ENVIRONMENTAL NUTRITIONAL PATHOLOGY Environmental and Nutritional Pathology Environment




, makes them less lipophilic by adding")





-1")







 n n C =")






 n Oral Contraceptives (BCPs) n Hormone Replacement Therapy (HRT) n Acetaminophen")
 n Breast cancer and other cancers n n Thromboembolic events n")
 n Cancer n n in women with a uterus combined")
 Does not affect cyclooxygenase so bleeding associated with aspirin does not occur")
 n n respiratory alkalosis followed")
 constitutively expressed")



 n")





Curie vs. (M)Becqerel IONIZING vs. NON-IONIZING PARTICULATE vs.")





 n n Vascular effects n n")
 CHRONIC (fibrosis)")






")








 reported the results of a large North")

 all require")

- Slides: 76
ENVIRONMENTAL & NUTRITIONAL PATHOLOGY
Environmental and Nutritional Pathology Environment and Disease n Common Exposures n Environmental n Occupational n n Nutrition and Disease
Reported Occupational Diseases Disease Number Repeated trauma 276, 600 64 57, 900 20, 300 13 5 16, 600 5, 100 2, 900 4 1 1 50, 600 430, 000 12 100 Skin disorders Lung conditions due to toxic exposures Physical injury Poisoning Lung disease due to dusts All other illnesses Total Percentage
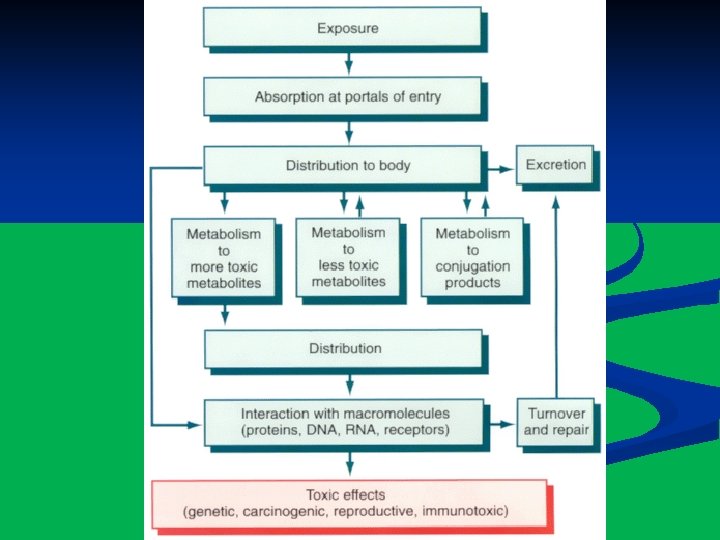
Mechanisms of Toxicity n “Threshold” effect n Absorption at portals of entry ingestion n inhalation n skin contact n Distribution within the body n Metabolism and Excretion n Toxic effects n
Xenobiotic Mechanisms n Phase I Reactions (Smooth ER), makes them less lipophilic by adding a direct polar group Cytochrome P-450 -dependent monooxygenase system n Flavin-containing monooxygenase system n Peroxidase-dependent cooxidation n n Phase II Reactions, combines them with other polar substances Glucuronidation n Biomethylation n Glutathione conjugation n
Contents of Toxic Waste Dumps Acetone Aldrin/Dieldrin Arsenic DDT, DDE, DDD 1, 1 and 1, 2 -Dichloroethane Lead Barium Benzene 2 -Butanone Cadmium Carbon tetrachloride Chlordane Chloroform Chromium Cyanide Mercury Methylene chloride Nickel Pentachlorophenol Polychlorinated biphenyls Tri- and Tetrachloroethylene Toluene Vinyl Chloride Zinc
Dose-response Curve
Common Exposures n Personal n Medications n Outdoor Air Pollution n Industrial Exposures n Agricultural Hazards n Natural Toxins n Radiation Injury n Physical Injury
Tobacco n 440, 000 premature deaths/year in USA n cancer n cardiovascular disease n respiratory disease n cerebrovascular disease n $150 billion in health related costs n. By far the most preventable
Tobacco and Cancer n 70% of all lung cancers* n 30% of all cancers
Organ-Specific Carcinogens in Tobacco Smoke Organ Lung, larynx Carcinogen Polycyclic aromatic hydrocarbons 4 -(Methylnitrosoamino)-1 -(3 -pyridyl)-1 -buta-none (NNK) Polonium 210 Esophagus N'-Nitrosonornicotine (NNN) Pancreas NNK (? ) Bladder 4 -Aminobiphenyl, 2 -naphthylamine Oral cavity (smoking) Polycyclic aromatic hydrocarbons, NNK, NNN Oral cavity (snuff) NNK, NNN, polonium 210 Data from Szczesny LB, Holbrook JH: Cigarette smoking. In Rom WH (ed): Environmental and Occupational Medicine, 2 nd ed. Boston, Little, Brown, 1992, p. 1211.
Relative Risks for Current Smokers of Cigarettes Disease or Condition Males Females Coronary heart disease Age 35– 64 2. 8 3. 1 Age ≥ 65 1. 6 Age 35– 64 3. 3 4 Age ≥ 65 1. 6 1. 5 Aortic aneurysm 6. 2 7. 1 Chronic airways obstruction 10. 6 13. 1 Lip, oral cavity, pharynx 10. 9 5. 1 Esophagus 6. 8 7. 8 Stomach 2 1. 4 Pancreas 2. 3 Larynx 14. 6 13 Lung 23. 3 12. 7 Cerebrovascular lesions Cancer Cervix 1. 6 Kidney 2. 7 1. 3 Bladder, other urinary organs 3. 3 2. 2
Cigarettes And The Workplace Similar to asbestos exposure, cigarette smoke is “synergistic” with radon decay products in causing lung cancer n Cigarette smoke exacerbates bronchitis, asthma, and pneumoconiosis associated with exposure to silica, coal dust, grain dust, cotton dust, and welding fumes (DUH) n
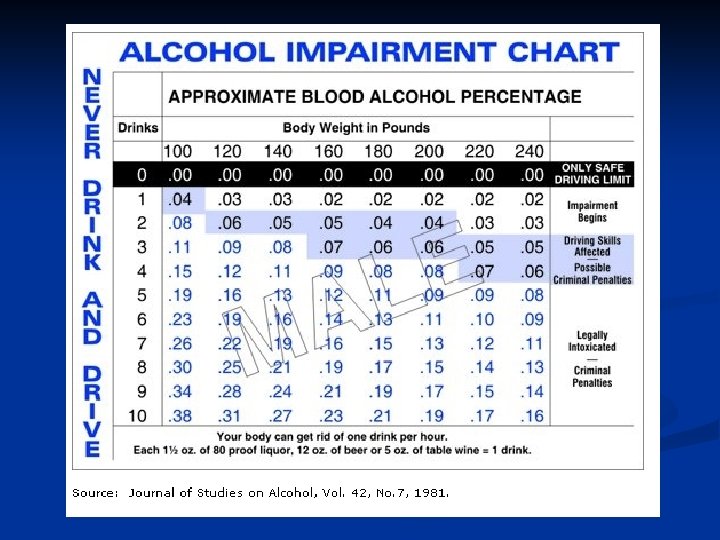
Alcohol n 15 to 20 million alcoholics in the USA n 100, 000 deaths/year due to alcohol abuse n Economic losses of $100 to $130 billion/year n One to two drinks/day reduces * What kindof of person would put this kind of shit on incidence coronary artery a powerpoint? disease* A) Drinker? B) Non-Drinker? C) Alcoholic in Denial?
Definition of Alcoholism ?
Effects of Blood Alcohol Levels in the Absence of Tolerance Blood Level, mg/d. L Usual Effect 20 80 200 300 400 Decreased inhibitions, a slight feeling of intoxication Decrease in complex cognitive functions and motor performance Obvious slurred speech, motor incoordination, irritability, and poor judgment Light coma and depressed vital signs Death Harrison Internal Med, 16 th
Metabolism Of Ethanol 20% 80% CTP 2 E 1, a P 450 oxidase; ADH, alcohol dehydrogenase; ALDH, aldehyde dehydrogenase
LEGAL INTOXICATION 0. 08% = BAC = % BY VOLUME
Widmark Equation n C = A / (W * r) n n C = concentration of Et. OH in mg/dl A = mass of alcohol ingested in grams n n n W = body weight in grams r = Widmark distribution for ethanol n n n 0. 55 m. L/ g body weight for females 0. 68 m. L / g body weight for males Elimination of ethanol = 0. 015%/h 0. 015%/ (15 mg/dl/h (15 mg/dl/ ) n n density of ethanol = 0. 8 zero order kinetics, i. e. , is INDEPENDENT of the amount of reactants. Medical measurements use mg/dl in plasma, whereas legal definitions use percentage (mass/volume) in whole blood n to estimate the alcohol level in whole blood using the alcohol level in blood plasma, divide by 1. 16
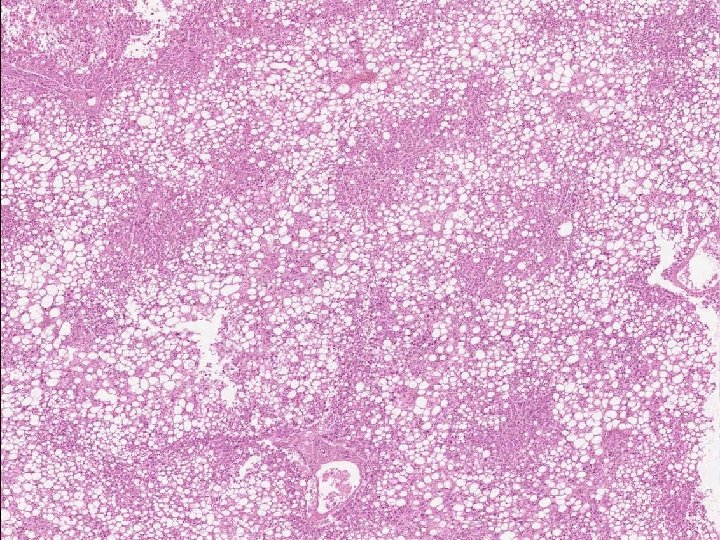
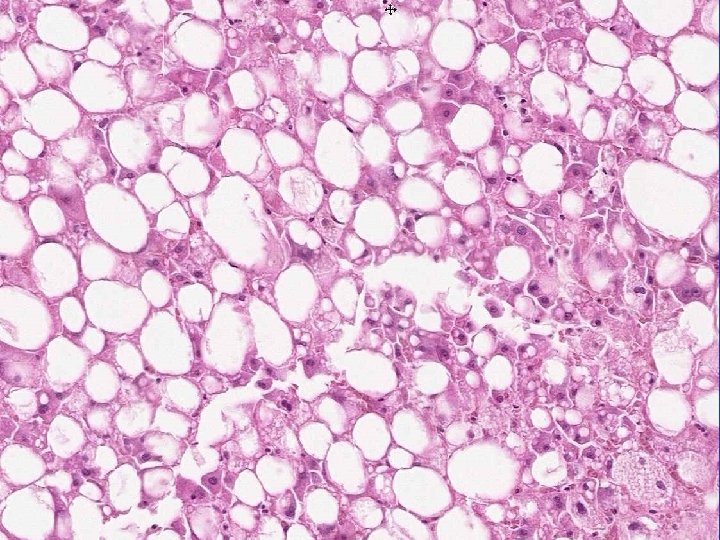
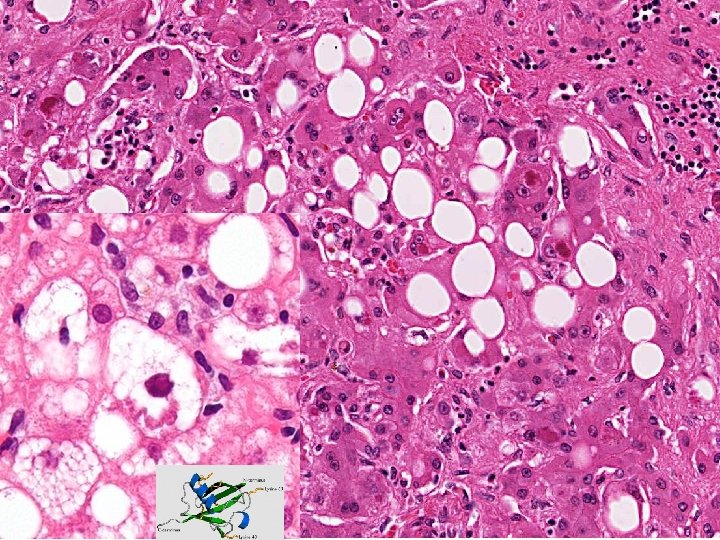
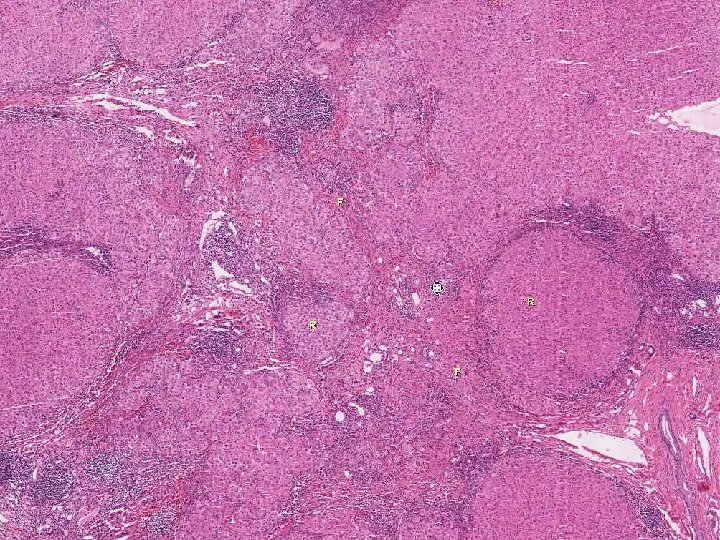
n Alcohol and the Liver Fatty Change n n n Alcohol hepatitis n n n present in over 90% of binge and chronic drinkers liver is enlarged but patient is asymptomatic changes are reversible with cessation of drinking macrosteatosis w/o inflammation or necrosis only between 10 - 15% of alcoholics will develop alcoholic hepatitis may have systemic symptoms and jaundice hepatocellular necrosis with Mallory bodies and PMNs (central hyaline sclerosis) thought to be a precursor of cirrhosis probably more than HALF will go onto cirrhosis if ETOH is not stopped Alcoholic cirrhosis n shrunken nodular liver with uniform small nodules (micronodular cirrhosis)
Fatty Change Biochemistry Catabolism of fat by peripheral tissues is increased, and there is increased delivery of free fatty acids to the liver n An excess of NADH over NAD stimulates lipid biosynthesis n Oxidation of fatty acids by mitochondria is decreased n Acetaldehyde forms adducts with tubulin and impairs function of microtubules, resulting in decreased transport of lipoproteins from the liver n
Neurologic Manifestations of Alcoholism n Wernicke syndrome n confusion, ataxia, and diplopia from ophthalmoplegia damage to mammillary bodies, cerebellum and periaqueductal gray matter of the midbrain n due to thiamine deficiency n may respond to prompt thiamine replacement n n Korsakov syndrome memory loss and confabulation n results from thiamine deficiency and direct n
Limbic system
Mechanisms of Disease Caused by Ethanol Abuse Organ System Liver Lesion Fatty change Mechanism Toxicity Acute hepatitis Alcoholic cirrhosis Nervous system Cardiovascular system Wernicke syndrome Thiamine deficiency Korsakoff syndrome Toxicity and thiamine deficiency Cerebellar degeneration Nutritional deficiency Peripheral neuropathy Thiamine deficiency Cardiomyopathy Toxicity Hypertension Vasopressor
Mechanisms of Disease Caused by Ethanol Abuse Organ System Gastrointestinal tract Skeletal muscle Lesion Gastritis Toxicity Pancreatitis Toxicity Rhabdomyolysis Toxicity Reproductive system Testicular atrophy Fetal alcohol syndrome Mechanism ? Spontaneous abortion ? Growth retardation Toxicity Mental retardation Birth defects
Therapeutic Drugs (Medications) n Oral Contraceptives (BCPs) n Hormone Replacement Therapy (HRT) n Acetaminophen n Aspirin
Oral Contraceptives (BCPs) n Breast cancer and other cancers n n Thromboembolic events n n n DVT and Pulmonary Embolism increased adds to other risk factors (e. g. Factor V Leiden) Cardiovascular disease n no increase in breast cancer decrease endometrial and ovarian cancers increase in cervical cancer (? lifestyle induced) with current low estrogen pills, risk of MI and atherosclerosis not increased in non-smoking women < 45 y ischemic stroke increased regardless of age or smoking Liver tumors n n benign hepatic adenomas older women with prolonged use
Hormone Replacement Therapy (HRT) n Cancer n n in women with a uterus combined estrogen and progestin Rx necessary to reduce endometrial cancer WHI showed increased risk of breast cancer in women who used HRT combined therapy for 5 years n Thromboembolic n elevated approximated twofold in HRT users, especially within the first 2 years n Cardiovascular n events disease WHI reported 29% increased risk of myocardial infarction, especially during the first year of
Acetaminophen (Tylenol) Does not affect cyclooxygenase so bleeding associated with aspirin does not occur n Has analgesic and antipyretic actions but no anti-inflammatory action n Large doses may produce hepatic necrosis n patients should not exceed recommended dose (4 grams/day) n toxic dose in adults is 15 to 25 gm n dose should be reduced in children with n
Aspirin n Overdose n n Chronic aspirin toxicity (salicylism) n n respiratory alkalosis followed by metabolic acidosis that may be fatal headache, dizziness, ringing in the ears (tinnitus), mental confusion, drowsiness, nausea, vomiting, and diarrhea Inhibits cyclooxygenases (COX 1 & 2) Erosive gastritis is a major cause of GI bleeding May be implicated in Reye syndrome (fatty liver with encephalopathy) in children < 15 years old, especially with influenza and
Cox-1 and Cox-2 Inhibitors n Cyclooxygenase 1 (inhib of COX-1 is BAD) constitutively expressed and active in the normal platelet (thromboxane A 2) n involved in synthesis of gastro-protective prostaglandins n n Cyclooxygenase 2 (inhib of COX-2 is GOOD) induced, especially in inflamed tissue n in vessel wall produces prostacyclin (PGI 2) n n Aspirin and other nonselective NSAIDS inhibit both COX-1 and COX-2
Figure 2 -16 Generation of arachidonic acid metabolites and their roles in inflammation. The molecular targets of action of some anti-inflammatory drugs are indicated by a red X. COX, cyclooxygenase; HETE, hydroxyeicosatetraenoic acid; HPETE, hydroperoxyeicosatetraenoic acid. Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 15 August 2005 06: 35 PM) © 2005 Elsevier
Indoor Air Pollution n Carbon Monoxide CO n Nitrogen Dioxide NO 2 (from acid rain) n Wood Smoke n Formaldehyde n. Radon n Manufactured Mineral Fibers
Radon is a radioactive gas and a decay product of uranium, naturally occurring n It is widely distributed in the soil and is prevalent in homes (especially in basements) n Radon decay products are alpha emitters n 10% of US homes have levels associated with an increased risk of lung cancer and an estimated 10, 000 lung cancers per year in the United States are due to radon. n
Lead is classified as a heavy metal (others include mercury, arsenic, and cadmium) n Source of exposure n lead paint n lead solder in plumbing (older houses) n lead-glazed ceramics n industrial exposure n n Route of exposure inhalation with industrial exposure n ingestion with household exposure n
Lead Distribution and Excretion n Lead is a divalent cation that is taken up by bone and developing teeth in children (80% to 85%) n n Half-life of lead in bone is 30 years Blood accumulates 5% to 10% of lead, but lead is rapidly cleared from the blood lead in blood indicates recent exposure n blood level does not allow the determination of total body burden n n Remainder is distributed in the soft tissues
Effects of Lead n High affinity for sulfhydryl groups n n Competition with calcium ions n n n inhibition of heme biosynthesis with hypochromic anemia and basophillic stippling of erythrocytes As a divalent cation, lead competes with calcium and is stored in bone. It also interferes with nerve transmission and brain development. Inhibition of membrane-associated enzymes n Lead inhibits 5'-nucleotidase activity and sodiumpotassium ion pumps, leading to decreased survival of red blood cells (hemolysis), renal damage, and hypertension.
Consequences of lead exposure
“RADIATION” n n n n T½ (m)Curie vs. (M)Becqerel IONIZING vs. NON-IONIZING PARTICULATE vs. NON-PARTICULATE (Photons) ENERGY: Kev, Mev (~Wavelength) Linear Energy Transfer (LET), Relative Biologic Effect (RBE) LD 50@60 d
This is the single most RADIOSENSITIVE CELL In your body
Radiation Dosimetry n Roentgen: unit of charge produced by x-rays or gamma rays that ionize a specific volume of air. Physics unit. n RAD (radiation absorbed dose): the dose of n n n radiation that will produce absorption of 100 ergs of energy per gram of tissue; 1 gm of tissue exposed to 1 roentgen of gamma rays is equal to 93 ergs Gray (Gy): the dose of radiation that will produce absorption of 1 joule of energy per kilogram of tissue; 1 Gy corresponds to 100 rad (SI unit for absorbed dose) REM (radiation equivalent man): the dose of radiation that causes a biologic effect equivalent to 1 rad of x-rays or gamma rays Sievert (Sv): the dose of radiation that causes a biologic effect equivalent to 1 Gy of x-rays or gamma
Acute Effects of Ionizing Radiation n Free n radical generation Ionizing radiation + H 20 → H 30+ + OH· n DNA Damage double-stranded DNA breaks needed to kill cell (mammalian cells can repair single stranded breaks) n cross-linking of DNA strands, cleavage of sugar-phosphate bonds n n Tumor-suppressor gene p 53 activation n cell cycle arrest in presence of damaged DNA
Acute Whole Body Radiation n LD 50 @ 6 wks 2. 5 to 4. 0 Gy (250 to 400 rad) n Hematopoietic n n n Gastrointestinal n n 200– 600 REM Maximum neutrophil and platelet depression in 2 wk 600– 1000 REM Nausea, vomiting, diarrhea Hemorrhage and infection in 1– 3 wk Central nervous system n n n >1000 REM Intractable nausea and vomiting Confusion, somnolence, convulsions
Therapeutic Radiation External radiation is delivered to malignant neoplasms at fractionated doses up to 40 to 70 Gy (4000 to 7000 rad), with shielding of adjacent normal tissues n Therapeutic radiation alone seems to add little risk of AML but can increase the risk in people exposed to alkylating agents n Fatigue, nausea and vomiting frequent n Bone marrow suppression may occur n
Delayed Radiation Injury n Carcinogenesis (atom bomb survivors) n n Vascular effects n n n myeloid leukemias peak 5 to 7 years after exposure breast and thyroid cancers may show greater latency no germline mutations noted in progeny of survivors endothelial necrosis followed by intimal and medial fibrosis capillaries may become thrombosed and obliterated or ectatic Parenchymal atrophy and fibrosis
Radiation effects on TISSUE n n ACUTE (vasculitis, possibly “fibrinoid” necrosis) CHRONIC (fibrosis)
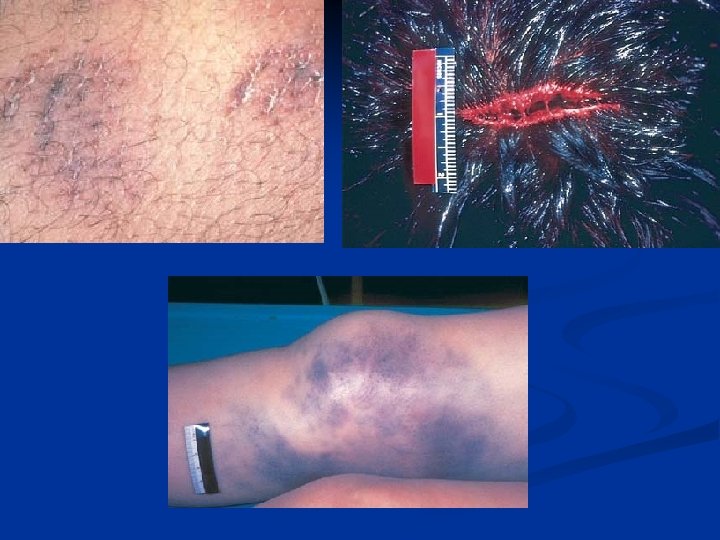
Physical Injury n Abrasion n n basically a scrape superficial epidermis is torn off by friction or force regeneration without scarring usually occurs Laceration vs. Incision n n a laceration is an irregular tear in the skin produced by overstretching. The wound margins are frequently hemorrhagic and traumatized an incision is made by a sharp cutting object. The margins of the incision are usually relatively clean n Contusion n an injury caused by a blunt force that damages small blood vessels and causes interstitial bleeding, usually without disruption of the continuity of the tissue (cf ecchymosis)
Adult Mortality Rates in the United States, Ages 25– 44, in 1998 Rate per 100, 000 population Cause Hispanic Black White Unintentional injuries 33. 4 40. 1 31. 6 Cancer 16. 8 38. 0 25. 3 Homicide 13. 1 Human immunodeficiency virus 12. 1 36. 2 43. 3 4. 7 4. 8 Heart disease 10. 3 43. 5 18. 3 Suicide Total 7. 8 — 17. 0 130. 2 303. 7 139. 4 Data from CDC Fact Book, 2000/2001, Department of Health and Human Services, Centers for Disease Control and Prevention.
GUNSHOT WOUND n Entrance Vs. Exit n Far range Vs. Close range NOT CLOSE RANGE (POWDER BURNS) EXIT WOUNDS are generally SLOPPIER than ENTRANCE
BURNS n n n 1 st, 2 nd, 3 rd, 4 th “Degree” FULL vs. PARTIAL Thickness Survival PERCENT of body using the rule of NINES n DEGREE (i. e. , Depth) n Respiratory Tract Involvement n AGE n Speed of access to Burn Unit n Immune System (Pseudomonas, S. aureus, Candida), infections are usually the lethal delayed cause of death. n
HYPER-THERMIA n HEAT n CRAMPS: Electrolyte loss via sweat n EXHAUSTION: Water depletion and lack of cardiovascular compensation n “STROKE”: Extensive peripheral vasodilatation, i. e. , “shocky”, very serious, T>106º, over 110º have been reported, high mortality. In this case true “SHOCK” would be a better term than “STROKE”
HYPO-THERMIA n Often in setting of homelessness or alcoholism or both n< 90º often fatal, assoc. w. BRADYCARDIA n ATRIAL FIBRILLATION n
LIGHTNING/ELECTRICAL n ELECTRIC DISTURBANCES NEURAL (because nerve is such an EXCELLENT conductor of electricity) n EKG (like reverse cardioversion) n n n THERMAL INJURY, directly proportional to a particular tissue’s RESISTANCE to electrical flow “LIGHTNING” MARKS
ATMOSPHERIC PRESSURE n Altitude Illness n Blast Injuries n Decompression Injuries
ALTITUDE ILLNESS n Caused by LOW Oxygen Tension HIGH ALTITUDES (>4000 m [12, 000 feet]) n OBTUNDATION n INCREASED CAPILLARY PERMEABILITY n ACUTE PULMONARY EDEMA (HAPE) n Q: What is the name of the base camp at Mt. Everest A: Pulmonary Edema
BLAST INJURIES n RELATED TO RAPID ATMOSPHERIC PRESSURE CHANGES LUNGS n VISCERA, especially GAS filled viscera n n n Rupture, Hemorrhage, etc. IMMERSION BLAST also possible, causing more of a total body compression syndrome
DECOMPRESSION n n Related to GAS SOLUBILITY in divers ascending rapidly, especially the more NON-SOLUBLE gasses, like NITROGEN, and, to a lesser extent, XENON AIR EMBOLISM is the common pathology n ACUTE: n “BENDS” (peri-articular), acute n “CHOKES” (lungs), acute n “STAGGERS” (inner ear), acute n CHRONIC:
NUTRITION & DISEASE n Food Safety n Additives n Contaminants n Nutritional Deficiencies n Vitamins n Minerals n Obesity n Diet and Disease n Chemoprevention of Cancer
Vitamin Deficiency and Excess n Fat soluble vitamins A, D, E, K n readily stored in body fat n poorly absorbed in digestive disorders involving malabsorbtion of fat n n Water soluble vitamins remaining vitamins n readily excreted in urine n n Vitamin stores (fat stores longer than water) n vitamins B-12 and A: stores sufficient for 1 year
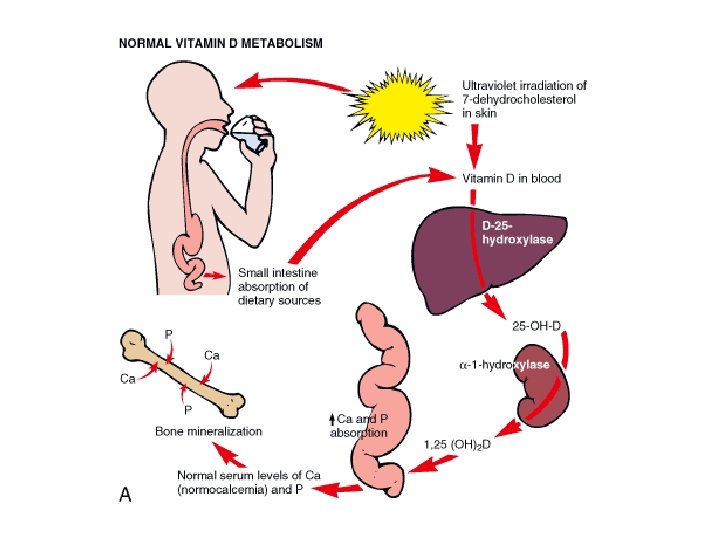
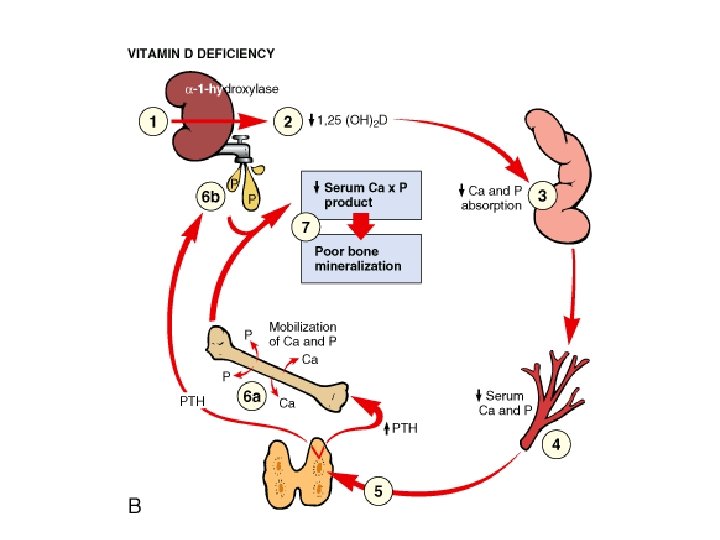
Vitamin D Metabolism n n Absorption of vitamin D in the gut or synthesis from precursors in the skin Binding to a plasma α 1 -globulin (Dbinding protein) and transport to liver Conversion to 25 -hydroxyvitamin D, 25(OH)D (calcidol) by 25 -hydroxylase in the liver Conversion of 25(OH)D to 1, 25(OH)2 D (calcitrol, Vitamin D 3) by α 1 hydroxylase in the kidney; biologically this is the most active form of vitamin
Functions of Vitamin D Stimulates intestinal absorption of calcium and phosphorus n Collaborates with PTH in the mobilization of calcium from bone n Stimulates the PTH-dependent reabsorption of calcium in the distal renal tubules n 1, 25(OH)2 D, the biologically active form of vitamin D, is best regarded as a steroid hormone which acts by binding to a high-affinity receptor n
Vitamin D Deficiency Holick et al (2005) reported the results of a large North American study that assessed the vitamin D status of postmenopausal women receiving therapy to treat or prevent osteoporosis n 52% of 1536 women had inadequate [25(OH)D] levels (<30 ng/m. L) n 36% and 18% had levels less than 25 and 20 ng/m. L, respectively. n Holick MF et al: J Clin Endocrinol Metab 90: 3215, 2005
Vitamin D Deficiency n Childhood: Rickets n epiphyses are open n cartilage overgrowth n Adults: osteomalacia n bone matrix is not calcified n vs osteoporosis (matrix reduced) ADULTS ßCHILDREN (RICKETS) OSTEOMALACIA 1) Bone fractures that happen with very little injury 2) Muscle weakness 3) Widespread bone pain,
Vitamin K n Clotting factors VII, IX, and X and prothrombin (II) all require carboxylation of glutamate residues for functional activity n anticoagulant coumadin is a Vitamin K antagonist Activation of anticoagulant proteins C and S also requires glutamate carboxylation n Sources n n endogenous intestinal bacterial flora
Vitamin K Deficiency n Causes fat malabsorption n reduced gut bacterial flora n n administration of wide specturm antibiotics n neonatal period before gut is colonized n n liver disease with reduced recycling of vitamin K Effects of vitamin K deficiency bleeding diathesis n estimated 3% prevalence of vitamin Kdependent bleeding diathesis among neonates warrants routine prophylactic n