Enhanced Recovery after Esophagectomy Joint Hospital Surgical Grand







 is applicable 1 • TIME trial")





















 452 451 P=0. 625 Blood loss")
- Slides: 35
Enhanced Recovery after Esophagectomy Joint Hospital Surgical Grand Round 10 -8 -19 Cheung Siu Hong United Christian Hospital
ERAS • Enhanced Recovery after surgery • Multidisciplinary team collaboration to maximize the efficiency of surgical recovery 1 • Promote earlier return to normal physiology 2, 3 1. 2. 3. http: //erassociety. org/ Fearon KC, Ljungqvist O, Von MM et al (2005) Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 24: 466– 477 Ljungqvist O, Scott M, Fearon KC (2017) Enhanced recovery after surgery: a review. JAMA Surg 152: 292– 298
Pre-operative Intra-operative ERAS Post-operative
Pre-operative Intra-operative ERAS Post-operative
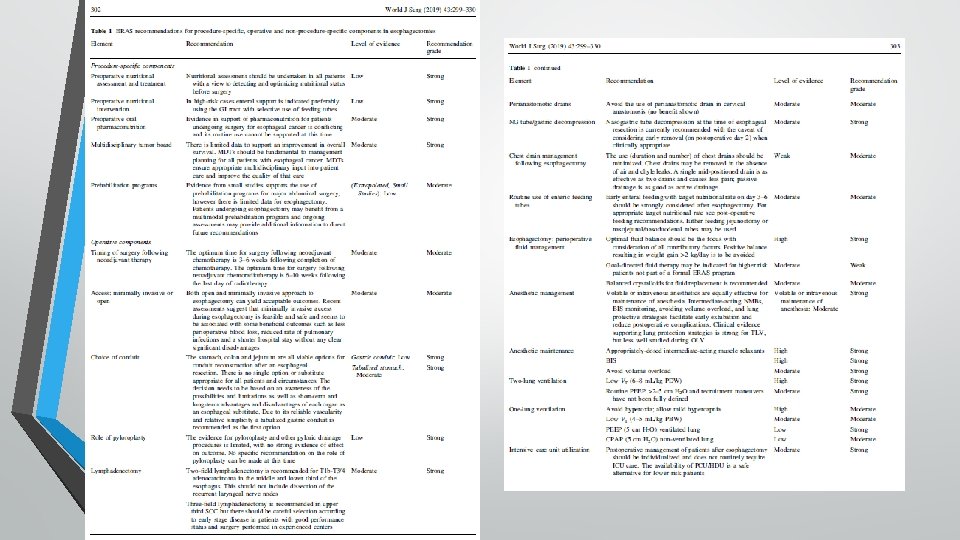
Pre-operative • Multidisciplinary tumor board assessment • Preoperative nutritional assessment + treatment • Prehabilitation • Patient counselling • Prolonged fasting should be avoided, and clear liquids, including specific preoperative high-carbohydrate drinks, should be allowed until 2 h prior to esophagectomy.
Pre-operative Intra-operative ERAS Post-operative
Pre-operative Intra-operative ERAS Post-operative
Intra-operative • Both open or minimal invasive esophagectomy(MIE) is applicable 1 • TIME trial showed similar anastomotic leak rate and number of lymph nodes retrieved, similar 30 -day mortality • Lymphadenectomy 2 • two-field lymphadenectomy is recommended for T 1 b-T 3/4 ACA in the middle and lower third of the esophagus • three-field lymphadenectomy is recommended in upper third SCC • tubulized gastric conduit is recommended as the first option due to it reliable vascularity, good outcome and relative simplicity 3 • Choice of conduit - stomach, colon and jejunum all are viable 1. Biere SS, van Berge Henegouwen MI, Maas KW et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomized controlled trial. Lancet (2012) 379: 1887– 1892 2. Hiranyatheb P, Osugi H. Radical lymphadenectomy in esophageal cancer: from the past to the present. Dis Esophagus(2015) 28: 68– 77 3. Akkerman RD, Haverkamp L, van Hillegersberg R et al. Surgical techniques to prevent delayed gastric emptying after esophagectomy with gastric interposition: a systematic review. Ann Thorac Surg(2014) 98: 1512– 1519
Intra-operative • The use of perianastomotic drain in cervical anastomosis may be avoided • does not give clinical information on leakage because it is often removed before the manifestation of anastomotic leak 1 • The use of chest drains should be minimized (duration and number) • one drain was as effective as two drains and resulted in less postoperative pain and earlier discharge from hospital 2 • • passive chest drainage was as effective as active drainage 3 fluid re-accumulation and re-intervention rates did not increase at a threshold of 200 ml/day 4 1. Choi HK, Law S, Chu KM et al. The value of neck drain in esophageal surgery: a randomized trial. Dis Esophagus(1998) 11: 40 -42 2. Gomez-Caro A, Roca MJ, Torres J et al. Successful use of a single chest drain post-lobectomy instead of two classical drains: a randomized study. Eur J Cardiothorac Surg(2006) 29: 562– 566 3. Johansson J, Lindberg CG, Johnsson F et al. Active or passive chest drainage after oesophagectomy in 101 patients: a prospective randomized study. Br J Surg(1998) 85: 1143– 1146 4. Hessami MA, Najafi F, Hatami S. Volume threshold for chest tube removal: a randomized controlled trial. J Inj Violence Res(2009) 1: 33– 36
Intra-operative • Nasogastric tube decompression at the time of esophageal resection is currently recommended with the caveat of considering early removal 1 1. 2. • no NG tube utilization showed that higher instances of pulmonary complications • no difference in pulmonary or other complications in comparison between the early (POD 2) and delayed NG tube removal. Mistry RC, Vijayabhaskar R, Karimundackal G et al. Effect of short-term vs prolonged nasogastric decompression on major postesophagectomy complications: a parallel-group, randomized trial. Arch Surg(2012) 147: 747– 751 Picture from https: //www. healthproductsforyou. com/
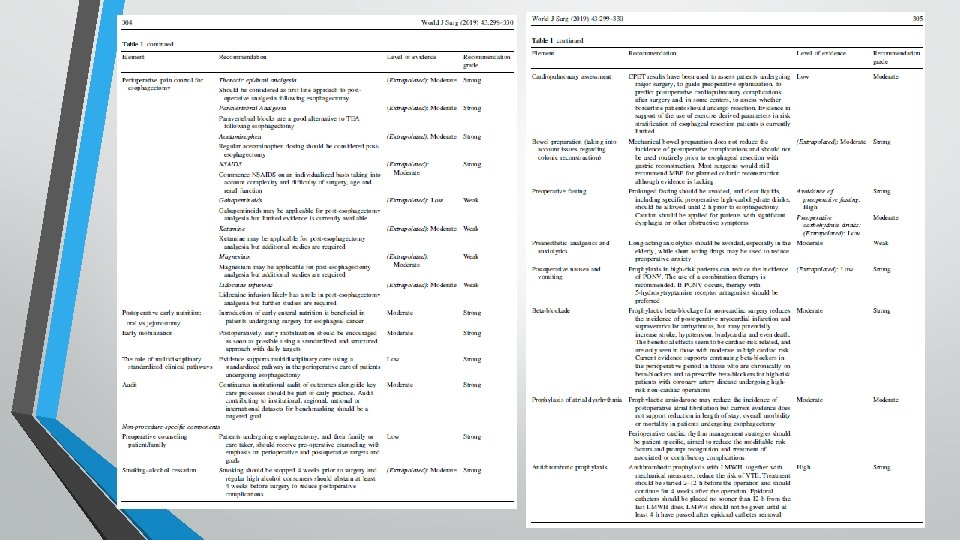
Intra-operative • Antithrombotic prophylaxis • Anaesthetic management • • consideration of short acting agent Lung protective ventilation • Optimal fluid balance should be the focus • Avoid positive balance • Maintain normothermia
Pre-operative Intra-operative ERAS Post-operative
Pre-operative Intra-operative ERAS Post-operative
Post operative • Does not routinely require ICU care • • • with better pain control and MIE, immediate extubation has become more common HDU is a safe alternative for lower risk patients retrospective analysis has shown large variation in the use of ICU after major surgery without any impact on outcome 1 1. Wunsch H, Gershengorn HB, Cooke CR et al. Use of intensive care services for medicare beneficiaries undergoing major surgical procedures. Anesthesiology(2016) 124: 899– 907
Post operative • Introduction of early enteral nutrition is beneficial in patients undergoing surgery for esophageal cancer 1 • • • oral/ tube feeding/ feeding jejunostomy with their own pros and cons 2 early enteral feeding target nutritional rate on day 3– 6 should be strongly considered after esophagectomy 2 • Early removal of drains and tubes 1. Mazaki T, Ebisawa K. Enteral versus parenteral nutrition after gastrointestinal surgery: a systematic review and metaanalysis of randomized controlled trials in the English literature. J Gastrointest Surg(2008) 12: 739– 755 2. Weijs TJ, Berkelmans GH, Nieuwenhuijzen GA et al. Routes for early enteral nutrition after esophagectomy: a systematic review. Clin Nutr(2015) 34: 1– 6
Post operative • Thoracic epidural analgesia should be considered as first line approach to post-operative analgesia following esophagectomy 2 • paravertebral blocks are good alternative as showed in meta-analysis 3 • Regular acetaminophen dosing should be considered post-esophagectomy. • NSAIDS on an individualized basis • Combination therapy for post operative nausea and vomiting suggested 2. Flisberg P, Tornebrandt K, Walther B et al. Pain relief after esophagectomy: thoracic epidural analgesia is better than parenteral opioids. J Cardiothorac Vasc Anesth(2001) 15: 282– 287 3. Davies RG, Myles PS, Graham JM. A comparison of the analgesic efficacy and side-effects of paravertebral vs epidural blockade for thoracotomy: a systematic review and meta-analysis of randomized trials. Br J Anaesth(2006) 96: 418– 426
Post operative • Early mobilization should be encouraged • Avoid hyperglycemia • Continuous audit
Future trend
Future Trend • Shifting towards ERAS • Small retrospective studies showed its feasibility and safety • Expecting more studies and results
Conclusion • ERAS esophagectomy provided the current best evidence based practice • Early review of outcome showed that it is feasible without compromising patient’s safety • Continuous audit is required
Reference 1. 2. 3. 4. http: //erassociety. org/ Fearon KC, Ljungqvist O, Von MM et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr (2005) 24: 466– 477 Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg (2017) 152: 292– 298 Nelson G, Altman AD, Nick A, et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations – Part I. Gynecologic Oncology. (2016. b) 140(2): 313– 322. 5. 6. 7. 8. 9. Thorell, A. , Mac. Cormick, A. D. , Awad, S. et al. Guidelines for Perioperative Care in Bariatric Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J Surg (2016) 40: 2065. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. Blom, R. L. G. M. , van Heijl, M. , Bemelman, W. A. et al. Initial Experiences of an Enhanced Recovery Protocol in Esophageal Surgery. World J Surg (2013) 37: 2372. 22. 23. 24. Mazaki T, Ebisawa K. Enteral versus parenteral nutrition after gastrointestinal surgery: a systematic review and metaanalysis of randomized controlled trials in the English literature. J Gastrointest Surg(2008) 12: 739– 755 Melloul, E. , Hübner, M. , Scott, M. et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J Surg (2016) 40: 2425. Gustafsson, U. O. , Scott, M. J. , Hubner, M. et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J Surg (2019) 43: 659. Findlay JM, Gillies RS, Millo J et al. Enhanced recovery for esophagectomy: a systematic review and evidence-based guidelines. Ann Surg (2014) 259: 413– 431 S. Giacopuzzi, J. Weindelmayer, E. Treppiedi et al. Enhanced recovery after surgery protocol in patients undergoing esophagectomy for cancer: a single center experience, Diseases of the Esophagus, Volume 30, Issue 4, April 2017, Pages 1– 6 Low DE, Allum W, De Manzoni G et al. Guidelines for Perioperative Care in Esophagectomy: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J Surg (2019) 43: 299– 330 Biere SS, van Berge Henegouwen MI, Maas KW et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomized controlled trial. Lancet (2012) 379: 1887– 1892 Hiranyatheb P, Osugi H. Radical lymphadenectomy in esophageal cancer: from the past to the present. Dis Esophagus(2015) 28: 68– 77 Akkerman RD, Haverkamp L, van Hillegersberg R et al. Surgical techniques to prevent delayed gastric emptying after esophagectomy with gastric interposition: a systematic review. Ann Thorac Surg(2014) 98: 1512– 1519 Choi HK, Law S, Chu KM et al. The value of neck drain in esophageal surgery: a randomized trial. Dis Esophagus(1998) 11: 40 -42 Gomez-Caro A, Roca MJ, Torres J et al. Successful use of a single chest drain postlobectomy instead of two classical drains: a randomized study. Eur J Cardiothorac Surg(2006) 29: 562– 566 Johansson J, Lindberg CG, Johnsson F et al. Active or passive chest drainage after oesophagectomy in 101 patients: a prospective randomized study. Br J Surg(1998) 85: 1143– 1146 Mistry RC, Vijayabhaskar R, Karimundackal G et al. Effect of short-term vs prolonged nasogastric decompression on major postesophagectomy complications: a parallel-group, randomized trial. Arch Surg(2012) 147: 747– 751 Wunsch H, Gershengorn HB, Cooke CR et al. Use of intensive care services for medicare beneficiaries undergoing major surgical procedures. Anesthesiology(2016) 124: 899– 907 Flisberg P, Tornebrandt K, Walther B et al. Pain relief after esophagectomy: thoracic epidural analgesia is better than parenteral opioids. J Cardiothorac Vasc Anesth(2001) 15: 282– 287 Davies RG, Myles PS, Graham JM. A comparison of the analgesic efficacy and side-effects of paravertebral vs epidural blockade for thoracotomy: a systematic review and meta-analysis of randomized trials. Br J Anaesth(2006) 96: 418– 426 Weijs TJ, Berkelmans GH, Nieuwenhuijzen GA et al. Routes for early enteral nutrition after esophagectomy: a systematic review. Clin Nutr(2015) 34: 1– 6 Hessami MA, Najafi F, Hatami S. Volume threshold for chest tube removal: a randomized controlled trial. J Inj Violence Res(2009) 1: 33– 36
Thank you
Why ERAS? • Promote earlier return to normal physiology 1, 2 • • • Lower complication rates Lower readmission rates Improve length of stay Lower overall cost Patient satisfaction 1. Fearon KC, Ljungqvist O, Von MM et al (2005) Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 24: 466– 477 2. Ljungqvist O, Scott M, Fearon KC (2017) Enhanced recovery after surgery: a review. JAMA Surg 152: 292– 298
Nutrition
Challenges in research • • CA esophagus/OGJ tumour is not as common as other GI malignancies. Varies surgical approaches depending on the patient/tumour/experitise availabilities (transhiatal/thoracoabdominal/VATS, two phases vs 3 phases, extended vs standard LN dissections) • • High quality RCT in single center is difficult Accurate controlling between different centers is difficult Despite all these, comparison of programs with historical controls is the first step to open up the opportunity for research
Our Experience • Initiated ERAS in esophagectomy since 2017 • 43 patients underwent MIE between 2015 and 2018 • • 24 patients were in the ERAS group from 2017 -2018 19 patients in the non-ERAS group from 2015 -2016 • Baseline characteristics were similar • No statistically significant difference in operative time, blood loss, transfusion rate and conversion rate • Significantly shorter hospital stay, earlier resumption of diet • No statistically significant difference in complication rate
Our Experience • • Median hospital stay was significantly shorter in ERAS group (10 days versus 23 days, p=0. 001) Time to resume diet is significantly earlier in ERAS group • clear fluid diet (3 day versus 8. 5 days, p=0. 05) • fluid diet (4 days versus 9 days, p=0. 004) • puree diet (5 days versus 10. 5 days, p=0. 004) Significant less usage of parental nutrition in ERAS group (0 day versus 9 days, p<0. 05) No significant difference of morbidity and post-operative complications between two groups (p=0. 631)
Preoperative management Intraoperative management Postoperative management Multi-disciplinary approach including Enhanced recovery anaesthetic surgeon, clinical oncologist, technique and fluid management diagnostic radiologist, case nurse, dietitian, physiotherapist DVT prophylaxis Extubated in OT if possible Restricted fluid management DVT prophylaxis Postoperative Chest physio Preoperative nutritional support. NGT feeding in patient with obstructive tumour If uneventful conduit + reconstruction/normal vocal cord status D 1 clear fluid +NJT feeding D 2 fluid diet+ increasing NJT feeding D 3 soft diet+/- off NJT if tolerated *Contrast study is not mandatory Preoperative Hb level optimizationuse of iv iron Preoperative chest physiotherapy VAT MIE, Laparoscopic gastric mobilization, intrathoracic/neck anastomosis as the standard approach *Intraoperative RLN monitoring *Intraoperative ICG for conduit blood supply Preoperative carbohydrate loading No routine neck/abdominal drains placement Adequate patient counselling Only one soft pliable chest drain on the right side with one-way valve to suction drain Same Day Admission Early removal of foley Early removal of pleural drainage if output <200 cc/day and no chyle leakage Early mobilization
traditional ERAS Patients 19 24 Operative time (min) 452 451 P=0. 625 Blood loss (ml) 150 120 P=0. 587 Median hospital stay (day) 23 10 p=0. 001 Use of abdominal drain 14 3 p<0. 05 Use of left side chest drain 19 8 p<0. 05 Clear fluid diet 8. 5 3 p=0. 05 4 p=0. 004 5 p=0. 004 Time to resume diet (day) Fluid diet 9 Puree diet 10. 5 Parental nutrition (day) 9 0 p<0. 05 Complication (Clavien-Dindo grade) 18 24 P= 0. 631 Grade I- II 12 18 Grade III- IV 6 6