Energy to Skeletal Muscles Lecture2 Creatine Metabolism Objectives

Energy to Skeletal Muscles Lecture-2 Creatine Metabolism

Objectives • To study the importance of creatine in muscle as a storage form of energy • To understand the biosynthesis of creatine • To study the process of creatine degradation and formation of creatinine as an end product • To understand the clinical importance of creatinine as a sensitive indicator of kidney function • To study different types of creatine kinase (CK) and their clinical importance

Production of ATP: • Contraction requires huge amounts of ATP • Muscle fibers produce ATP three ways: • Phosphagens • Aerobic metabolism • Anaerobic metabolism

Overview • Phosphagen is an energy-rich phosphate compound. • Breakdown of a phosphagen such as creatine phosphate enables ATP (adenosine triphosphate) to be generated very quickly without oxygen. • ATP is the only chemical energy which can be used directly by contracting muscles.
 Site of")
Creatine Biosynthesis Three amino acids are required: Glycine Arginine Methionine (as S-adenosylmethionine) Site of biosynthesis: Step 1: Kidneys Step 2: Liver

Creatine Biosynthesis Arginine Kidneys + Glycine Amidinotransferase Ornithine Guanidinoacetate Liver SAM Methyltransferase SAH Creatine

Distribution of body creatine • From liver, transported to other tissues • 98% of creatine are present in skeletal & heart muscles • In muscles, creatine is converted to the high energy source creatine phosphate (phosphocreatine) Creatine ATP Creatine Kinase ADP Creatine phosphate

Creatine phosphate • Creatine phosphate is a high-energy phosphate compound • Acts as a storage form of energy in the muscle • Provides a small but, ready source of energy during first few minutes of intense muscular contraction • The amount of creatine phosphate in the body is proportional to the muscle mass Creatine Phosphate ADP ATP Creatine ENERGY FOR MUSCLES DURING EXERCISE (first few minutes)

Creatine degradation 1. Creatine and creatine phosphate spontaneously form creatinine as an end product 2. Creatinine is excreted in the urine 3. Serum creatinine is a sensitive indicator of kidney disease (Kidney function test). Serum creatinine increases with the impairment of kidney function

Creatine Degradation CREATINE DEGRADATION IN MUSCLES

Creatinine in urine and plasma • Normal serum creatinine is 0. 7 to 1. 4 mg/dl (55 -120µmol/L) and serum creatine level is 0. 2 to 0. 4 mg/dl • Serum creatinine is a sensitive indicator of kidney disease (Kidney function test) because creatinine is normally rapidly removed from the blood and excreted • Urinary creatinine can be used to estimate muscle mass As the amount of creatinine excreted in urine is proportional to the total amount of creatine phosphate of the body & the amount of creatine phosphate in the body is proportional to the muscle mass. A typical male excretes about 15 mmol of creatinine per day A decrease in muscle mass due to muscular dystrophy or paralysis leads to decreased amount of creatinine in urine • The amount of creatinine in urine is used as an indicator for the proper collection of 24 hours urine sample (normal urinary output is 15 -25 mg/kg/day )

Plasma creatinine & kidney functions Creatinine is an end product of nitrogen metabolism and is excreted in urine. Plasma creatinine & creatinine clearance are used to assess the kidney functions (Kidney function tests in labs). Plasma creatinine: 1 - more precise than creatinine clearance which depends on urine volume for its calculation 2 - is fairly constant through out adult life while creatinine clearance declines with aging. .
 • Creatine Kinase is responsible for the generation of creatine")
Plasma Creatine Kinase (CK) • Creatine Kinase is responsible for the generation of creatine phosphate in contractile muscular tissues • CK levels are changed in disorders of cardiac and skeletal muscle Creatine ATP Creatine. Kinase ADP Creatine phosphate
 1. CK is required for conversion of creatine into creatine")
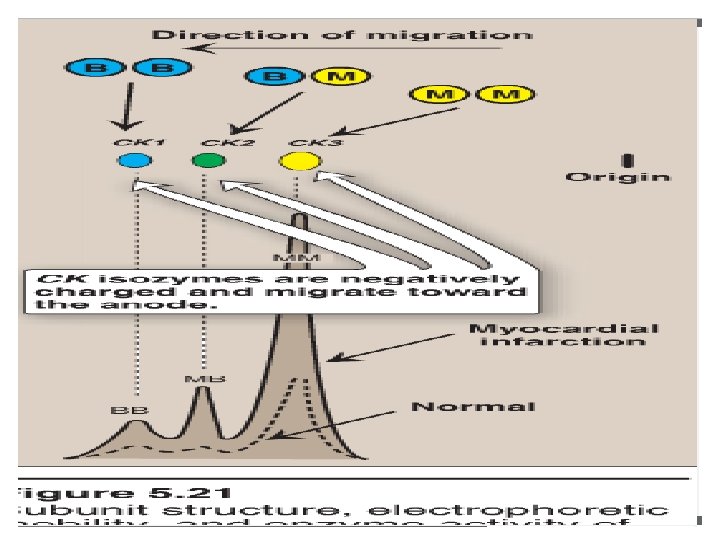
Plasma Creatine Kinase (CK) 1. CK is required for conversion of creatine into creatine phosphate 2. It is formed of two subunits (B & M) 3. CK has 3 isoenzymes: Skeletal muscle: > 98% CK-MM & 2 % CK-MB Heart muscle: 70% CK- MM& 20 & 30%CK-MB Brain : CK-BB These isoenzymes can be separated according to their physical properties using electrophoresis

Creatine Kinase & muscle diseases • There are many enzymes as CK, AST, LD & ALT may be increased in muscle diseases. • Plasma total CK is usually the measurement of choice (largest changes and the greatest number of cases of different etiologies) • Plasma CK is valuable in the diagnosis of myocardial infarction and some muscle diseases • Increase in plasma CK may occur after trauma or surgical operation, intramuscular injections , after prolonged muscular exercise.

Creatine Kinase & muscle diseases • In Duchenne muscular dystrophy: • Increase in total plasma CK at birth before onset of clinical signs • Plasma total CK is increased during early stages of the disease & tend to fall at the terminal stage • About 75% of female carriers of Duchenne dystrophy have small increases in plasma CK • In neurogenic muscle disease: plasma CK is usually normal in peripheral neuritis, polymyelitis

References • Lippincott, Illustrated Biochemistry • Bishop : Clinical Chemistry Principles, Procedures Correlation 6 th edition • Lecture Notes in Clinical Biochemistry
- Slides: 18