Enfermedad de la Glucoquinasa De la investigacin bsica

“Enfermedad de la Glucoquinasa. De la investigación básica a la Clínica” Profesor. Antonio Luis Cuesta Muñoz Danish Diabetes Academy. Faculty of Health and Medical Sciences. Universidad de Copenhagen, Dinamarca 24 de abril 11: 30 h AULA B 2 FACULTAD DE CIENCIAS UMA

Seminario Facultad de Medicina Universidad de Málaga Abril 2017 “Enfermedad de la Glucoquinasa, de la Investigación Básica a la Clínica y Viceversa” Antonio L. Cuesta Muñoz MD, Ph. D. Danish Diabetes Academy International Institute of Genetics of Diabetes (INIGEDIA) University of Copenhagen Faculty of Health and Medical Sciences Department of Biomedical Sciences Panum Institute

D. M. tipo 1 D. M. tipo 2 D. Monogénicas Inmunológica Genético - ambiental Mutación genética Ausencia Insulínica Resistencia Insulínica Disminución Secreción Insulina

Diabetes Monogénica • • • Autosómica dominante. Comienzo temprano. Autoinmunidad pancreática negativa. Alta penetrancia. Correlación genotipo-fenotipo facilmente identificable en una misma familia. Comienzo con hiperglucemia leve y asintomático en jóvenes (adultos) no obesos. No cetósica. Evolución variable. Defecto primario: Alteración en la función de la célula . Alterada secreción de insulina en respuesta a la glucosa. 5 -8%

GK
 600 500 Control 400 Glucokinase HNF-1 300 200 HNF-4 100 0 3")
ISR (pmol/min) 600 500 Control 400 Glucokinase HNF-1 300 200 HNF-4 100 0 3 6 9 12 Glucose (m. M) 15
.")
Understanding Glucokinase • Encoded by the GCK gene on chromosome 7. • GK (HK-IV). Glucose is the only relevant physiological substrate. • 50 -KD, Three isoforms; GK-I, GK-L 1 y GK-L 2. • It is not regulated by metabolites ( glucose-6 -P) or cofactors (Pi) of glucose metabolism. • Low affinity for glucose (6 -10 m. M) • Cooperative behaviour for glucose, but not for its second substrate Mg. ATP 2 -.
 Glucokinase WT Glucose (m. M)")
Rate ( mol/min/mg protein) Glucokinase WT Glucose (m. M)

Where is GK located and what it does. • Islet cells producing insulin ( -cell) • Islet cells producing glucagon ( -cell) • Islet cells producing somatostatin (delta-cell) • Hypothalamus • Enterocytes • Hepatocytes Glucose Sensor • “Switch on” the Glycogen Synthase in hepatocytes.
 by pancreatic β-cell. Glucose Transporter Acetylcholine GLP-1")
Glucokinase governs Glucose Stimulated Insulin Secretion (GSIS) by pancreatic β-cell. Glucose Transporter Acetylcholine GLP-1 M 3 Glucose Glucokinase G-6 -P Triggering c. AMP PKC PKA Augmentation Glycolysis ATP/ADP Insulin Granules [Ca 2+] K+ATP dependent channel Voltage dependent Ca 2+ Channel Insulin Ca 2+ De ation polariz K+
. 100 Relative blood glucose Phosphorylation")
GK is responsible for the threshold for GSIS (TGSIS). 100 Relative blood glucose Phosphorylation rate (%) 90 80 70 60 50 Maximum Insulin Secr. 40 30 20 Threshold for Insulin Secr. 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 Plasma Glucose (mmol/l) The concept of Glucokinase System.

Translation to Human Inactivating GCK Mutations: Heterozygous >>> GCK - MD. Homozygous >>> GCK – PNMD. Activating GCK Mutations: Heterozygous >>> GCK – Hypoglycaemia Homozygous >>> ? ? ? Glucokinase Disease.

Glucokinase Disease Disorder that involves a functional disruption of GK due to mutations in GCK, which result in both and altered insulin, glucagon and somatostatin secretion by the pancreatic islet and glycogen production by the hepatocytes, affecting the maintenance of euglycemia in humans.
 • Life-long mild or moderate fasting hyperglycaemia,")
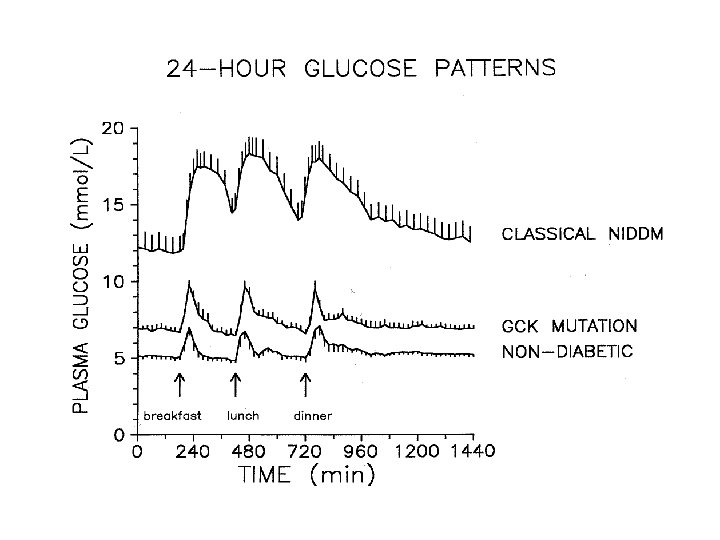
Glucokinase Disease Familial fasting hyperglycemia (MODY 2) • Life-long mild or moderate fasting hyperglycaemia, from birth • Clinical phenotype remarkably constant • Compensation over expression of the normal, non-mutated allele • Rarely symptomatic and (usually detected incidentally) • Glucose remains regulated at a higher level re-setting • Fasting glucose >5. 5 mol/l 2 hour value <4. 5 mmol/l
. 100 Relative blood glucose Phosphorylation")
GK is responsible for the threshold for GSIS (TGSIS). 100 Relative blood glucose Phosphorylation rate (%) 90 80 70 60 50 Maximum Insulin Secr. 40 30 20 Threshold for Insulin Secr. 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 Plasma Glucose (mmol/l) The concept of Glucokinase System.

GCK-Hypoglycemia • Activating GCK mutations. • Clinically Heterogeneous, from mild to severe hypoglycemia. • “Transitory” forms will relapse. • Normal lipid profile. • High frequency of “de novo” mutations.
. 100 Relative blood glucose Phosphorylation")
GK is responsible for the threshold for GSIS (TGSIS). 100 Relative blood glucose Phosphorylation rate (%) 90 80 70 60 50 Maximum Insulin Secr. 40 30 20 Threshold for Insulin Secr. 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 Plasma Glucose (mmol/l) The concept of Glucokinase System.

TGSIS S 64 F Y 214 C V 91 L 454 Ainsert A 456 V S 64 Y G 68 V 6 70 5 60 4 50 40 3 30 2 20 10 0 0 Relative Activity Index (RAI) (unitless) 1 T 65 I W 99 R V 455 M WT GSIS-Threshold (GSIS-T) (mmol/l) Clinically Heterogeneous RAI Bautista et al. NEJM Submitted 2013

61% of activating GCK mutations are “de novo” GCK-T 65 I GCK-S 64 Y GCK-G 68 V GCK-V 91 L GCK-W 99 R GCK-W 99 L GCK-M 197 I GCK-Y 214 C GCK-E 442 K GCK-V 452 L GCK-ins 454 A GCK-V 455 M GCK-A 456 V Paternity test reported

GCK-hypoglycemia is pathophysiologically different to K ATP-HI. KATP-HI “Impossibility” to suppress insulin secretion during hypoglycemia as this secretion becomes independent from βcell glucose metabolism and consequently completely “unregulated”. GCK-Hypoglycemia Insulin secretion depends entirely on β-cell glucose metabolism but with a “resetting” of its TGSIS at values lower than physiological (5 mmol/l) >>> “delay”, rather than incapacity, in the suppression of insulin secretion “regulated” insulin secretion.

In humans with GCK-Hypoglycemia insulin secretion is regulated GCK-V 452 L Meissner et al. Horm Metab Res 2008; 40: 1 – 7

In humans with GCK-Hypoglycemia insulin secretion is regulated GCK-W 99 L C-peptide = 0. 16 nmol/L (0. 26 -1. 32 nmol/L) Samir et al. Diabetes P. Ahead 2009

Islet

Finnish baby girl born in 1972 Severe Neonatal Hypoglycemia Sub-total pancreatectomy at 6 m. o. a “De novo” Activating GCK mutation (GCK-Y 214 C) Histology report >>> Normal Islets. African-Caribean baby girl born in 1997 Severe Neonatal Hypoglycemia Subtotal pancreatectomy at 3 y. o. a Activating GCK mutation (GCK-V 91 L) Histology report >>> Normal Islets. French baby boy of Tunisian origin born in 2009 Severe Neonatal Hypoglycemia Subtotal pancreatectomy at 2 and 4 m. o. a “De novo” Activating GCK mutation (GCK-S 64 F) Histology report >>> Normal Islets.

GK – Y 214 C Jacques Rahier Age Matched Controls 120 m 50 m GK – V 91 L Sameer Kassem Jacques Rahier GK – S 64 F V. Verkarre D. Bautista Jacques Rahier

GCK-hypoglycemia is histopathologically different to K ATP-HI. GK – V 91 L 120 mm focal hyperinsulinism KATPHI diffuse hyperinsulinism KATPHI Cuesta-Muñoz et al. Diabetes 53: 2164; 2004

GCK-V 91 L CTRL EGFP β-cell proliferation
 Age Matched Controls GK – V 91 L")
GCK-hypoglycemia and -cell Proliferation (Ki 67) Age Matched Controls GK – V 91 L Sameer Kassem Jacques Rahier GK – S 64 F D. Bautista Jacques Rahier

GCK-V 91 L CTRL EGFP β-cell apoptosis

GCK-hypo: -cell apoptosis TUNEL Staining 10 m GK – V 91 L 10 m Age-matched control S. Kassem et NEJM; 2010

α-cells

GK is expressed in pancreatic α-cells. Anti-GFP Anti-glucagon. Overlay, co-localization.
")
GCK-hypoglycemia and -cell Proliferation (Ki 67)

δ-cells

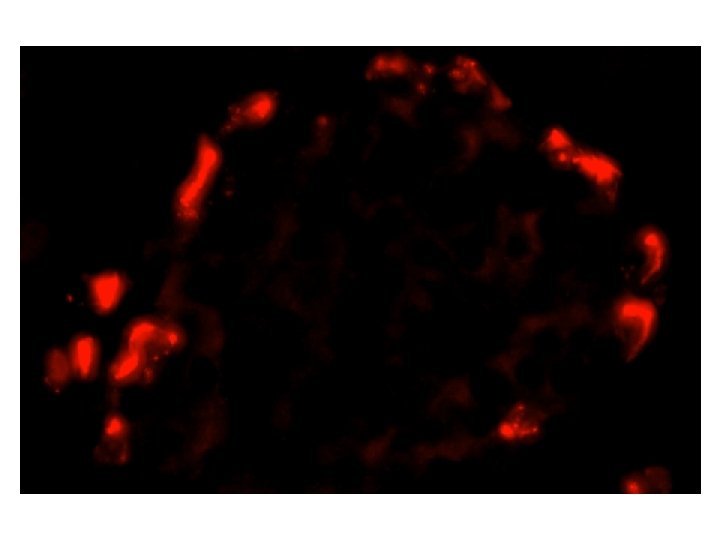
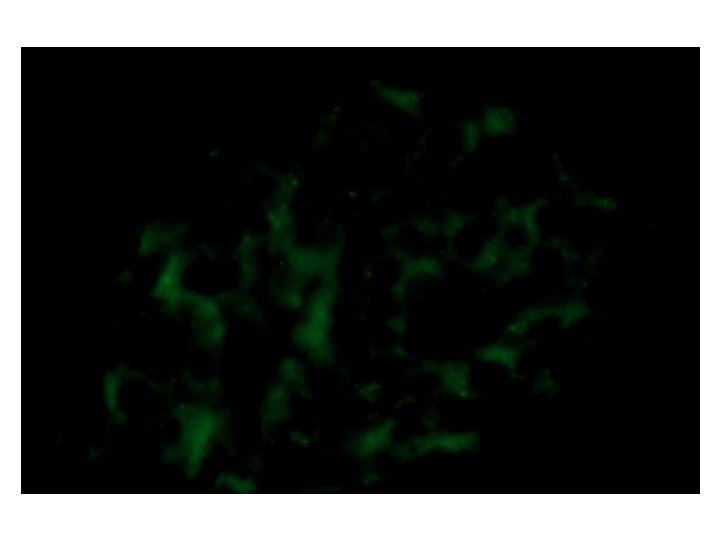
GK is expressed in human pancreatic δ-cells GK Somatostatin 3 x zoom Somatostatin Co-localization 3 x zoom GK 3 x zoom Co-localization
")
GCK-hypoglycemia and -cell Proliferation (Ki 67)

Bi-hormonal cells and an activating glucokinase gene mutation.

Insulin and glucagon coexpression in patient´s islets with GCK-Hypoglycemia. C C B A Figure 1: Presence of bihormonal cells (insulin+ / glucagon+) in human islets from the patient with GCK-Hypoglycemia NAGCK-S 64 F (confocal microscopy).

Double Immunofluorescence for Insulin and Somatostatin INSULIN: GREEN SOMATOSTATIN: RED COMBINED FILTERS
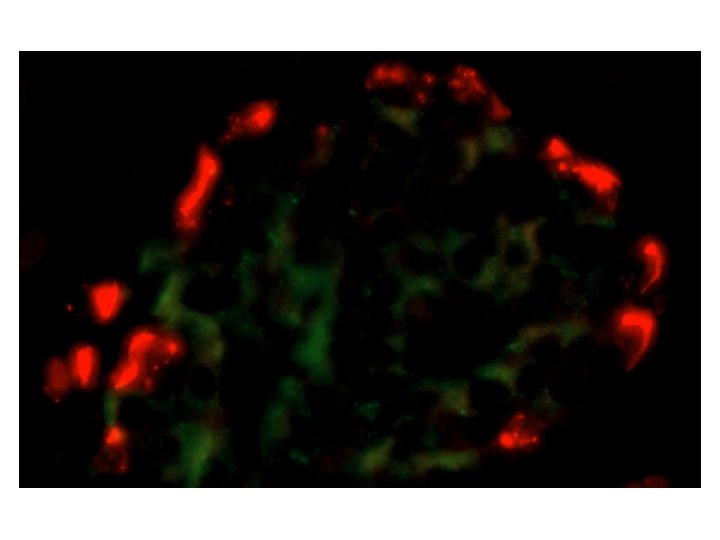
 in human")
A B C Figure 2: Presence of bihormonal cells (insulin+ / somatostatin+) in human islets from the patient with GCK-Hypoglycemia NAGCK-S 64 F (Double Inmunofluorescence Staining).

Double Immunofluorescence for Glucagon and Somatostatin
- Slides: 46