Endoscopic Ultrasound Applications in Premalignant and Malignant Disease







")




















")


























")














")
")





- Slides: 110
Endoscopic Ultrasound: Applications in Pre-malignant and Malignant Disease December 20 th, 2010 Andrew T. Pellecchia, MD Director of Advanced Endoscopy Jacobi Medical Center
EUS Originally utilized to ‘clear’ the bile duct precholecystectomy in patients with suspected CBD stones Less invasive alternative to ERCP Risks similar to standard EGD EUS still used for this indication Less than 20% of EUS procedures are performed for this indication in established advanced endoscopy center
Evolution of EUS as an imaging study EUS as a means of fluid and tissue acquisition Cancer staging Cyst analysis EUS as an interventional/therapeutic modality Neurolysis Transmural cyst drainage Direct access to biliary system More…
Overview Several illustrative EUS cases from JMC Basic EUS principles What is ‘within reach’ of EUS +/- FNA? Brief overview of selected diseases
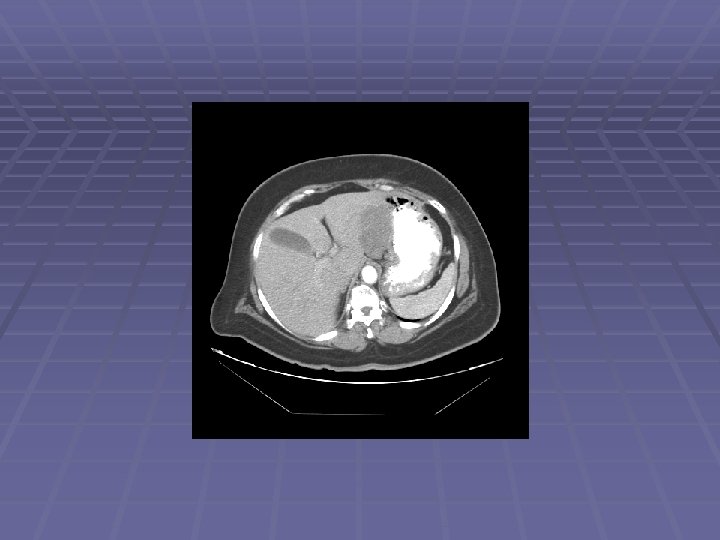
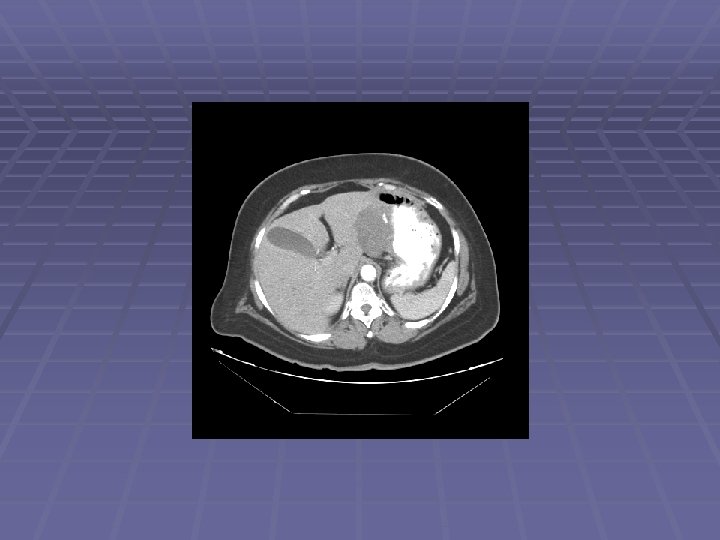
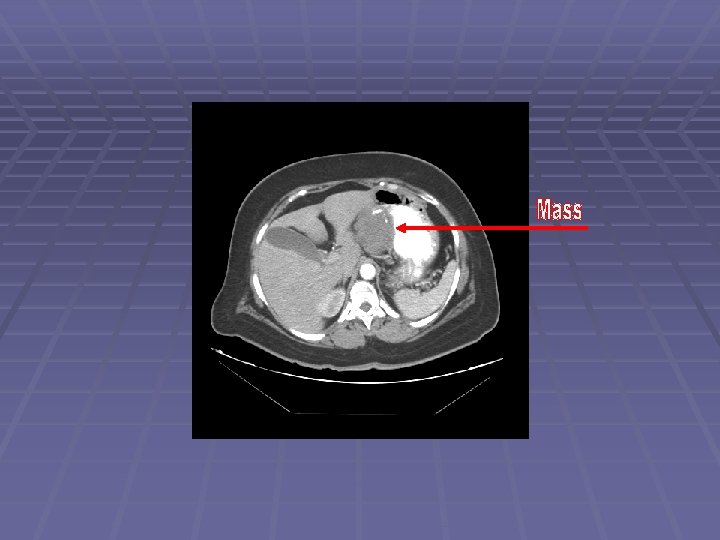
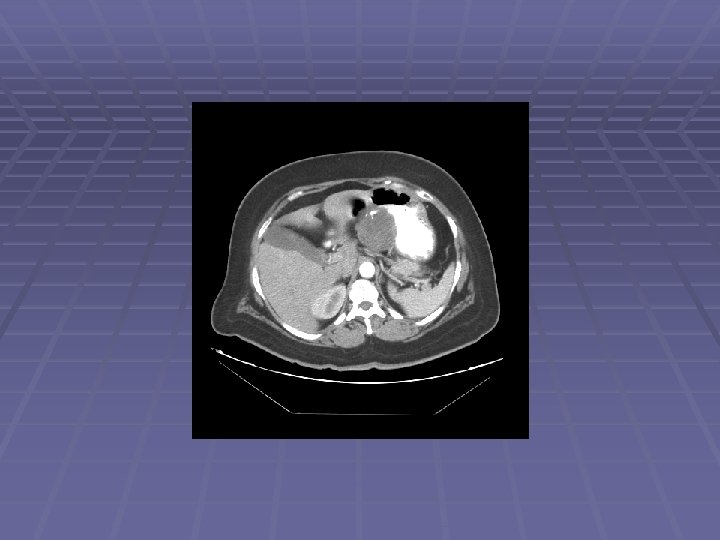
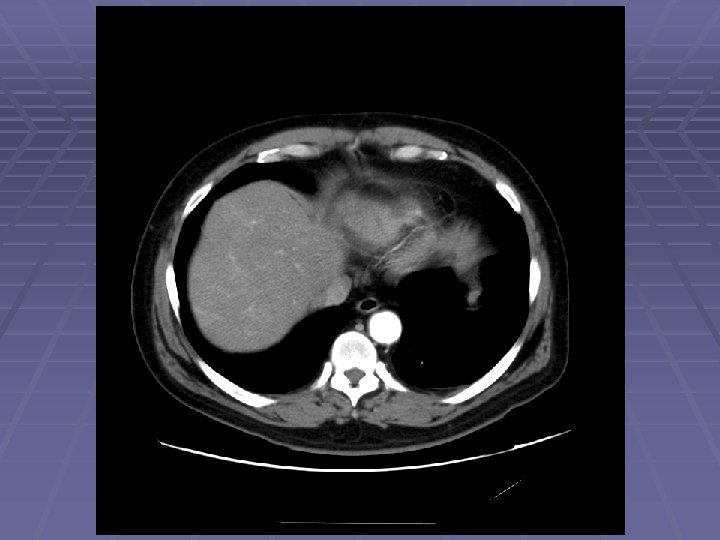
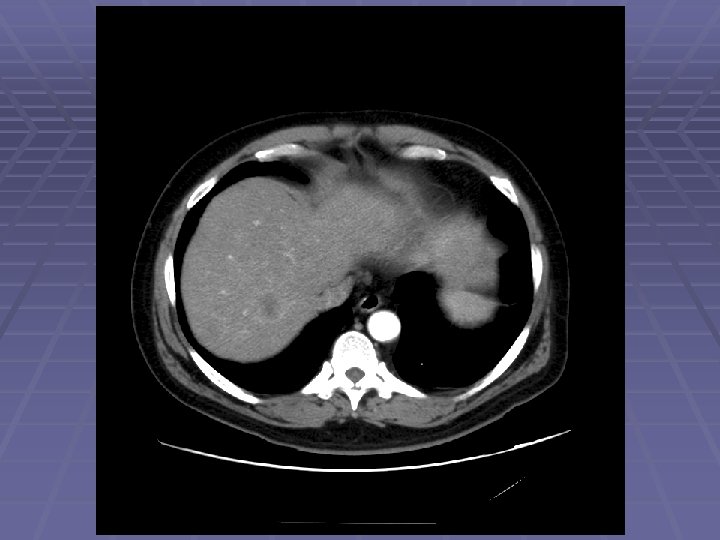
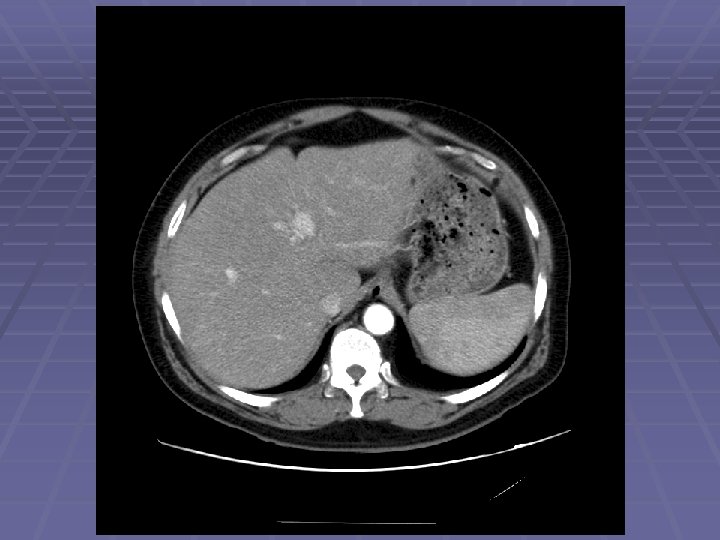
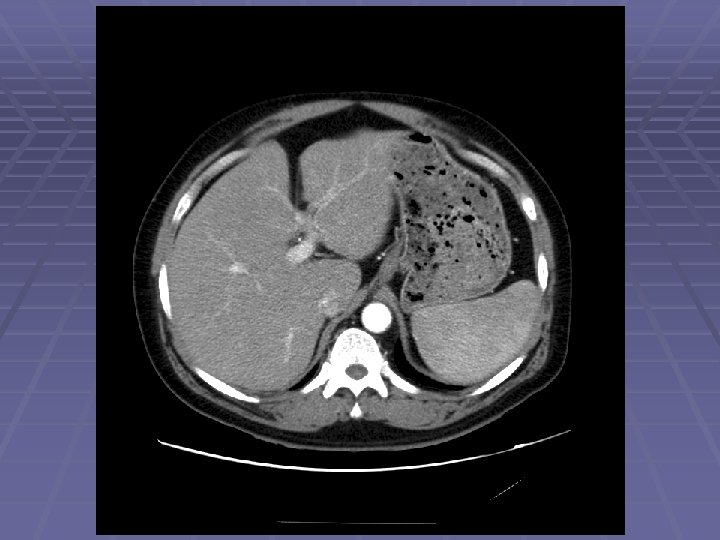
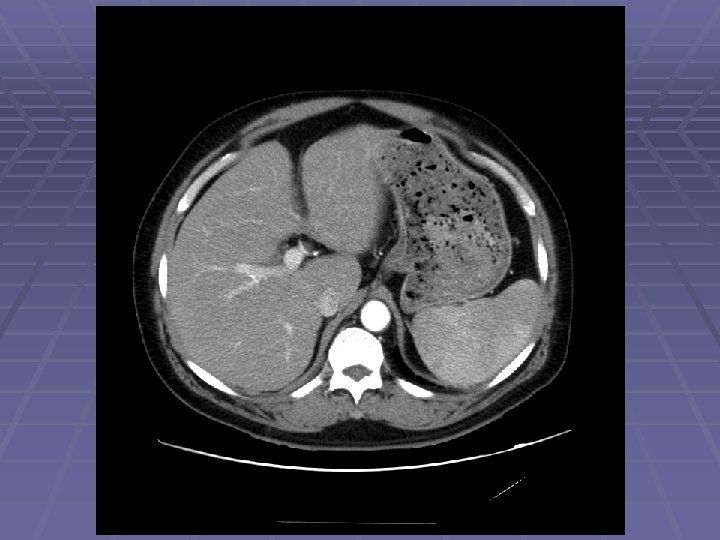
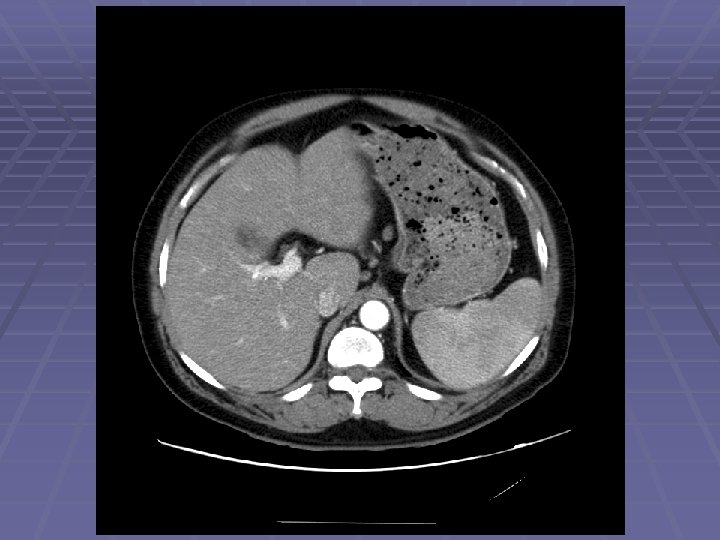
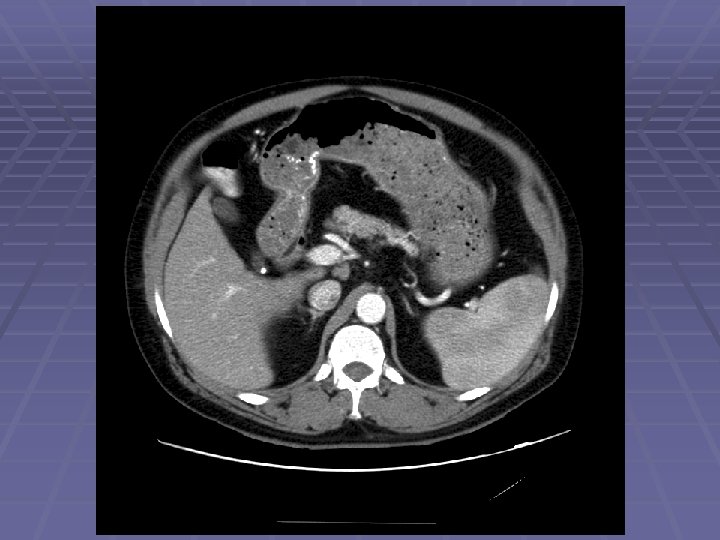
Patient GR 62 y. o. woman with significant weight loss over the past 6 months CT a/p shows a 6 cm intra-abdominal mass EGD/EUS/FNA planned to further evaluate lesion
Endosonographic Evaluation EGD showed normal gastric mucosa with evidence of mild external compression vs. submucosal lesion in the area of the gastric incisura EUS Clear demarcation of hypoechoic mass adjacent to left lobe of the liver FNA was performed
GR-GIST H&E
GR-GIST C-KIT (CD 117)
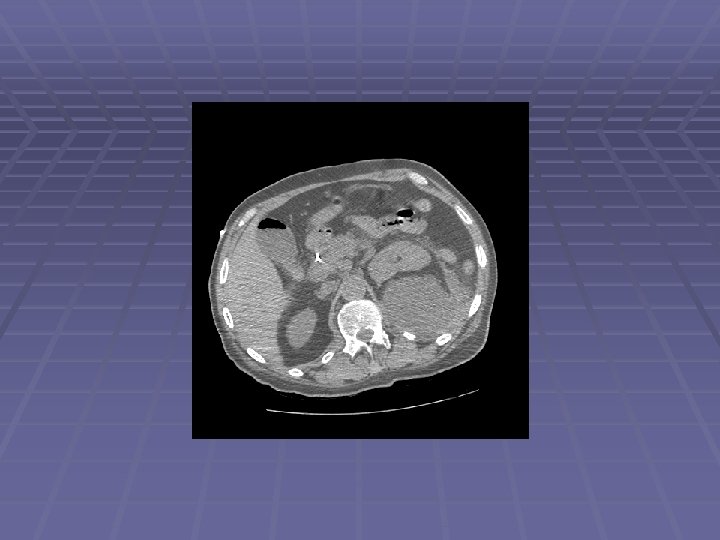
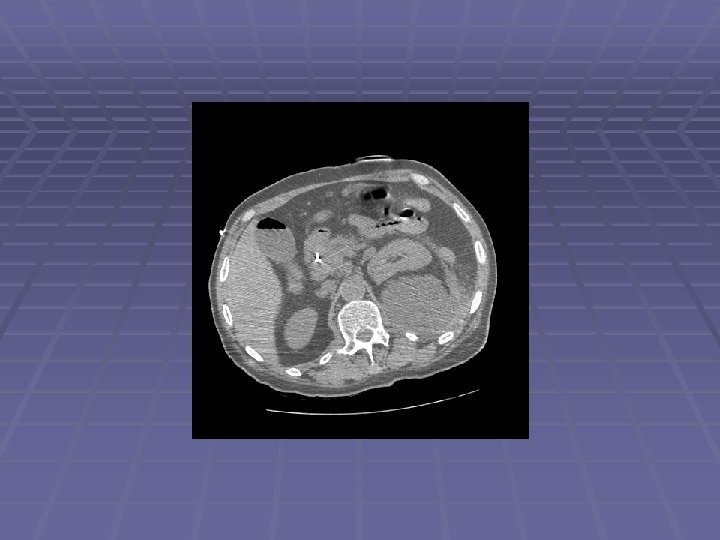
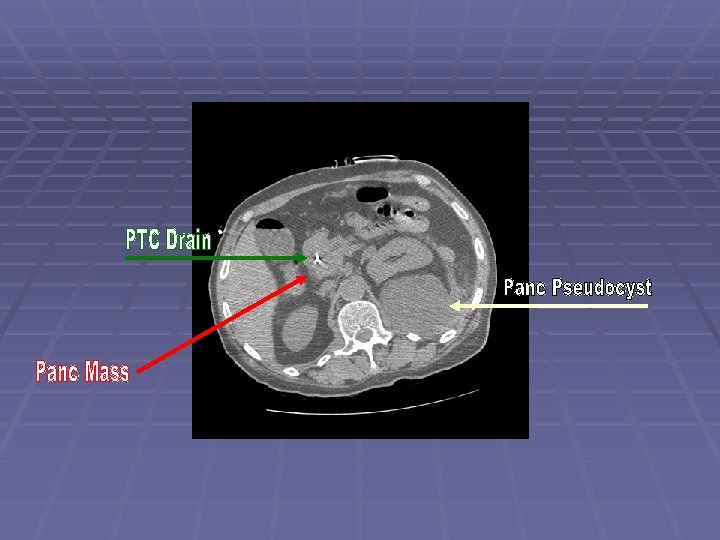
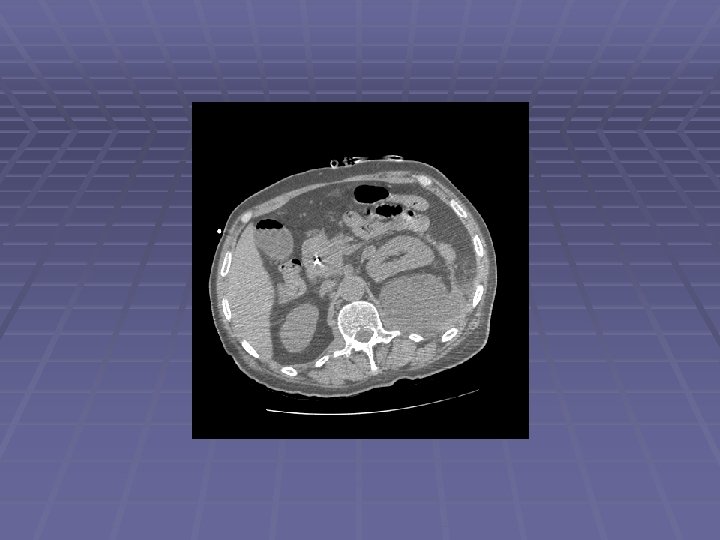
Patient DD 62 y. o. man with history of alcoholism and recurrent pancreatitis since the 1970’s, admitted to an outside hospital with jaundice MRI showed a large pancreatic head mass ERCP for biliary drainage – failed Complicated PTC by pancreatic tail pseudocyst formation with internalization - successful Patient left AMA and came to JMC EUS/FNA performed to obtain diagnosis
Endosonographic Evaluation EUS Large ~30 mm hypoechoic pancreatic head mass surrounding the intrapancreatic CBD with PTC drain seen within CBD Dilated PD to 5 mm with evidence of chronic pancreatitis FNA performed
DD- Pancreas Ca. Pap stain
DD-Pancreas Ca. Pap stain
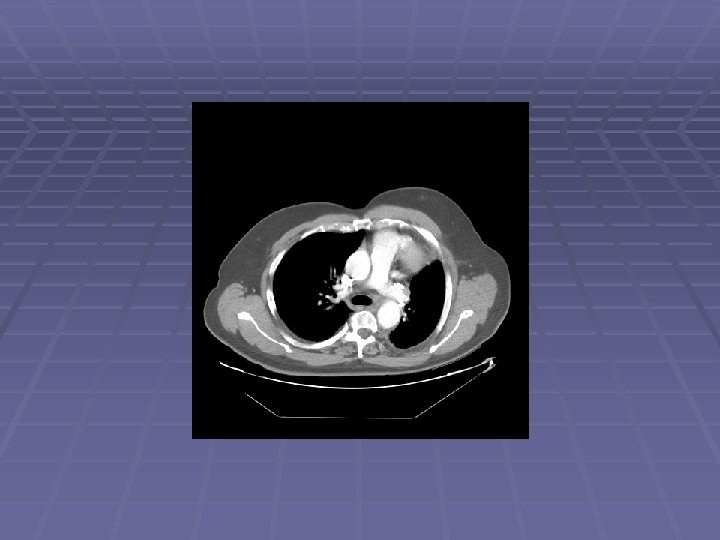
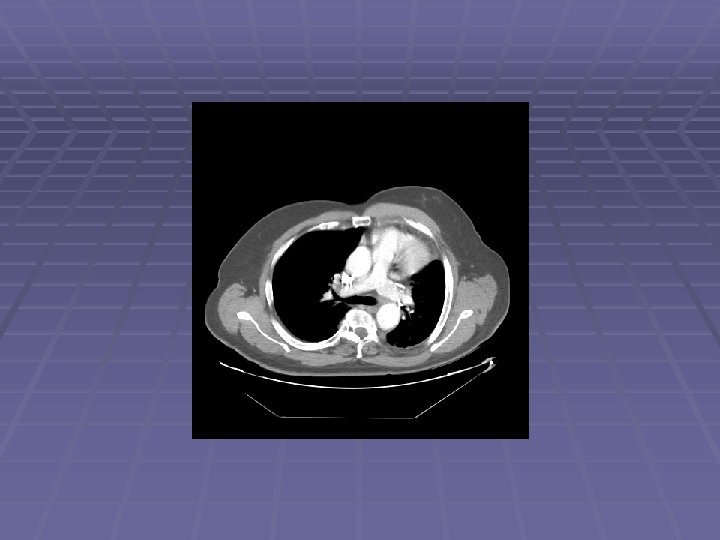
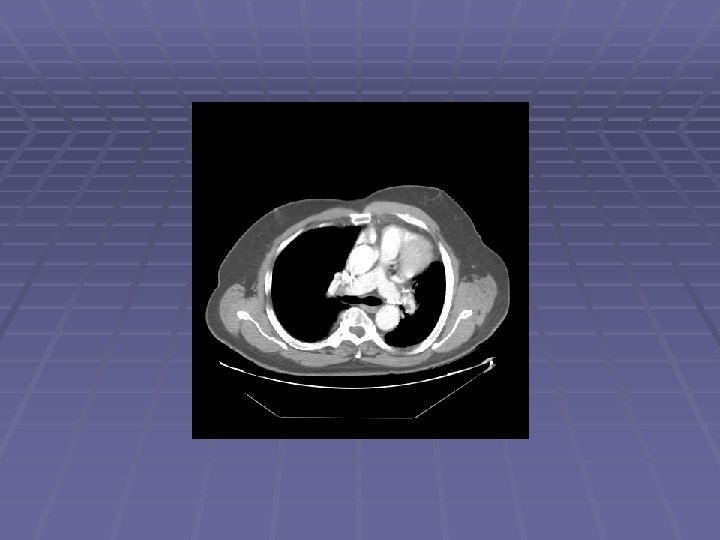
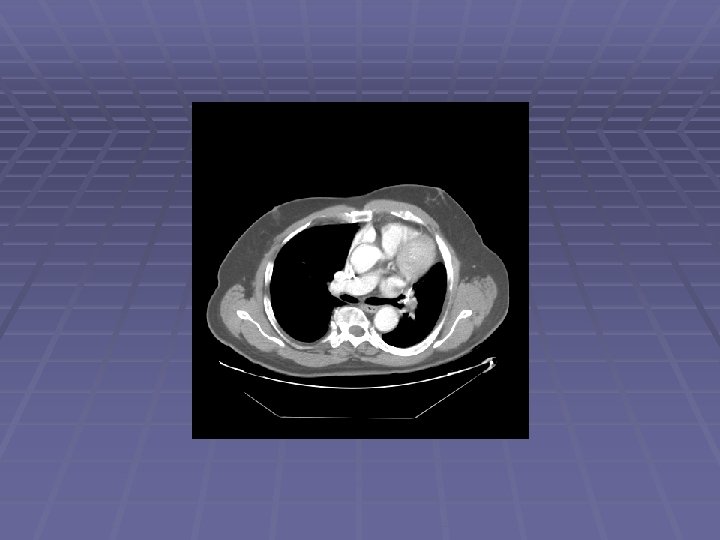
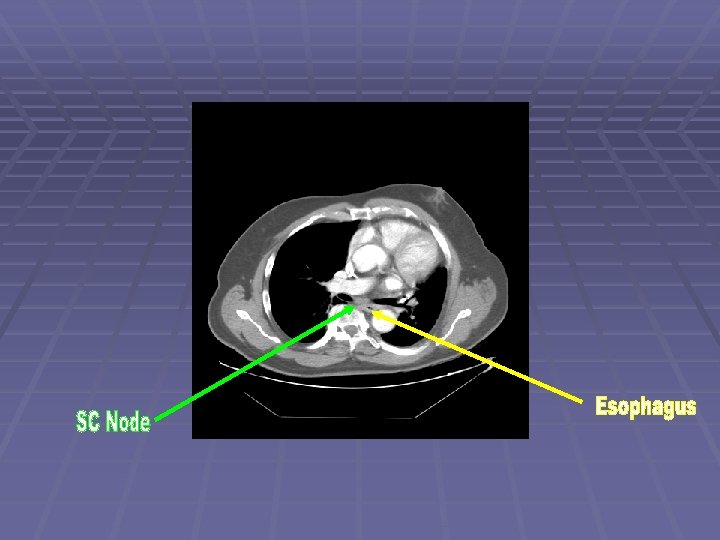
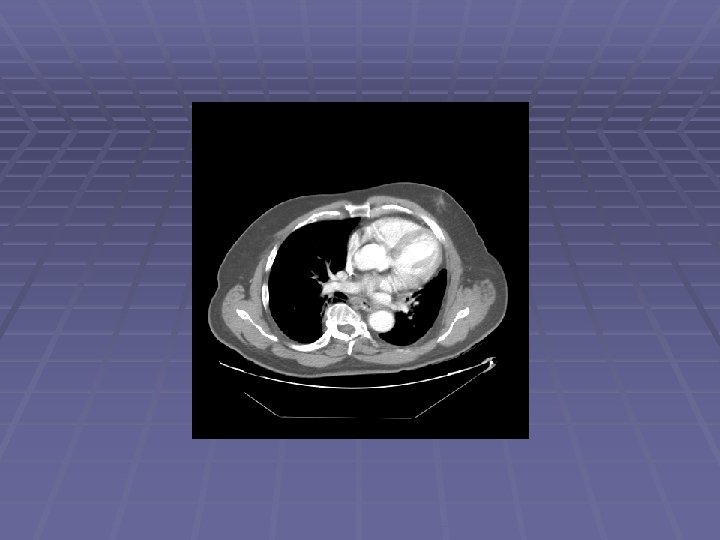
Patient CE 69 y. o. man with h/o non-small cell lung cancer s/p LUL resection in 2006 who is referred after a chest CT showed new mediastinal lymphadenopathy EUS/FNA scheduled to evaluate for recurrent disease
Endosonographic Evaluation EUS Suspicious lymph nodes in the aortopulmonary window, sized 6 -11 mm Suspicious lymph nodes in the subcarinal space, sized 6 -12 mm FNA performed
CE-Non-small cell ca. Pap stain
CE-Non-small cell ca. Pap stain
Radial Ultrasonography Oblique-viewing instruments with an ultrasound transducer located at the tip The circumferential ultrasound image is perpendicular to the long axis of the endoscope
Linear Ultrasonography Ultrasound image parallel to the long axis of the endoscope Capable of performing real time, ultrasound directed needle aspiration biopsy Color Doppler analysis
Working End of Linear Echoendoscope
What The Scope of the Echoendoscope can be assessed by EUS with potential FNA? Any structure within several cm of U/L GI tract Ability to see structures measuring 1 mm Ability to perform FNA upon structures measuring 3 mm Limitations Cannot visualize beyond air-filled structures Cannot biopsy through air-filled structures, blood vessels, or the heart Lung that is non-adjacent to esophagus, trachea, aorta, pulmonary artery, r/l atria
Risks of EUS FNA Pancreatitis < Significant bleeding < 1: 500 Perforation < 1: 1000 Infection - rare Antibiotics for transrectal FNA or FNA of cysts Inadequate tissue 1: 10 to 1: 5 Can be related to pathology of lesion Cholangio, GIST
Thyroid Mass
FNA of Thyroid Mass
Right Lower Pole Kidney Mass
EUS in Pre-Malignant Disease Pancreatic Cysts PD fluid analysis Pancreatic screening in high risk populations Chronic pancreatitis Family history of pancreatic cancer Cancer syndromes Submucosal Pancreatic lesions rests
Pancreatic Cystic Fluid Analysis Incidental pancreatic cysts seen in up to 20% of abdominal CT’s performed for any reason Cystic lesions of the pancreas, even when found incidentally, may represent malignant or pre-malignant lesions The majority of pancreatic cysts require evaluation by EUS/FNA measurement of CEA, amylase, genetic markers Relatively sensitive and specific for differentiating mucinous cysts (IPMN, MCA) from non-mucinous cysts (SCA, Pseudocyst)
HOP Serous Cystadenoma
BOP Serous Cystadenoma
Oncology Consult? (FNA benign: Island of normal pancreatic tissue within serous cystadenoma)
Patient PS Media reports state that the actor was diagnosed with an IPMN is a pre-cancerous lesion Conclusion: the IPMN had already progressed to adenocarcinoma prior to diagnosis/resection Resected IPMNs often have foci of adenocarcinoma Lesson: ALL pancreatic cysts need to be referred for risk stratification
EUS in Malignant Disease Non-small cell lung cancer Pancreatic cancer Esophageal and gastric cancer Cholangiocarcinoma Rectal adenocarcinoma Metastatic disease Lymph nodes: aortopulmonary, subcarinal, paraesophageal, celiac, intra-abdominal Left lobe of liver Left adrenal And beyond – right lobe of liver, right adrenal, . . .
EUS and Lung Cancer “We really do not need additional proof before EUS-FNA is considered the gold standard for invasive staging of non-small cell lung cancer and for diagnosis of posterior mediastinal lesions; there is little to lose and much to gain. ” -P. Vilmann and S. S. Larsen, Eur Respir J 2005; 25: 400– 401
EUS and Lung Cancer
Lymph Node Stations
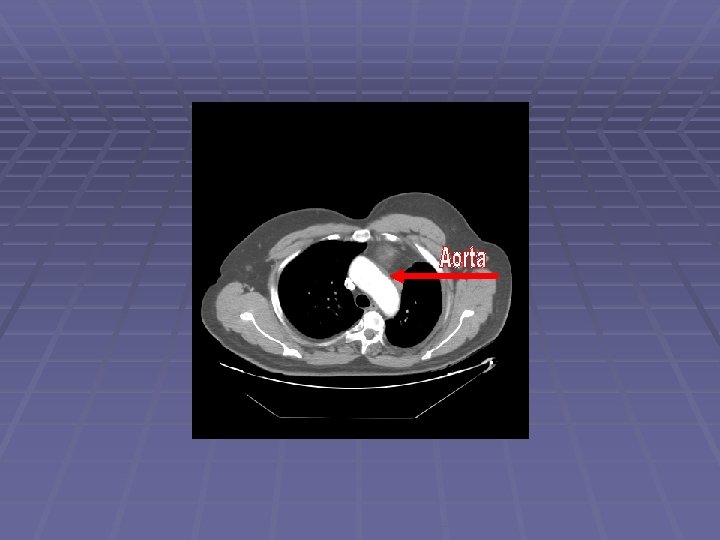
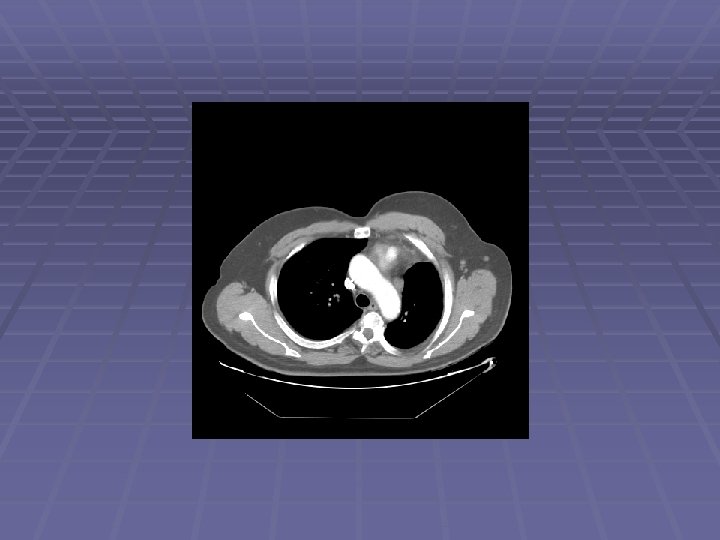
Normal AP Window
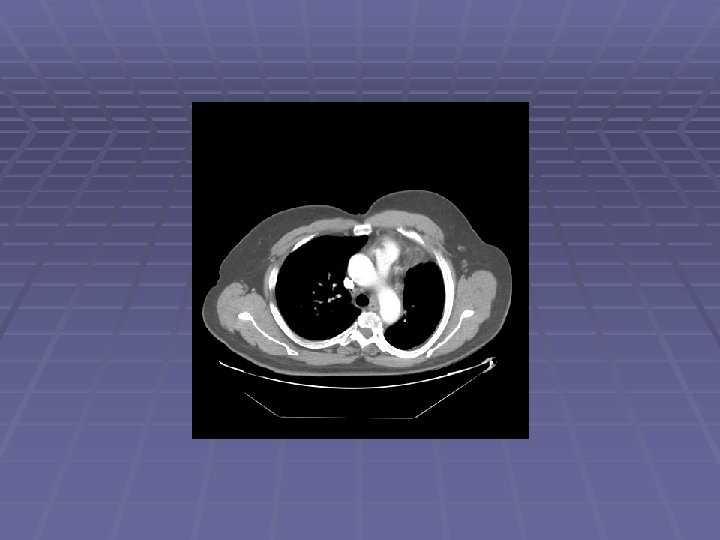
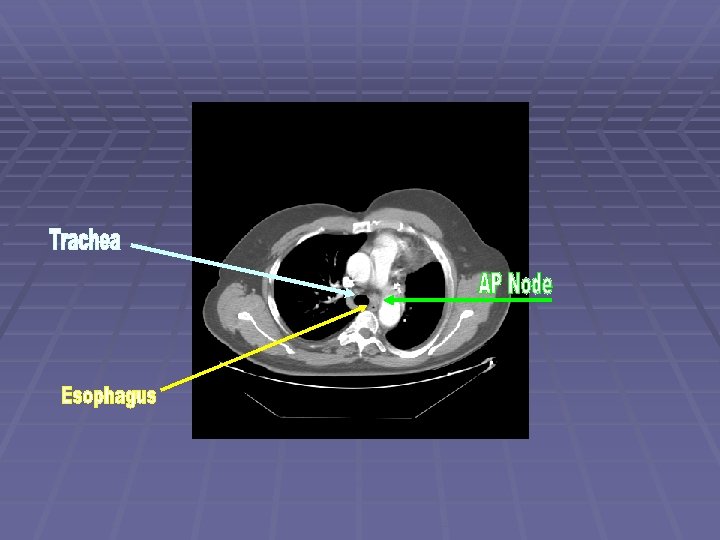
LAD at AP Window
FNA at AP Window
Subcarinal Space
LAD in Subcarinal Space
Likely Benign Abd LAD
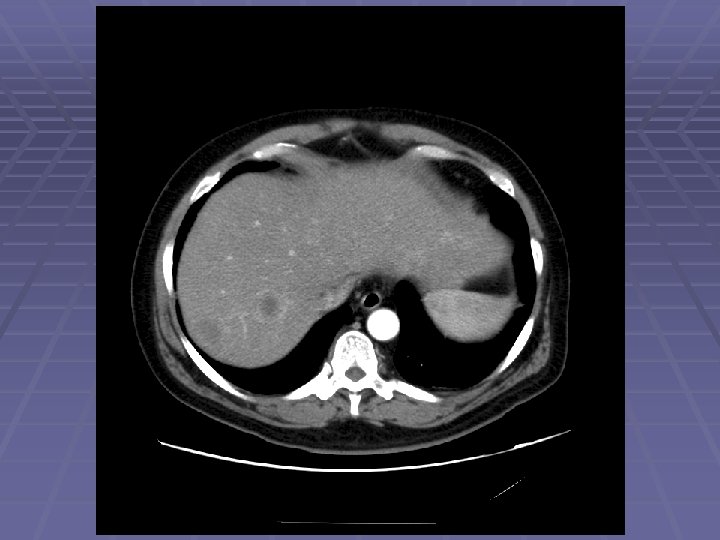
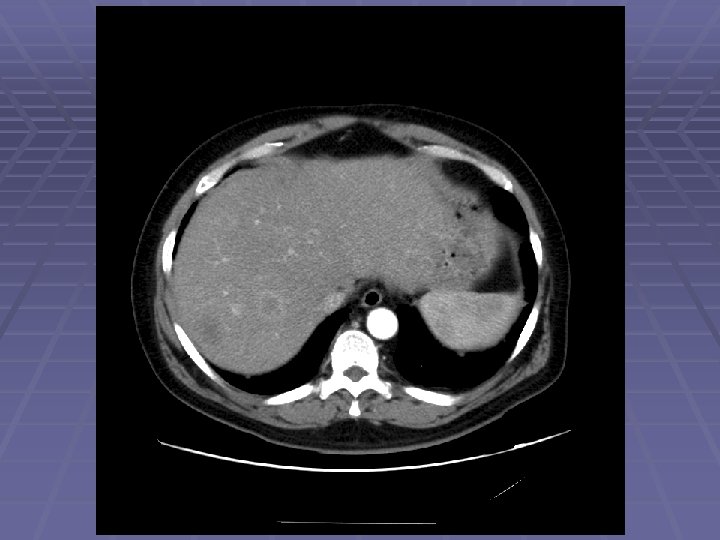
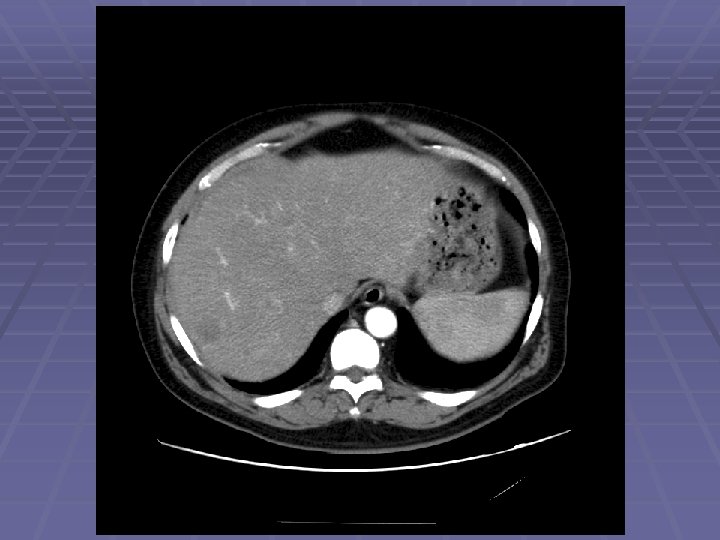
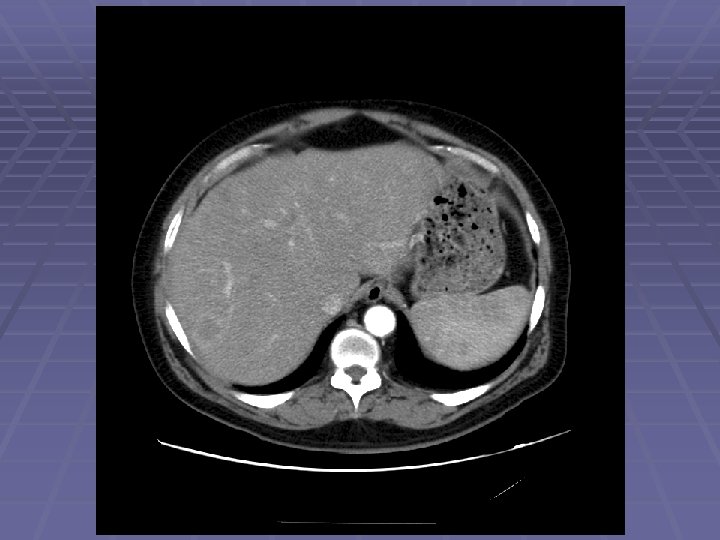
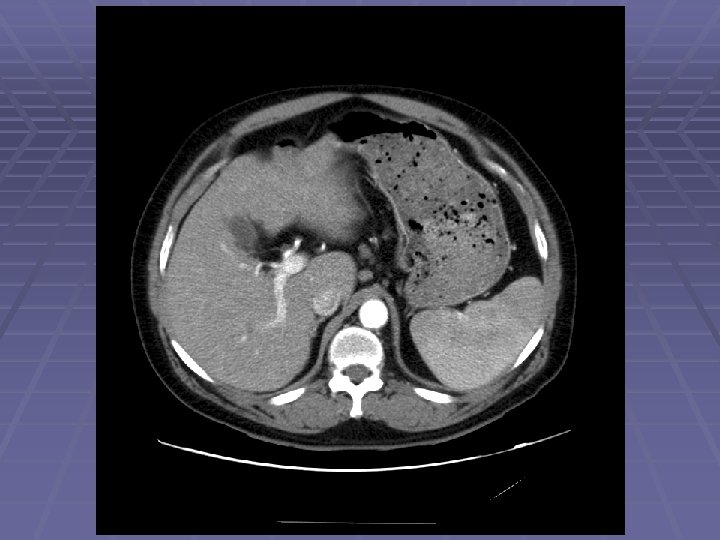
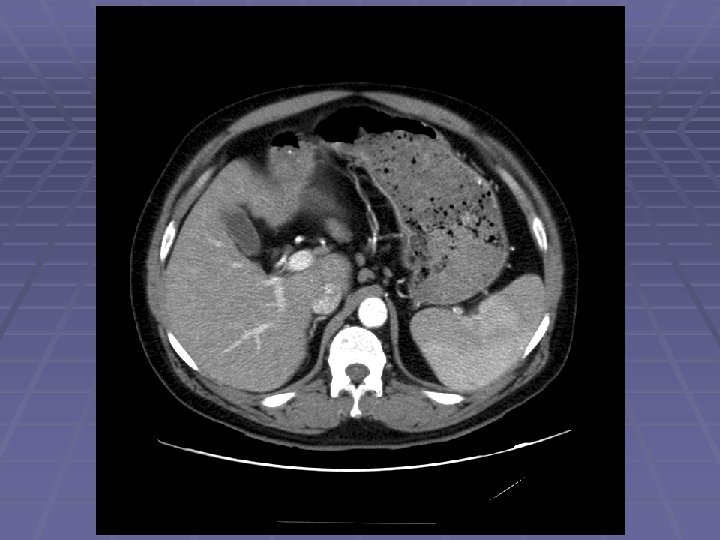
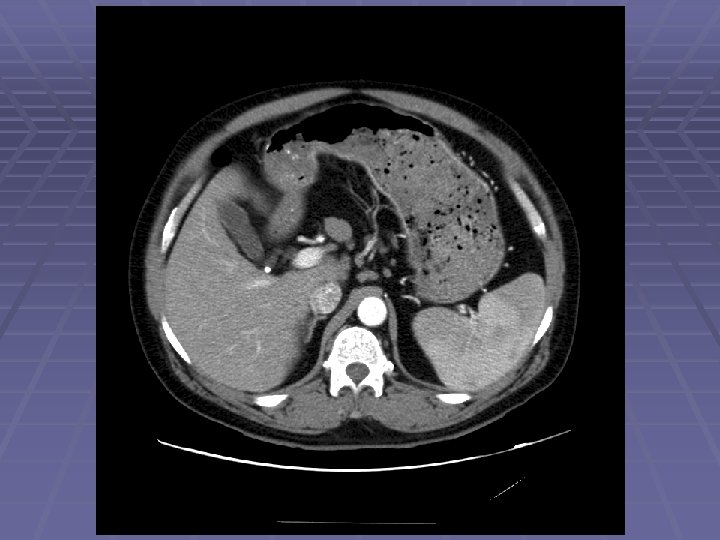
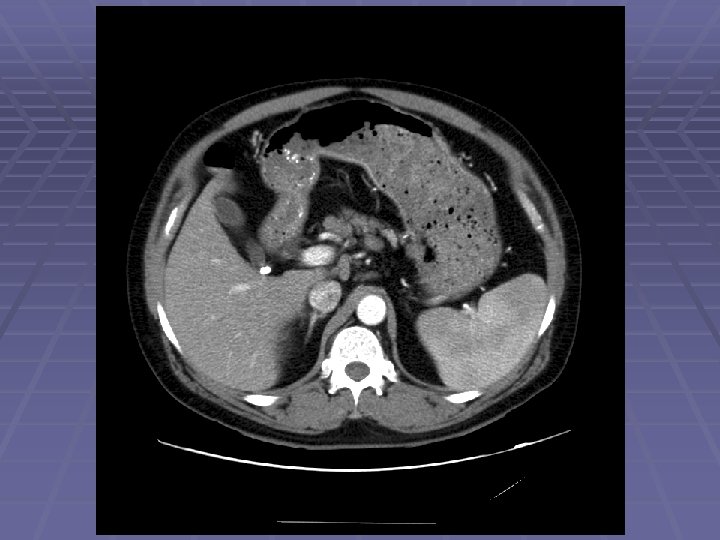
Pancreatic Mass
Pancreatic Mass at CT
Pancreatic Mass at CT
'Pancreatic' Mass at EUS
FNA of Peri-pancreatic Mass § Metastatic Leiomyosarcoma
Liver Mass
FNA of Liver Mass
Hyperechoic Liver Masses
FNA of Hyperechoic Liver Mass
EUS Evaluation of Left Lobe of Liver
Abdominal LAD
EUS/FNA of Periportal LN
Primary Target Fail…
…Secondary Target Acquired (Carcinoma at FNA)
Normal Left Adrenal
Left Adrenal Met in NSCLC
Normal GI Wall Layers
Normal Esophagus and Cyst
Distal Esophageal Lesion
Normal Gastric Wall Layers
Mucosal Lesion
Mucosal Lesion
Malt Lymphoma
Gastric Lipoma
T 2 Gastric Adenocarcinoma Invasion of Muscularis With Intact Serosa
T 3 Gastric Cancer
T 1 Rectal Cancer by EUS
T 2 Rectal Cancer
Rectal Mass at CT: T 4? (Apparent invasion of uterus)
Further History: Recent IUD Removal (Actinomycosis)
Celiac Plexus Neurolysis
Celiac Axis
Key Points All patients with pancreatic cysts should have consultation for possible EUS/FNA is the standard of care in the loco-regional staging of many cancers Lung Esophageal Gastric Pancreatic Cholangiocarcinoma Rectal adenocarcinoma
Key Points, Continued EUS is minimally invasive Reduces need for mediastinoscopy, surgical biopsy, bronchoscopy, CT guided biopsy Reduces morbidity/mortality while reducing health care costs Appropriate Prevents cancer staging unnecessary surgical resections Identifies patients who will benefit from pre-op chemo/xrt
Cutting Edge EUS Applications Role for EUS is expanding EUS placement of fiducials for radiation therapy EUS rendezvous procedure for accessing CBD EUS directed brachytherapy EUS guided hepaticogastrostomy for malignant CBD obstruction