Endoscopy Sedation and Its Role in Bundled Payments

Endoscopy Sedation and Its Role in Bundled Payments Chris Steel MD

Objectives • To understand the basics of endoscopy sedation • To understand the current reimbursement model for endoscopy • To understand a GI nurses’ role in future endoscopy practice models

RED – Southern BLUE - Northern

Perceptions No Glasses • Most Attractive • Most Likeable Glasses • Most Successful • Most Intelligent

Good news • Thin-Rimmed Glasses • Similar attractiveness and likeability of no glasses and more • Similar success and intelligence of thick rimmed glasses

Perceptions Fast paced Speech Cons Pros • Stigma of a “fast-talker” • More intelligent • More socially attractive • More likely to be listened to • More Credible ? – A person who influences or persuades people by talking in a confident and often dishonest way.

Summary of Perceptions Cons Pros • Southern Accent – Less attractive – Less intelligent – Less healthy • Thin rimmed Glasses • Fast-Paced Speech – Less trustworthy (fast talker) – More likeable • Thin-rimmed glasses – More intelligence and success than no glasses – Similar attractiveness and likeability as no glasses • Fast-Pace Speech – – More intelligent More Socially attractive More Credible More likely to be listened to

Planning • Napolean Bonaparte always said he never had a battle that went as he planned, but he never had a battle he didn’t plan for.

Planning • In preparing for battle, I have always found that plans are useless but planning is indispensable. • Everybody has a plan ‘till they get punched in the mouth.

Patient Assessment • History and Physical completed and on the chart. – Specifically review • Airway – Trach (which kind) • Vital Signs • Heart – Murmur – AS • Extremities – Pitting edema » Decompensated Heart Failure • Labs – • • If they are on diuretics consider lytes Consent obtained. Evaluation of NPO status – ASA guidelines: • For any elective procedure, the patient must be NPO for 8 hours prior to start for food intake, 6 hours for milk/formula, 4 hours for breast milk or clear liquids (adult), and 2 hours for clear liquids (child).

Airway Assessment • • • Note any airway deformities or difficulty opening the mouth (examine for any tracheal deviation). Recognize obese patients, those with limited flexion and extension of neck, those with rheumatoid arthritis or Down syndrome, and those with a small or receding chin can be difficult to mask ventilate and intubate. Recognize that edentulous patients and those with facial hair may also be difficult to ventilate with a mask.
 is a drug-induced state during")
Basics of Endoscopy Sedation • • Minimal Sedation (Anxiolysis) is a drug-induced state during which patients respond normally to verbal commands. Although cognitive function and physical coordination may be impaired, airway reflexes, and ventilatory and cardiovascular functions are unaffected. Moderate Sedation/Analgesia (“Conscious Sedation”) is a drug-induced depression of consciousness during which patients respond purposefully** to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are req Deep Sedation/Analgesia is a drug-induced depression of consciousness during which patients cannot be easily aroused but respond purposefully** following repeated or painful stimulation. The ability to independently maintain ventilatory function may be impaired. Patients may require assistance in maintaining a patent airway, and spontaneous ventilation may be inadequate. Cardiovascular function is usually maintained. General Anesthesia is a drug-induced loss of consciousness during which patients are not arousable, even by painful stimulation. The ability to independently maintain ventilatory function is often impaired. Patients often require assistance in maintaining a patent airway, and positive pressure ventilation may be required because of depressed spontaneous ventilation or drug-induced depression of neuromuscular function. Cardiovascular function may be impaired.

Key Information • When performing conscious sedation, do NOT simply give more meds because the pt is moving or occasionally groans. • Allow time for pt to wake up and follow commands. If they do not then the case can be aborted and pt can be coded as combative which will allow for a MAC by a CRNA or anesthesiologist. – Only Anesthesiologist or CRNA should intentionally induce a general anesthetic

Procedure • Monitors: – Vital signs are to be documented every 5 minutes throughout procedure. This includes: • Blood pressure, heart rate, respiratory rate, level of consciousness, and oxygen saturation. – RN administering IV sedation should have no other responsibilities during the procedure that would compromise continuous monitoring. – Physician MUST be present during administration of sedation and be available to assist with adverse events until discharge criteria is met. – Continuous Waveform Capnography is quickly moving towards the standard of care. • Who has it in their GI labs? • If you don’t have it, please work with your administration to move toward getting it. • If you don’t have it, make sure you are watching the airway closely for ventilation, not simply pulse ox or the chest moving.

Post Procedure • Vital signs taken every 15 minutes for an hour, every 30 minutes for 2 hours, or until discharge criteria met. • Discharge instruction given to a responsible adult, and patients are not permitted to drive. – Inpatients may resume routine care as ordered. • Significant changes from pre-operative condition should be reported. Discharge criteria to be met includes: – VS stable within 20% of pre-op values, can deep breathe and cough, move all extremities, easily rousable, skin color unchanged, and able to ambulate if applicable.

Procedure continued • The physician performing the procedure orders the medication given. • All medications given must be documented as well; including type, amount, and time given. • Adverse events should promptly be communicated with the physician and documented. • Assure there is a proper Quality Improvement/Quality Assurance (QI/QA)

Medications • Titrate all IV medications slowly to desired effect, ensure line is flushed well following administration to clear the tubing. – Be cautious of dosing with the elderly, and those with abnormal liver or kidney function as they may be more sensitive to the drugs effects. Try ½ dose at first. – Always push sedation drugs slowly

Medications • Have the appropriate reversal agents readily available. – Narcan/Naloxone • Narcotic antagonist • Dose: 0. 4 to 2 mg IV – Romazicon/Flumazenil • A benzodiazepine antagonist • Used to reversed • 0. 2 mg slowly, may repeat up to max of 1 mg – If a patient is given a reversal agent, watch closely over the next 30 -60 minutes as the reversal may wear off before the narcotic/sedative, once again unmasking its effects.

Supplemental Oxygen Delivery • Tips on oxygen delivery/flow – Nasal cannula is low flow oxygen • 1 -6 L delivers 24 -44% O 2 – Face mask • 8 -10 L delivers 40 -60% O 2 – Face mask with reservoir (ex. NRB) • 6 L is 60%/ 10 L is 100% O 2 delivery – Ambu-bag is 100% O 2 delivery • Be aware that patients who are obese, have sleep apnea, or those with beards/facial hair may be much harder to mask ventilate.

Airway Management • Equipment: – ALWAYS have readily available supplementary oxygen, ambubag and mask, and suction. – Know where to find crash cart and intubation equipment quickly if needed. • Observe the rise and fall of the chest, the rate of breathing, and for signs of airway obstruction. – Rocking motion in chest and abdomen, intercostal retractions, nasal flaring, stridor (harsh noises as patient tries to inspire), or place your hand in front of patients nose and mouth to feel if air is moving in and out. – They DIDN’T “Stop breathing”, their diaphragm is still moving, but their airway is occluded usually from upper airway, but occasionally from saliva or lube hitting the vocal cords causing a laryngospasm

Airway Management • To assist in opening the airway, first try a head tilt/chin lift. • Next try a jaw thrust to help displace the tongue from the posterior pharynx and stimulate breathing. • If both are unsuccessful, try an oral or nasal airway. • For continued obstruction: assist breathing with a bag and mask until sedation can be reversed. Important to watch for chest rise and fall.

How Its Paid For • Every outpatient endoscopy procedure is divided into Facility Fees and Professional Fees – Facilities vary whether it is hospital outpatient or ASC or office • Colonoscopy (Medicare pays about 750 for hospital outpatient and 420 for ASC) – Professional Fees can be for Anesthesia provider and for operating practitioner • Colonoscopy (Medicare pays about 217 to operating practitioner in facility and about 140 to the anesthesia provider • If a MAC is not required then no anesthesia professional fee is paid – Determine by payer’s LCD (Local Coverage Determinations) • Other possible costs/revenue include: redo procedure, barium enema or other imagine, and pathology costs including special stains

Alignment of Incentives • In the current system, the more you do, the more you make. • Recently via MACRA/MIPS for physicians and Bundled Payments for health systems and providers, insurers have begin to share savings and incentivize providers and health systems to strive for value • Remember Value =Quality/Cost – So either increasing quality OR decreasing cost increases value

Background Alternative Payment Models • This isn’t the first time these programs have been tried – For decades medicare has reimbursed hospitals via the inpatient prospective payment system via DRGs for hospital episodes not based on charges – Surgeons receive a global fee including their clinic visits, surgery and hospital visits – More recently they have extended the episodes • Medicare acute care episodes – Lower extremity joints, CABG, Valves, PCI • Medicare participating heart bypass center demonstration – CABG • Bundled payment for care improvement (BPCI) – 48 episodes available – Mostly Lower Ext joint replacement, CHF, Pneumonia were focused on – In spine cases, costs went up in BPCI group • Comprehensive Care for Joint Replacement Model (CJR) – Lower extremity joints – Even states have gotten onboard with private and insurance and Medicaid • Arkansas’ Episodes of Care

Background • Based on their previous experience, CMS first chose CJR as a mandatory bundle likely due to the savings seen in their previous programs without a dip in quality – First 21 months of BPCI for joint replacements showed no change in quality, but a decrease of 3286 dollars per episode in participants compared to a decrease of 2119 per episode in nonparticipants • This resulted in a net savings difference of 1167 dollars per episode between the 2 groups

CMS Goals • The stated improvement goals for CMS in their new EPMs – Post hospital follow-up and medical management for patients – Care coordination across the inpatient and post-acute care spectrum – Conducting appropriate discharge planning – Adherence to treatment or drug regimens – Reducing readmissions and complications during post discharge period – Managing chronic diseases and conditions that may be related to the EPMs episode – Choosing the most appropriate post-acute care setting – Coordinating between providers and suppliers

BPCI • Bundled Payment for Care Improvement – 4 models – Most chose model 2, where CMS pays fee for service, but reconciles at the end of the year and if certain quality measures are met and less money is spent on a care episode than is expected, then that savings is shared with the health system and the provider

What are the Options? BPCI • • • • • • Major joint Upper Ext - Ortho Amputation - Ortho, Podiatry, Gen Surg Urinary Tract Infection - Hospitalist, IM Stroke - Neuro, IM, Hospitalist COPD - IM, Hospitalist, Pulm CABG - Card Surg Major Joint Lower Ext - Ortho Percutaneous Coronary Intervention - Int Cards Pacemaker - Int Cards Cardiac Defibrillator - Int Cards Pacemaker replacement or revision - Int Cards AICD - Int Cards CHF - Cards, IM, Hospitalist AMI - Cards, IM, Hospitalist Cardiac Arrhythmia - Cards, IM, Hospitalist Cardiac Valve - Card Surg Other Vascular Surgery - Vasc Surg Major Cardiovascular Procedure - Card/Vasc Surg GI hemorrhage - IM, Hosp, GI, Gen surg Major Bowel Surgery - Gen surg, Colo surg Fractures Femur Hip/Pelvis - Ortho Medical Non-infectious Orthopedic - IM, Hospitalist, Ortho Double Joint replacement Lower Ext - Ortho Revision of the Hip or knee - Ortho • • • • • • Spinal Fusion Non-cervical - Ortho/Neuro spine Hip and Femur procedure except major joint - Ortho Cervical Spinal Fusion - Ortho/Neuro Spine Other Knee Procedure - Ortho Complex non-Cervical Spinal fusion - Ortho/Neuro Spine Combined AP spinal Fusion - Ortho/Neuro Spine Back and neck except spinal fusion - Ortho/Neuro Spine Lower Ext and Humerus procedure except hip, foot, femur Removal of orthopedic devices - Ortho Sepsis - IM, Hospitalist, ER Diabetes - Endo, IM, Hospitalist Simple pneumonia and respiratory infections - IM, Hospitalist, Pulm Other respiratory - IM, Hospitalist, Pulm Chest Pain - IM, Hospitalist, Cards Medical Peripheral Vascular Disorders - IM, Hospitalist Atherosclerosis - Cards, IM, Hopsitalist Gastrointestinal Obstruction - Gen Surg, IM, Hospitalist Syncope and Collapse - IM, Hospitalist, Neuro Renal Failure - Neph, IM, Hospitalist Nutritional and Metabolic Disorders - Endo, IM, Hospitalist Cellulitis - IM , Hospitalist, Gen Surg Red Blood Cell disorders - Heme, IM, Hospitalist Transient Ischemia - Neuro, IM, Hospitalist Esophagitis, gastroenteritis, and other digestive disorders - IM, GI, Gen Surg, Hospitalist

90 Day Episode Costs Anchor Cost Post-Acute Cost Unadjusted Episode Cost Estimated Target Difference Price* ** $11, 371. $34, 712. $46, 083. $16, 904. ($18, 724. ) $12, 132. $15, 558. $27, 690. $16, 904. ($10, 786. ) $12, 828. $27, 774. $40, 603. $32, 302. ($8, 301. ) $11, 760. $12, 370. $24, 130. $32, 302. $8, 172. $11, 347. $5, 527. $16, 874. $32, 302. $15, 427. $11, 550. $4, 642. $16, 193. $32, 302. $16, 109.
 – Protocol Adherence (optimization)")
Stakeholders % Share • Citizenship Measures – Meeting Attendance (20%) – Protocol Adherence (optimization) (20%) • Outcome Measures – DVT Rate (90 days) (15%) – Readmission Rate (30 days) (15%) – Reoperation Rate (90 days) (15%) – SSI (90 days) (15%)

Gain Sharing Report Card

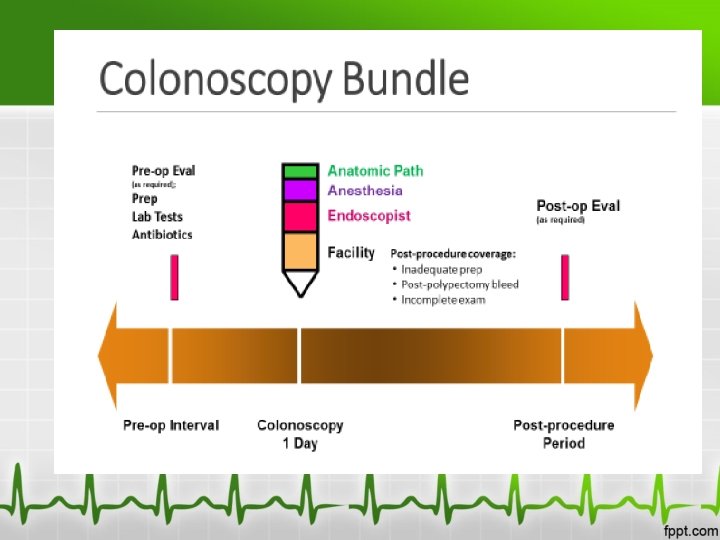
Proposed Bundle for Colonoscopy • Digestive Health Network led by Dr Joel Brill submitted a proposal for a colonoscopy bundle December 28, 2016 • It is not a matter as to whether something like this is approved……. but when

Colonoscopy Bundle • The proposed bundle will track total costs and utilization and reward groups for costsavings while maintaining a high quality. • Measures such as redo rate, anesthesiology utilization, ASC utilization, post op ER visits…

GI Nurse Opportunity • Health Systems are in uncharted waters • Gone are the days where the only thing that matters is volume and efficiency • Who better than to give ideas to drive up quality or drive down costs?

Cost Saving Questions • Can more cases safely be done at ASC rather than hospital outpatient setting? • Can cancellations and repeat procedures be avoided by a preop call to evaluate prep? • Can cases be rearranged or placed at the end of the day to continue prep rather than reschedule • Can a higher percentage of cases be done under conscious sedation rather than with an anesthesia provider?

Sedation Savings • Propofol – Proven safe for many patient, but many political hurdles, likely will improve throughput compared to versed and fentanyl • Physician Expectations – Many operating practitioners don’t understand that conscious sedation is not general anesthesia – They also don’t understand the cost differences • Hybrid Models – MAC vs conscious sedation – Anesthesia availability if needed on failed cases – CRNA availability, MD consult available

Bottom Line • The new changes with payment models can be something people dread, but it can also be a huge opportunity to create a system that is more cost effective and also more safe.

Change • “In times of change, learners inherit the earth, while the learned find themselves beautifully equipped with a world that no longer exists. ” • ---Eric Hoffer

Any Questions

References • • • ASA: Continuum of depth of sedation: Definition of general anesthesia and depths of sedation/analgesia. October 2014. Brill J. Proposal for a Physician-Focused Payment Model: Comprehensive Colonoscopy Advanced Alternative Payment Model for Colorectal Cancer Screening, Diagnosis and Surveillance. December 28, 2016. Guidepoint Reimbursement Resource Feb 2016. Morgan, G. E. , Mikhail, M. S. , & Murray, M. J. (2006). Clinical Anesthesiology (4 th ed. ). New York: Mc. Graw-Hill. Schroeder, J. (2008). Moderate sedation study module for nonanesthesiologists. Retrieved March 18, 2010, from www. jupitermed. com/workfiles/PDFfile. White River Medical Center. (2004). Conscious sedation for diagnostic therapeutic procedures. Surgery Policy and Procedures Manual, 1.
- Slides: 41