Endovascular Live Case Mount Sinai Hospital NY 012418


 • ABI: Right – 0.")























- Slides: 32
Endovascular Live Case Mount Sinai Hospital, NY 01/24/18
History • 81 year old, male • Type 2 DM, hypertension, dyslipidemia, CAD, PAD, CKD • Claudication x 3 months (<1/2 block, left>right). Rutherford category 3
Exam, Labs, Medications • left DP and PT (doppler) • ABI: Right – 0. 89, Left- 0. 77 • • Hb- 13. 1 g% Platelets- 183 k INR- 1. 0 Creatinine- 1. 4 • Medications: Aspirin, Plavix, Simvastatin, Cilostazol
Inflow
Left leg run off
DSA – CFA bifurcation
Strategy • Right groin access • 7 F, 45 cm cross over Terumo destination sheath • Cross with spartacore wire • Embosheild NAV 6 filter • Directional atherectomy • Drug coated balloon angioplasty • Bail out stenting for flow limiting dissection, perforation
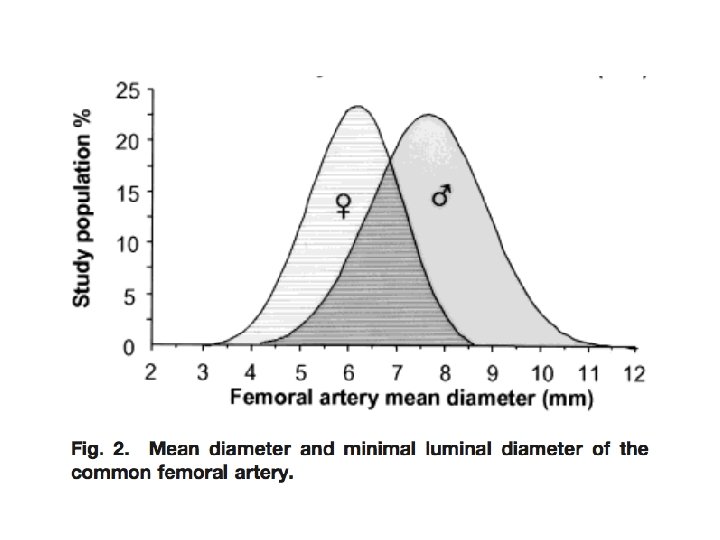
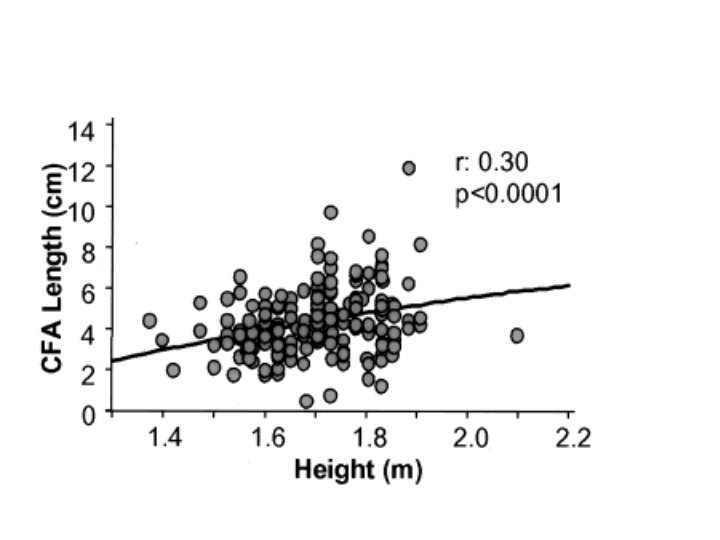
CFA anatomy Diameter Length Bifurcation anatomy
CFA bifurcation variants
TASC II classification
SCAI 2014 guidelines
2016 AHA/ACC PAD guidelines
CFA endarterectomy
CFA endarterectomy
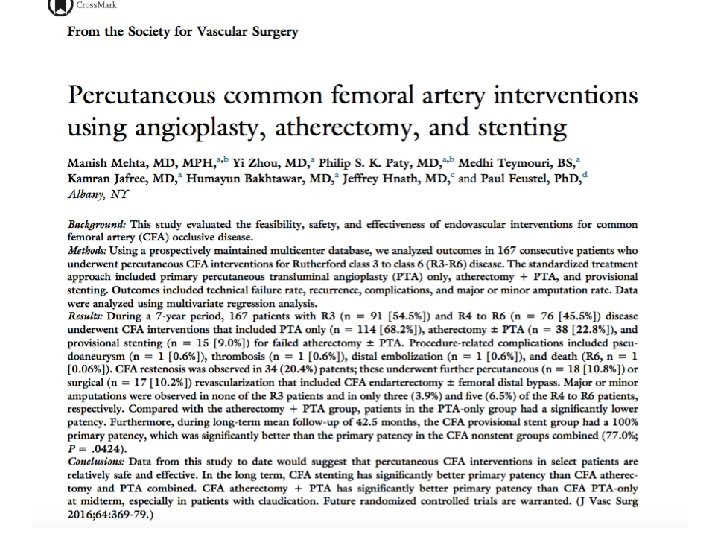
Endovascular treatment of atherosclerotic CFA disease
Patient characteristics
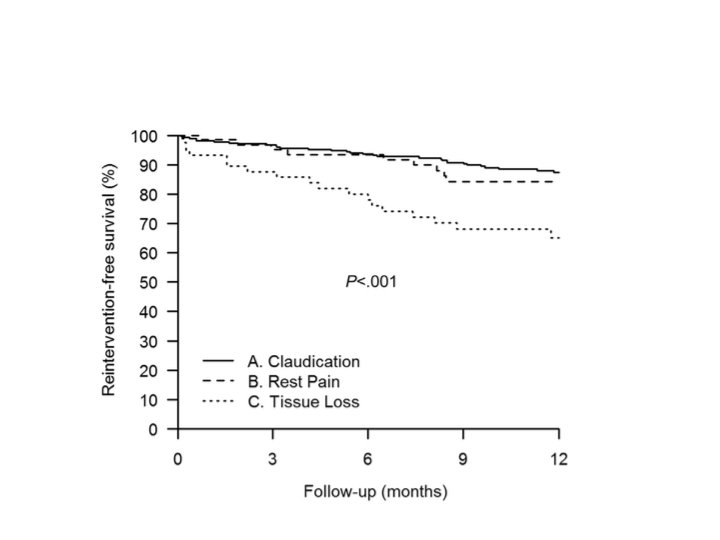
Kaplan-Meir TLR free proportion
Stented vs non stented
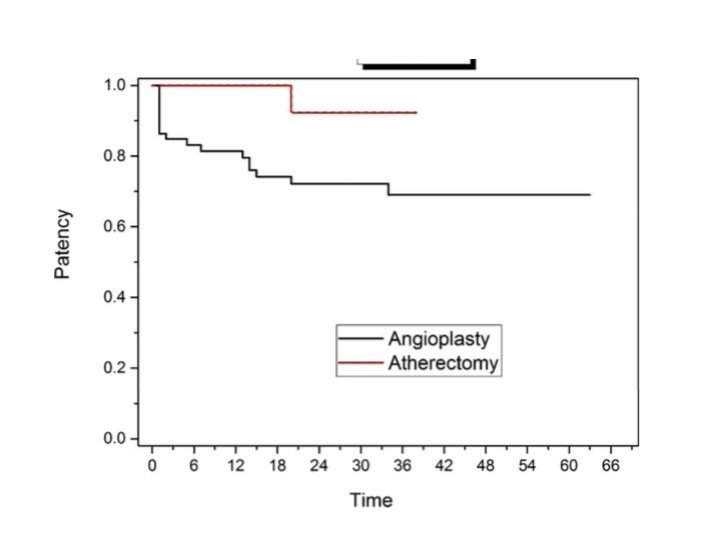
Atherectomy vs PTA
CFA –nitinol stents
CFA- nitinol stents
CFA covered stents
CFA-covered stent
Summary • Endarterectomy should be considered as the first line treatment of CFA disease • Endovascular Rx provides a viable option in non-surgical cases • Atherectomy> PTA • Drug coated balloon • Stent- bailout • Covered stent- emergencies
CFA-CFV
CFA-CFV overlap