EPDM 566 Epid of CVD Pathobiology of Atherosclerosis

EPDM 566 – Epid of CVD Pathobiology of Atherosclerosis Raymond Knutsen MD, MPH

Anatomy of the arteries Tunica intima - endothelium - myoepithelial cells collagen elastic fibers Tunica adventitia Serous layer - connective tissue Tunica media - • nerve fibers • vasa vasorum smooth muscle layer elastic fibers fibrous connective tissue elastin fibers (external elastic membrane)

Schematic arterial wall in cross-section

Arterial Cell Anatomy • The intima - the inner layer lined by a smooth tissue called endothelium • The media - a layer of muscle that lets arteries handle the high pressures from the heart • The adventitia - connective tissue anchoring arteries to nearby tissues

Arterial Cell Anatomy Endothelium or endothelial layer: Lines inside of arterial walls In direct contact with blood Controls passage of substances from blood into arterial wall • Anti-thrombotic = inhibits blood clots • • •

Arterial Cell Anatomy Endothelial Cells: • under normal conditions - protect against the development of atherosclerosis • when damaged - play a major role in its development • Produce several vasoactive substances – Prostacyclin - vasodilator; antithrombotic – Endothelial derived relaxing factor (EDRF) EDRF or nitric oxide inactivates platelets; inhibits smooth muscle cell migration and proliferation

Functions of endothelium • Active site of protein synthesis • Synthesize, secrete, modify and regulate: – – – – Connective tissue components Vasodilators Vasoconstrictors Anticoagulants Procoagulants Fibrinolytic compounds Prostanoids

Endothelium – multifunctional organ that meticulously regulates blood flow Blood flow Luminal Subliminal Cohesive – Luminal – non-thrombogenic, negative charge – Subliminal – adheres to connective tissue and smooth muscle cells – Cohesive – joins endothelial cells by occluding (tight) or communicating (gap) junctions

Arterial Cell Anatomy Smooth muscle cells • Located primarily in the medial layer • Contractile • Synthetic – sensitive to growth promoting factors (proliferative) and migrating factors • Regulates tone of arteries - via the sympathic/ parasympathic nervous system

Arterial Cell Anatomy Serous layer: – Outermost part – Contains blood supply to vessel wall – ‘Fastens’ vessels to surrounding tissue
 • Sclerosis (greek: sklerosis =")
Atherosclerosis • Athero (greek: athera = gruel, paste, porridge) • Sclerosis (greek: sklerosis = hard mass) • Atherosclerosis = build-up of fatty plaques and cholesterol in the arteries • Arteriosclerosis = thickening, hardening and loss of elasticity the arterial walls. 3 types: – Atherosclerosis – most common type of arteriosclerosis – Arteriosclerosis obliterans – sclerosis of median and large arteries of lower extremities – Monckeberg’s arteriosclerosis – calcific sclerosis of tunica media in extremities of elderly

Advanced/complicated lesion

Atherosclerosis • Slow and progressive disease • It may start in childhood, but usually does not become clinically detectable before the fifth decade or later
 - Epithelial dysfunction - Vascular inflammation - Buildup")
Atherosclerosis • Characterized by (large/medium-sized arteries) - Epithelial dysfunction - Vascular inflammation - Buildup within intima of: ◦ ◦ Lipids Cholesterol Calcium Cellular debris

Atherosclerosis • Results in - Plaque formation Vascular remodeling Acute & chronic luminal obstruction Abnormalities of blood flow Diminished O 2 supply to target organs

Normal artery vs. Atherosclerosis

Atherosclerosis • An incompletely understood interaction between critical cellular elements of the atherosclerotic lesion, involving: - Endothelial cells Smooth muscle cells Platelets Leukocytes

Atherosclerosis • Other elements involved - Vasomotor function The thrombogenicity of the blood vessel wall The activity of the coagulation cascade The fibrinolytic system Smooth muscle cell migration/proliferation Cellular inflammation

Atherosclerotic Process • Endothelial disruption/injury – the first step initiating a series of events: • endothelial permeability to: – lipoproteins – other plasma constituents such as leukocytes
, pp. 115–")
Endothelial Dysfunction in Atherosclerosis Ross, R. N Engl J Med 340 (1999), pp. 115– 126.

Atherosclerosis Intima is affected to the largest degree: 3 focal lesions which represent stages of the atherosclerotic process: 1. Fatty streaks 2. Fibrous plaques 3. Complicated lesions bleeding necrotic areas embolus aneurysm may rupture 2. and 3. are referred to as ‘raised lesions’ because they protrude into the lumen of the vessel

Atherosclerotic Process • Formation of Fatty streaks – Initially consist of: § Foam cells (Lipid-laden monocytes and macrophages) § T lymphocytes – Later they are joined by various numbers of § Smooth-muscle cells – The steps involved in this process include § smooth-muscle migration § foam-cell formation § platelet adherence and aggregation
, pp. 115–")
Fatty-Streak Formation in Atherosclerosis Ross, R. N Engl J Med 340 (1999), pp. 115– 126.

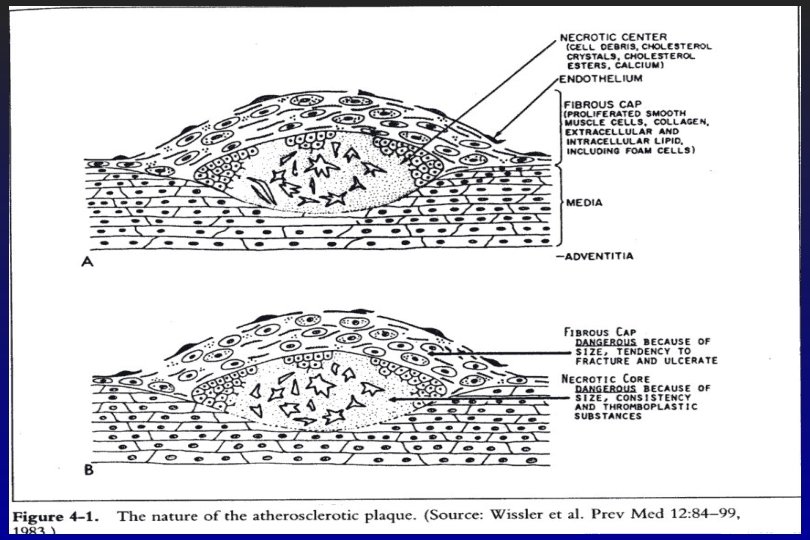
Formation of an Advanced, Complicated Lesion of Atherosclerosis • Fibrous cap formation – As fatty streaks progress to intermediate and advanced lesions, they tend to form a fibrous cap that walls off the lesion from the lumen – This represents a type of healing or fibrous response to the injury

Formation of an Advanced, Complicated Lesion of Atherosclerosis • Necrotic core formation – The fibrous cap covers a mixture of leukocytes, lipid, and debris, which may form a necrotic core. – These lesions expand at their shoulders by means of continued leukocyte adhesion and entry.

Formation of an Advanced, Complicated Lesion of Atherosclerosis Ross, R. N Engl J Med 340 (1999), pp. 115– 126.

Anatomy of the Atherosclerotic Plaque Fibrous cap Lumen Shoulder Lipid Core Intima Media Elastic laminæ Internal External

Atherosclerotic Process • Progression of atherosclerosis is non-linear – some lesions are stable over many years – some progress rapidly within months • Rupture of fissuring of plaques – from turbulent flow or chemical factors – may lead to mural thrombi (platelet aggregation) of varying sizes at these sites – Thrombi may be incorporated into the plaque during this process
, pp.")
Unstable Fibrous Plaques in Atherosclerosis Ross, R. N Engl J Med 340 (1999), pp. 115– 126.

Schematic Time Course of Atherosclerosis Ischemic Heart Disease Cerebrovascular Disease Peripheral Vascular Disease Lesion initiation No symptoms Symptoms Time (y) Symptoms

Clinical manifestation • A combination of atherosclerosis and platelet/Vessel Wall interaction • Pathological result: – ISCHEMIA (Greek: ischein = to hold back, Greek: naima = blood) – NECROSIS (Greek: necros = corps, dead)

Necrosis of myocardium - result of ischemia

Coronary Atherosclerosis and Coronary Blood Flow • Heart - completely aerobic organ • Coronary blood flow = “myocardial oxygen “supply” • Oxygen requirements of the myocardium = myocardial oxygen “demand” • At rest, myocardium extracts 85% or more of oxygen from blood • Exercise: 5 -6 fold increase in coronary blood flow • Atherosclerotic arteries – Limited ability to vasodilate – Deficient in EDRF* (nitric oxide) u increased likelihood of a mural thrombus *Endothelial Derived Relaxing Factor

Atherosclerosis and CAD • Coronary atherosclerosis can occur diffusely with occasional discrete, localized areas of more pronounced narrowing of the vessel lumen that may produce obstruction of blood flow • Described as “percent occlusion” or “percent stenosis” – Example 90% stenosis of the LAD • Obstructive coronary atherosclerosis is used to describe CAD that is severe enough to reduce blood flow • Coronary angiography is used to determine the severity of coronary atherosclerosis – coronary angiogram

EC = Endothelial cell SMC = Smooth muscle cells Ockene IS & JK: Prevention of CHD. 1992
")
Oxidative modification of LDL is central to sequence of events • Oxidized (or modified) LDL penetrates the endothelial surface 10 x easier than normal (native) LDL • Oxidized LDL triggers several other mechanisms important for ultimate formation of the fatty streak.

Characteristics of oxidized LDL • • • Cytotoxic – endothelial injury Chemotactic – attracts macrophages Motility inhibiting – inhibits out-migration of macrophages from the vessel wall • Increases the rate of oxidation of LDL Oxidative modification of LDL • Reduced – by antioxidants (Vit A, C, E, beta-carotene, selenium, etc) • Stimulated by endothelial injury

Elevated serum cholesterol levels - Associated with uptake by arteries of atherogenic lipoproteins - Seems to be a necessary prerequisite for initiating atherogenesis § Populations where other risk factors are present, but where the serum lipid levels are low, have very little atherosclerosis I. e. Japan – until recently low CHD risk Ø Large proportion of smokers Ø Large proportion with hypertension Ø Low serum cholesterol

Platelets • Normally circulate freely through the blood vessels • Normally do not adhere to the endothelial surface • Readily cling to damaged or dysfunctional endothelium

Interaction between platelets and vessel wall can initiate: • Local thrombus formation → Immediate occlusion of the vessel and thus blood supply → Serve as stimulus for subsequent vascular events

Ockene IS & JK: Prevention of CHD. 1992

Factors important for the platelet-vessel wall interactions and which are released from the endothelium • Prostacyclin (PGI 2) – is released in response to biochemical and mechanical mediators (tromboxane A 2, thrombin, bradykinin, histamine, HDL, tissue hypoxia, hemodynamic stress) – Potent vasodilator – Inhibits platelet aggregation • Endothelim-derived relaxing factor (EDRF) – nitric oxide (which is derived from Larginine (diet – nuts…) Is released in response to thrombin, bradykinin, thromboxane A 2, histamine, adenine, nucleotides and aggregating platelets. – Relaxes smooth muscles – Potent inhibitor of platelet adhesion and aggregation – Acts in synergism with PGI 2 • Angiotensin II – is converted from Angiotensin I by angiotensin-converting enzyme (ACE) Other enzymes from endothelium can also convert Angiotensin I to Angiotensin II

Factors important for the platelet-vessel wall interactions and which are released from the endothelium: • Endothelin – is released slowly – Smooth muscle contraction – Vasoconstrictor – 10 x more potent than Angiotensin II • Plasminogen activators – is released in response to epinephrine, thrombin, heparin, interleukin-1, venous occlusion, aggregating platelets, etc – Generate plasmin locally → fibrinolysis by proteolytically degrading fibrin • Plasminogen-activator inhibitor (PAI-1) – Inhibits fibrinolysis

Factors important for the platelet-vessel wall interactions and which are released from the endothelium: • Heparin-like species – anticoagulant • Platelet-activating factor (PAF) – is a lipid – induces platelet aggregation by mobilizing platelet surface membrane arachidonic acid, which stimulates thromboxane A 2 synthesis • Tissue factor or tissue thromboplastin – Activates Factor X by activating factor VIIa • Von Willebrand factor

Not clear what initiates the process of atherosclerosis “Response to injury” - the most accepted hypothesis Some kind of injury to the endothelium initiates the process of atherosclerosis: • • Mechanical – non-laminar blood flow, hypertension Infection – Viral? : Herpes simplex, cytomegalovirus - Bact. ? : Chlamydia pneumonia, helicobacter pylori. Hyperlipidemia – seems mandatory for atherosclerosis to occur Diabetes Mellitus – Hyperlipidemia, modified lipoprotein, growth factors, chemoattractants, increased serum glucose Toxins – smoking, hypoxia, antioxidants Immunologic factors – I. e. Transplant rejection, collagen vascular diseases Hereditary factors – I. e. Homocysteinuria, Plasminogen activator deficiency
- Slides: 46