Endoscopic Vein harvesting Is there a learning curve




 • Secondary outcome measures: –")
: – – – – 3 cases done off pump (no")
 –")
 Routine Aprotinin (n = 148) Radial artery")
 EVH (n=117) mean Age 67. 5 66. 5 No of grafts 3.")
 5 (5%) Leg wound")

 –")
 EVH (n=101) Preop 1. 9")
 EVH (95) Pre-op 2. 1")



")

- Slides: 20
Endoscopic Vein harvesting: Is there a learning curve effect on patient outcomes? Joseph Zacharias & Bilal Kirmani Lancashire Cardiac Centre Blackpool England
Lancashire Cardiac Centre 2008: 950 cardiac cases 350 Thoracic cases 2009: 1035 cardiac cases 450 thoracic cases 2010: 1200 cardiac cases 600 thoracic cases
Background • Endoscopic Vein harvesting has been developed over the past decade mainly in the US. • The short term benefits on leg wounds are impossible to deny • A recent sub group analysis of a randomised trial cast doubt on 2 year clinical outcomes. • In the UK with a high level of public scrutiny there is a concern in adoption of new technology due to its potential learning curve impact.
Methods • Design – Review of prospectively collected data. – Consecutive first time CABG – Retrospective patient cohorts • Inclusion Criteria: – Two or more vessel disease – Operated on by a single surgeon • Exclusion Criteria: – – Previous Cardiac surgery Concomitant Valve surgery Radial artery use Routine use of aprotinin
Methods • Primary outcome measures: – Mortality (Civil registry) • Secondary outcome measures: – Major Adverse coronary events (clinical MI, ACS, need for revascularisation) – Cardiac related readmissions – Freedom from angina, dyspnoea – New anti-anginals, – Wound pain, – Self reported health status
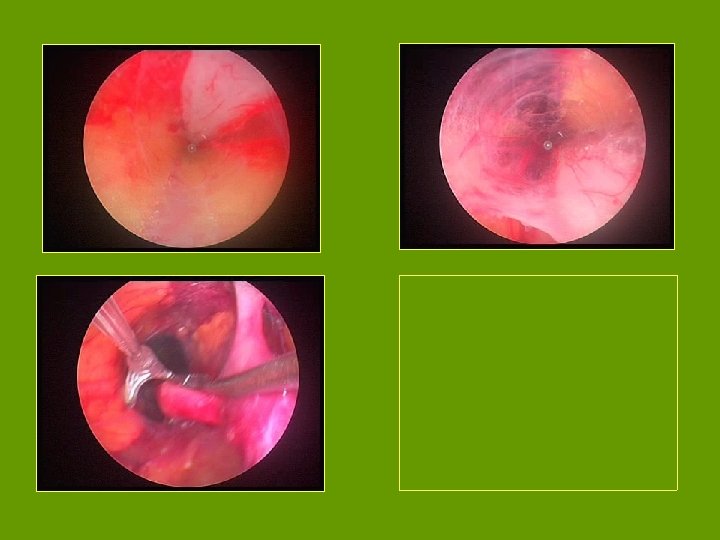
Technique • CABG (EVH): – – – – 3 cases done off pump (no touch) 114 cases done on pump Two stage Venous cannulation Straight aortic cannulation Centrifugal pump on bypass Single cross clamp technique Intermittent cold blood antegrade cardioplegia. • Open vein Harvesting: – Harvest by Surgical Care Practitioners or Registrars – CABG: Same technique as above. – 5% Off Pump (no touch)
EVH technique • EVH: – Vasoview 6, 7, Haemopro systems (Maquet Inc. ) – Carbon dioxide insufflation (pressure controlled to <10 mm. Hg) – 2, 500 iu heparin prior to insufflation – Bipolar diathermy until Haemopro – Titanium clips to side branches
Patients undergoing CABG under JZ (n: 495) Routine Aprotinin (n = 148) Radial artery Conduit = (48) Eligible = 299 EVH (n = 117) OVH (n = 182) Lost to follow up ( n = 21) Lost to follow up ( n = 77) Primary Endpoint analysis (n = 116) Primary Endpoint analysis (n = 180) Secondary Endpoint analysis (n =95) Secondary Endpoint analysis (n = 103)
OVH (n=182) EVH (n=117) mean Age 67. 5 66. 5 No of grafts 3. 5 3. 2 Euro. SCORE 3. 4 3. 3 Trainee Cases 42% 64% Cross clamp Time 64 65 Bypass Time 81 84 CVA 1 0 In Hospital Deaths 2 (1. 09%) 1 (0. 85%)
Results: Leg Wound OVH EVH Leg wound problems 29 (28%) 5 (5%) Leg wound pain Mean +/- SD 1. 0 +/- 2. 3 1. 3 +/- 1. 4 Sternal wound pain Mean +/- SD 0. 8 +/- 0. 9 1. 6 +/- 1. 3
Major adverse Clinical events • Need for new anti-anginals – OVH: 13 (12%) – EVH : 9 (9%) • Further cardiac related admissions – OVH: 9 (9%) – EVH: 5 (5%)
Results: Quality of Life: Dyspnoea NYHA class OVH (n=105) EVH (n=101) Preop 1. 9 +/- 0. 8 2. 1 +/- 0. 8 Post op 0. 5 +/- 0. 9 0. 8 +/- 0. 9
Quality of Life : Angina CCS status OVH (105) EVH (95) Pre-op 2. 1 +/- 1. 1 2. 2 +/- 1. 0 Post-op 0. 2 +/- 0. 6 0. 2 +/- 0. 7
Self rated health status • Relative health: – Very Good or Excellent: 52% in OVH 61% in EVH • Relative health: – Much Better : 81% in OVH 90% in EVH
Results: Survival
Learning curve: Time A prospective audit of endoscopic vein harvesting for coronary artery bypass surgery ZAKARIYA WAQAR-UDDIN, MANOJ PUROHIT, NADENE BLAKEMAN, JOSEPH ZACHARIAS Ann R Coll Surg Engl 2009; 91: 426– 429
Learning curve: Conversion • Initial audit 25 patients – Conversion rate of 3 (12%) – Reasons: • Unable to find vein : 2 • Poor caliber vein harvested: 1 • In 117 patients: – Conversion rate < 8% – Reasons: • Poor vein caliber: >80% • Poor vein quality: <10%
Conclusion • Our review suggests: – Endoscopic vein harvest can be introduced into every day practice without an obvious impact on patient outcomes – Despite the limitations of the size of the study at a median of 20 months we found, at least equivalent, survival and freedom from angina in patients at the start of our program.