (SES) In general, low SES is associated with higher BP. Low SES is most probably a marker for a lifestyle associated with higher BP such as: • • • Higher BMI Less education “Poor” diet Higher smoking prevalence Less exercise