Endovascular Stenting for Superior Vena Cava Occlusion Secondary


 syndrome commonly results from malignant obstruction caused by direct")



. Additionally,")











- Slides: 19
Endovascular Stenting for Superior Vena Cava Occlusion Secondary to Postradiation Fibrosis Mohammad Thawabi, MD, FACC Interventional cardiologist Huntsville Heart Center, Huntsville, AL Mohammad. thawabi@outlook. com
Disclosures Nothing to disclose
Introduction Superior vena cava (SVC) syndrome commonly results from malignant obstruction caused by direct invasion or external compression of the SVC by a pathological process. Rarely, SVC obstruction can occur due to postradiation vascular fibrosis in patients who received prior thoracic radiation therapy predating their symptoms by several years. We present a case of SVC obstruction diagnosed 18 years after chest radiation and treated with an endovascular approach.
History and PE • A 47 -year-old male was referred for evaluation of exertional chest pain. • The pain was described as heaviness that occurs during exercise and severely limits his active lifestyle. He has been coping with his symptoms for the past 15 years, during which he underwent multiple non-diagnostic cardiac evaluations. • Additionally, he noted head fullness exacerbated by bending forward, recurrent headaches and nasal congestion, and distended veins over his lower chest and upper extremities swelling when he exercises.
History and PE • Past medical history: significant for a history of Hodgkin lymphoma treated successfully with chest radiotherapy 18 years ago with no evidence of recurrence by surveillance PET scans. • Physical examination: mild neck veins distention.
Workup • Given history and the timing of his symptoms, starting three years post chest radiation, postradiation fibrosis of the SVC was suspected. • A gated chest CTA was performed to evaluate for SVC obstruction and rule out mediastinal masses and coronary disease
• SVC occlusion was seen with extensive collateral circulation (Images A, B). Additionally, extensive pericardial varices were seen (Image C).
Treatment options • Endovascular attempt with possible stenting. • Surgical bypass using prosthesis or autologous vein graft. • Conservative management.
Venography and intervention planning • • Access: US guided right CFV with Pre. CLose and right basilic vein. Simultaneous venography from the right atrium and right brachiocephalic. Destination sheath from the CFV. Antegrade vs retrograde crossing depending on the cap characteristics. IVUS after crossing to rule out thrombotic burden and assess in sizing. Venous stent and bailout covered stent (Viabahn VBX 11 mm expanding to 16 mm). CTS on standby.
• 5 -Fr Pigtail catheter was advanced from the basilic vein. • 5 -F MP 2 catheter was advanced from the CFV into the proximal SVC. • Favorable cap was noted proximally.
• After using multiple wires and microcatheters, 0. 018” system could cross the occlusion (Glideadvantage and Rubicon microcatheter). • Most wiring attempts were initially unsuccessful due to the abundant collaterals.
Only 3. 0 mm PTA balloon could cross the stenosis and required high pressure inflation. Sequential PTA with 5. 0 mm balloon
• Initial angiography after 5. 0 mm PTA to rule out immediate complications. • No complications were noted.
After IVUS. High pressure angioplasty with 10. 0 mm PTA balloon was required to overcome the severe fibrotic nature of stenosis.
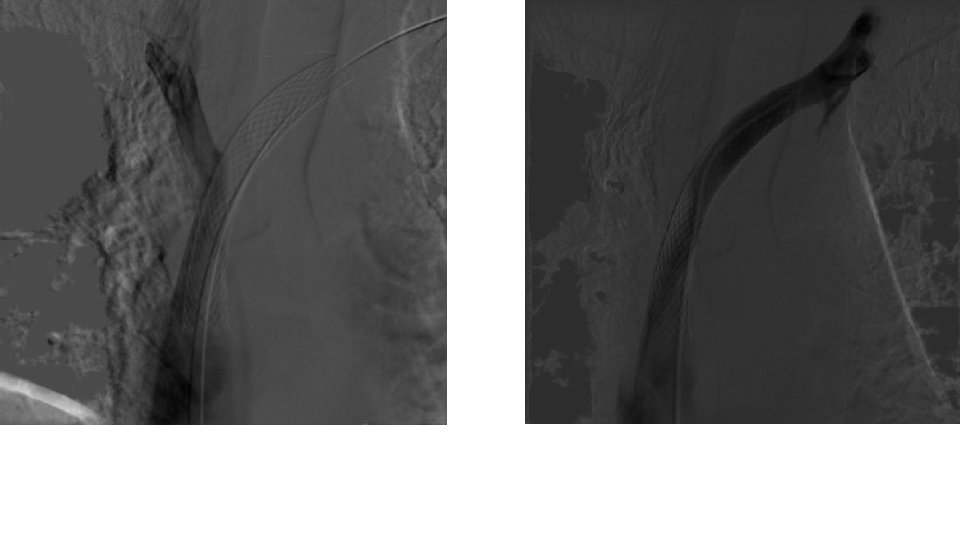
16 x 60 WALLSTENT was deployed and postdilated with a 16 mm PTA balloon
• The patient was start on clopidogrel and rivaroxaban. • On follow up, the patient has resolution of his symptoms, with significant improvement in his exercise tolerance. • Maintained on rivaroxaban.
Discussion • Postradiation fibrosis, with subsequent SVC obstruction, can occur in cancer survivors and present several years post chest radiation therapy. • Endovascular therapy is a feasible therapeutic option with excellent results.
Questions Mohammad. thawabi@outlook. com