Endotracheal Intubation of Dogs and Cats Anesthetist This
 • This set of notes is for")
Endotracheal Intubation of Dogs and Cats (Anesthetist) • This set of notes is for practical use in the surgery suite at VTI • There are no gold stars because this whole power point is a • There is a second set of notes that are more detailed and comprehensive regarding the process and importance of intubation, the risks associated with it, and items we do not have at VTI (VTNE information) • Reading assignment: A&A pages 97 -99 covers the equipment needed & pages 245 -251 covers the process • During lab, be sure to familiarize yourself with where to find intubation supplies and where to clean them
 patient, used")
Endotracheal Intubation • Flexible tube, placed inside trachea of an anesthetized (induced/unconscious) patient, used to transfer gases directly from the anesthesia machine to the patient’s lungs, therefore securing the airway. • Please know the definition of/be able to locate the following: • • Larynx Trachea Arytenoids Epiglottis Soft palate Tracheal bifurcation Bronchus Alveoli 2
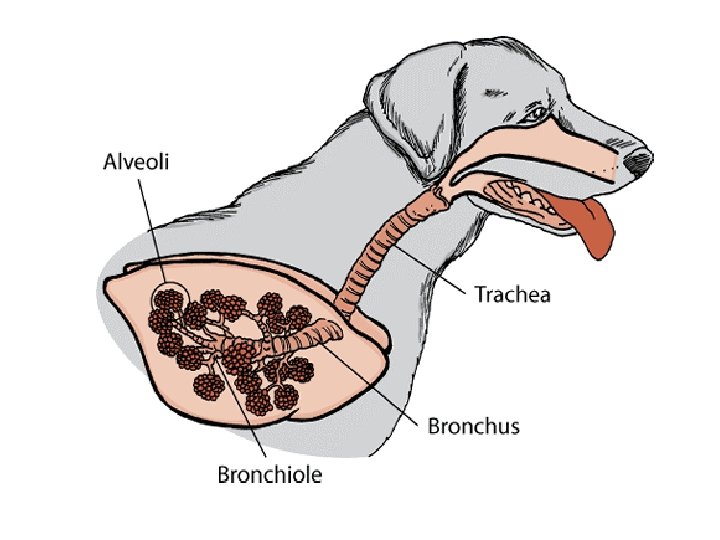

Anatomy Review

Supplies: Laryngoscope • Identify all parts • Ensure light is functioning properly • Curved vs. straight

Supplies: Secure Tube in Place • You have options: o Roll gauze o IV line tubing *usually best option • You will tie it around the tube first, and then around the patient’s head • Tie should be placed as far back as possible, without occluding the inflation line • Use a bow tie, not a knot

Supplies: Stylet • Stylet is placed inside of the ET tube o Made of strong wire/metal • What is the purpose? • Stylet should be longer than ET tube o Why? *Usually only used for cats

The Endotracheal Tube • ET tubes are made of polyvinyl chloride • View silicone demo tube • They have a Murphey eye and a cuff • You will prepare the size you think will be appropriate & 1 tube smaller and 1 tube larger

Selecting an Appropriate ET Tube DIAMETER • Measured in ________ • Should be a snug, but smooth fit • Should not “fall” in OR be forced into trachea “Largest that will comfortably accommodate patient” DOGS = based on weight (table in A&A book) Remember: 20 kg = 9. 5 -10 mm

Selecting an Appropriate ET Tube LENGTH • Should extend from the _________ to cranial to the _______________. • Can use shoulder as a landmark

Preparation is Key The night before surgery: • Check several tubes for loose connectors, excessive wear, cuff leaks, debris, etc. • Perform a cuff leak check: Immediately before intubating: • Apply lubrication to cuff • Water or sterile lube depending on tube size • Very small amount and this is optional • Check patient ______ tone and _____ reflex

Intubation Techniques 1. Visual Procedure 8 -6 on Page 260 • Direct visualization of larynx minimizes possibility of traumatic or improper intubation • RESTRAINT/positioning IS KEY!

Visual Technique: Restrainer • Restrainer holds hand placed on the muzzle with fingers behind front canine teeth (like you would for pilling) pulling upward to open the mouth • Neck should be straight in line with body and fully extended • Adjust to the wishes of the person intubating 13

Visual Technique: Intubation During intubation: • Hold laryngoscope in hand • Hold ET tube in other hand • Gently pull tongue forward, and press the blade to the base of tongue to expose trachea • Try to avoid touching the epiglottis • Soft palate may be obstructing your view • Blade too far forward can obstruct your view
 • Epiglottis")
• Visualize tracheal opening (confirm by presence of arytenoids and epiglottis) • Epiglottis closed? *May need to use blade to push down on tongue or push up on soft palate • Once epiglottis lies flat/open, slide ET tube past it and down into the trachea o Aiming caudally may cause esophageal intubation • Once it’s in to desired depth, confirm presence in trachea • Secure into place

How Do You Know You’re In? • Condensation seen in ET tube with each breath • Feel air through tube with each breath • Palpate throat for one firm structure • Patient can not vocalize

How Do You Know You’re In? Using Machines: • Provide PPV= chest should rise (stomach should NOT) • Auscultate BOTH lung fields • Parts of Ax machine should move with respirations o Which parts? • Capnometer should give appropriate readings

Cuff Inflation- Patient Leak Test Cuff is attached to a pilot balloon with a spring loaded inflation valve • Must depress the spring in order to inflate! 1. Manually ventilate and listen for air escaping around the tube • If you hear air escaping (most likely will), inflate cuff slowly until you don’t • Balloon should not feel taught or be fully inflated • Once no air sounds are heard, you’re good! • You will also feel resistance while squeezing the reservoir bag if the cuff is inflated appropriately *Inflating the cuff fully should not take the place of using a larger tube!

After Intubation • Move the patient into desired position for the procedure • Hook up anesthesia machine to patient • Set flow meter first • Set vaporizer (if needed) once hoses are in place • MUST DISCONNECT PATIENT from breathing hoses anytime the patient is repositioned *Never let breathing hoses hang off of the table • Most important with small ET tubes *Do not move the endotracheal tube without deflating the cuff first!

Recovery Period • You’re ready to wake them up! • Patient will remain on oxygen for about 5 minutes • Recumbency: ____________ • Head and neck ______ • Check oral cavity • Watch for signs of waking up:

Recovery Period- Extubation 1. After 5 minutes, oxygen can usually be discontinued 2. Disconnect breathing hoses and then untie ET tube tie 3. Deflate cuff completely and remove ET tube only when: DOGS: Once swallowing reflex has returned CATS: Earliest sign of regaining consciousness (any voluntary movement- whiskers, head, tail flick, brisk palpebral) 4. Prevent obstruction of airway with tongue by pulling tongue forward during AND after removing the tube 5. Patient should react to removal of ET tube • Swallowing, licking/moving tongue, raising head, extending legs

ET Tube Cleaning • Inflate cuff and leave inflated until dry • Wash inside AND outside of endotracheal tube • Use bottle brushes and pipe cleaners to remove all debris • Use warm soapy water to get mucus off • Rinse • Disinfect in DILUTE chlorhexidine solution • Rinse VERY well • Hang upright to dry over night • Deflate cuff and replace in correct location
- Slides: 22