Endotracheal Intubation of Dogs and Cats Anesthetist AA
 A&A Pages 97 -99 & 245 -251")
Endotracheal Intubation of Dogs and Cats (Anesthetist) A&A Pages 97 -99 & 245 -251
 patient, used to")
Endotracheal Intubation Flexible tube, placed inside trachea of an anesthetized (induced) patient, used to transfer gases directly from the anesthesia machine to the patient’s lungs, therefore securing the airway. Page 2

Advantages Artificial ventilation can be provided ◦ PPV Reduces the risk of pulmonary aspiration ◦ What is being aspirated? Dead air space reduced increase efficiency of gas exchange with inhalation anesthetics ◦ Anatomic dead space – This is good for two reasons: 1. 2. 3

More advantages Secretions can be removed with suction catheter through the ET tube Drugs can be easily administered in emergency (route = ____) ◦ Dosage =

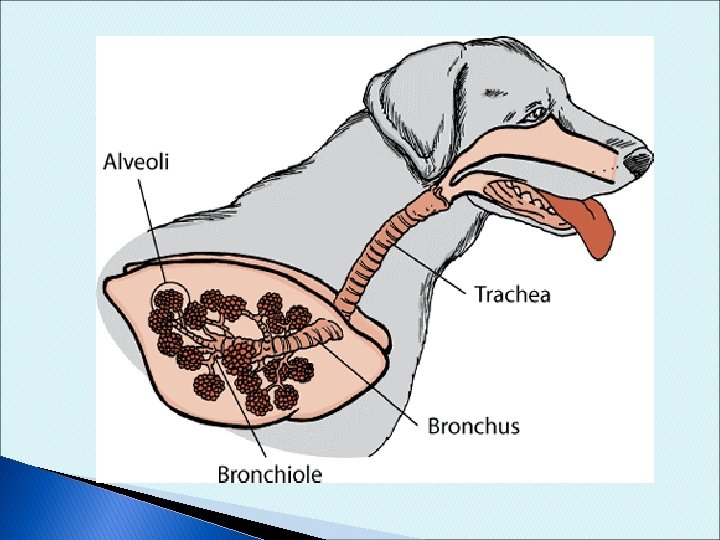
Anatomy Review

Challenges to Intubating Overzealous efforts to intubate can damage anatomy Esophageal intubation Tube can be left too far cranial Tube can be inserted past tracheal bifurcation Pressure ______ from over inflation of cuff

Types of ET Tubes- Materials

Types of ET Tubes- Armored

Types of ET Tubes Murphy tubes ◦ Cuffed or non-cuffed ◦ Murphey eye- distal end of tube Purpose: Magill tubes: ◦ Cuffed or non-cuffed ◦ No Murphey eye

Purpose of Cuff on Tube Efficient positive pressure ventilation Efficient delivery of inhalant anesthetics Prevent foreign material from entering lungs ◦ When is this likely?

Cuff Inflation Cuff is attached to a pilot balloon with a spring loaded inflation valve ◦ Must depress the spring in order to inflate! Cuff should inflate, but not be maximally full of air …how do you know how much? ?

Types of Cuffs High volume, low pressure cuffs *Rule:

Cuff Inflation- Patient Leak Test Manually ventilate and listen for air passing around the tube ◦ If no air sounds are heard, you’re good! ◦ If you hear air escaping, inflate cautiously until you don’t *Inflating the cuff more should not take the place of using a larger tube!

Cuff Inflation • Recheck every 30 min of surgery – especially after moving or repositioning patient • How can you check cuff inflation? • Most important for which type of procedures? ? • If you are running anesthesia for longer than 2 hours, you can reposition the ET tube slightly to ensure pressure necrosis does not happen. IMPORTANT: Must deflate cuff before moving tube! *Even in emergencies*

Types of ET Tubes Cole tubes Laser specific tubes

Laryngoscope Responsible for maintenance: batteries/charging and light bulbs

Videos http: //www. youtube. com/watch? v=3 EDRvv. Gp OZk&NR=1 - intubation of a dog http: //www. youtube. com/watch? v=CGj. GTf. P_ Bs 0 – intubation with cuff

Selecting an ET Tube DIAMETER Measured in ________ Should be a snug, but smooth fit ◦ Should not “fall” in OR be forced into trachea “Largest that will comfortably accommodate patient” CATS = 3. 0 -4. 5 mm DOGS = based on weight (table in A&A book) Remember: 20 kg = 9. 5 -10 mm

Tips for Tube Size Weight based is only a guideline! ◦ Brachycephalics: ◦ Obese patients: Palpation is more accurate; requires more practice Always prep 3 tubes! Can use width of space between the nostrils as a guide

Selecting an ET Tube LENGTH Extend from _________ to cranial to the ____________. If you extend into only one bronchus:

ET Tube Length If tube extends past patient’s nose Increased _______ dead space How might we solve this?

Prior to Intubation Check several tubes for loose connectors, excessive wear, cuff leaks, debris Cuff leak check: Immediately before intubating: Apply lubrication to cuff ◦ Water or sterile lube depending on tube size ◦ Very small amount and is optional Check patient jaw tone ◦ Swallow reflex?

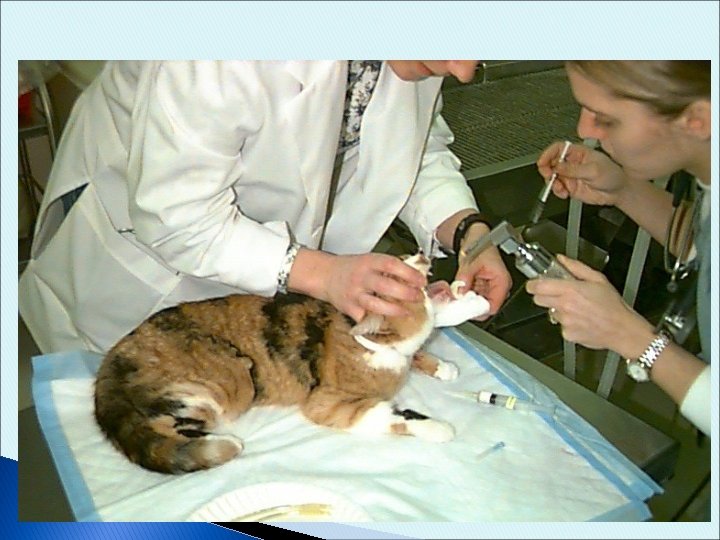
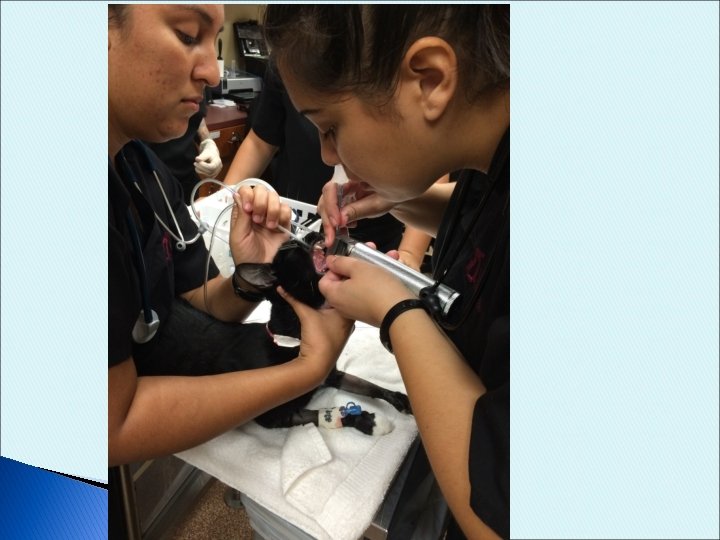
Intubation Techniques 1. Visual Procedure 8 -6 on Page 260 Direct visualization of larynx minimizes possibility of traumatic or improper intubation Position: ◦ Position is preference RESTRAINT IS KEY!

Visual Technique Restrainer holds hand placed on the muzzle with fingers behind front canine teeth (like you would for pilling) pulling upward to open the mouth Neck should be: Pull tongue forward to visualize back of throat ◦ Not too far! 27
 ◦ Epiglottis closed?")
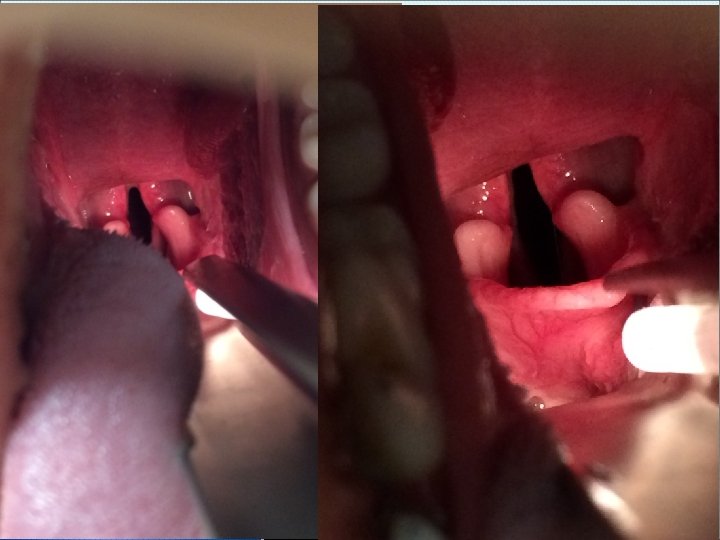
Visualize tracheal opening (confirm by presence of arytenoids and epiglottis) ◦ Epiglottis closed? *May need to use ____________to push down on tongue or push up on soft palate Once epiglottis lies flat/open, slide ET tube past it and down into the trachea Tech note: You may need to wait for inhalation to see the trachea on cats

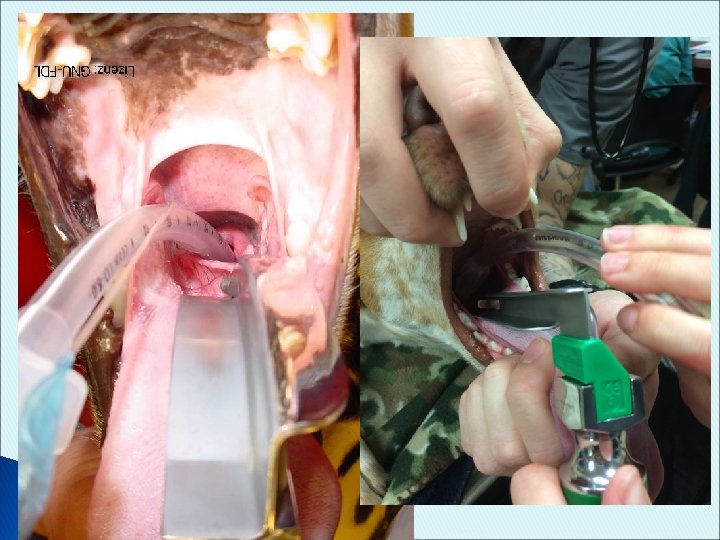
Holding the Laryngoscope Before the procedure: check the light! During intubation: Hold laryngoscope in one hand Hold ET tube in other hand *Note: flange may be obstructing view Press blade against pulled out tongue, exposing trachea ◦ Soft palate may be obstructing your view ◦ Blade too far forward can obstruct your view


With Stylet is placed inside of the ET tube Made of strong wire/metal ◦ Purpose? Stylet should be longer than ET tube! ◦ Why?

2. Blind Intubation Techniques Used in dogs and horses NOT suitable for cats, very small dogs, or patients with edema, swelling or trauma 3. Tactile Cattle, large exotics, a few large dogs Finger holds down the epiglottis Slide tube into trachea using your finger as a guide

Feline Intubation Small oral cavity and sensitive larynx Vocal cords tend to quickly close and push tube to side ◦ Due to swallowing reflex or contact with end of ET tube causes: ___________ ◦ Can be reduced by application of topical anesthetic Apply 0. 1 cc of ________ on glottis *Try to get 0. 05 ml on each arytenoid




How Do You Know You’re In? Condensation seen in ET tube Feel air through tube Palpate throat Normal breathing sounds Patient can not vocalize

How Do You Know You’re In? Using Machines: Give a breath = chest should rise (stomach should NOT) ◦ Listen to BOTH lung sounds Parts of Ax machine should move with respirations Capnometer should give appropriate reading Radiographs?

Page 42

Secure Tube in Place Roll gauze Rubber Band IV line tubing Paper tape-birds/reptiles Things to remember: 1. 2. 3. A L W A Y S disconnect the patient from the anesthetic tubes when moving OR repositioning

Page 44

Maintaining an ET Tube 1. 2. 3. 4. 5. Once you have checked placement and patient is stable, watch for: Kinks or bends ALWAYS disconnect from breathing system when repositioning Watch for weight of breathing system tugging on ET tube Don’t place items on patient’s chest! If you have a “bad lung” keep that one down

Recovery Period You’re ready to wake them up! ◦ Patient will remain on oxygen ◦ Recumbency: ____________ ◦ Head and neck ______ ◦ Check oral cavity ◦ Watch for signs of waking up:

Recovery Period- Extubation Untie the tube: when oxygen is discontinued Deflate cuff completely and remove ET tube: DOGS: Once swallowing has returned CATS: Earliest sign of regaining consciousness (any voluntary movement- whiskers, head, tail, brisk palpebral) *Brachycephalic: head up, chewing on tube before it is pulled! VIDEO

Extubation Process Once cuff is deflated: Slow and steady, down and away Prevent obstruction of airway with tongue by pulling tongue forward during AND after pulling the tube Patient should react: Waiting too long can cause patient to bite tube in half! *Exception to completely deflating cuff:

Post-op Advice to Owner Patients may cough post-op ◦ Should not be severe or continue to get worse ◦ Is noticed if there was a rough intubation Advising owner will avoid phone calls and later explanations!

ET Tube Cleaning Inflate cuff and leave inflated until dry Wash inside AND outside of endotracheal tube Use warm soapy water to get mucus off ◦ Commercial brushes available, cotton swabs, pipe cleaners Rinse Disinfect in DILUTE _________ Rinse VERY well Hang upright to dry over night Deflate cuff and replace in correct location
 Leaky cuff/damage ◦")
Complications Before You Even Start Unclean equipment (we reuse ET tubes!) Leaky cuff/damage ◦ Check before use, during surgery, and while cleaning

Complications While Placing Tube too small ◦ Not getting enough inhalant ax ◦ Like breathing through a straw ◦ Easily become blocked with mucus Tube too large ◦ Damage to anatomy Tube is too long ◦ Hypoxemia and atelectasis/decreased tidal volume

Complications While Placing Over-inflation of cuff: Under inflating cuff = No seal created ◦ Breathing room air ◦ Staff breathing inhalant ◦ Aspiration likely: Vagus nerve stimulation: ◦ Parasympathetic response _________, apnea, cardiac arrhythmias ◦ What class of premed can help prevent this response?
 Not")
Complications During Ax Dislodged tube ◦ ◦ Not tied securely? Coughs out (cats) Not disconnected while repositioning Weight of hoses & machine pulls tube out Restricted air flow ◦ Bevel against wall of trachea What can help prevent this? ◦ Kinks-extreme head position, over edge of table, floppy tube
- Slides: 54