Endodontic Emergencies Its all about the pain and
.")
Endodontic Emergencies “It’s all about the pain and swelling” Dr Daniel Farmer BDS. MDS(Endo). FRACDS. FADI. FICD.

Emergency Care Protocol All emergency appointments result from acute cases of infection or inflammation Basic principles to be followed: Correct diagnosis Treatment of the causative agent Drainage Medication - local - systemic (post operative) Rest

• Correct diagnosis Chief Complaint Medical History Emergency examination • Treatment of the causative agent Breaking the “pain cycle” - administration of LA Endodontic therapy / Extraction • Drainage Through the tooth Trephination – Apical / Cortical Incision and drainage
 Local use of the correct intra-canal medication 2) Systemic Analgesics")
• Medication 1) Local use of the correct intra-canal medication 2) Systemic Analgesics - mild pain - Acetaminophen (Paracetamol) - severe pain – Narcotic Opiods Anti-inflammatory - NSAID - Steroid therapy Antibiotics - An understanding of the type of infection is essential - Indicated for systemic infection (e. g. malaise, fever, lymphadenopathy, swelling) - Oral vs. IM / IV

• Rest General - post operative “let down reflex” Occlusal - relieving the occlusion “The effect of occlusal reduction on pain after endodontic instrumentation. ” Rosenberg PA. et al. J Endod. 1998: 24: 492 -6.

Emergency management of Irreversible Pulpitis Correct diagnosis is essential – reversible/irreversible Adequate LA Endodontic therapy. : Pulpotomy / Pulpectomy (If possible establish lengths and debride canals to at least size 25 file) Dress tooth with 100% Odontopaste / Ledermix paste Temporise Reappoint 3 -4 weeks Post operative Care: Ibuprofen 400 -600 mg four hourly prn +/- Analgesics @ two hourly intervals

Emergency management of Acute Apical Periodontitis → can be associated with vital/non-vital tissue Procedure: Adequate LA Endodontic therapy. If possible establish lengths and debride canals to at least size 25 file Dress tooth with 50 : 50 medication / Ca. OH 2 Temporise Reappoint 3 -4 weeks N. B. ensure all instruments are confined to the pulp canals and establish lengths Post operative Care: - Ibuprofen 400 -600 mg four hourly prn +/- Analgesics @ two hourly intervals - Antibiotics?


Pharmacology of Local Anaesthetics The efficacy of LA solution depends on the balance between the ionised (acid) and un-ionised (base) form. In the dental cartridge - most exists in the ionised form → longer shelf life In the tissues - the local p. H of the tissues and the drug’s strength as an acid (its p. Ka) regulate the distribution of the LA between the acid & base forms

Hypotheses for LA failure Effect of inflammation on local tissue: tissue → causes a drop in p. H in the immediate area (approx 6. 0) “tissue acidosis” → “ion trapping” (i. e a greater proportion of LA is caught in ionised form and therefore unable to cross the cell membrane) → LA solutions with a lower p. Ka value are relatively resistant to ion trapping Over come by use of LA solutions with lower p. Ka values e. g. mepivacaine

Hypotheses for LA failure Effect of inflammation on blood flow: flow Inflammation causes localised vaso-dilation → increased rate of systemic absorption of the LA More applicable for failure following infiltration Overcome by use of single / multiple vasoconstrictors in LA OR increasing the volume of solution

Hypotheses for LA failure Effect of Inflammation on Nociceptors: Nociceptors Substances released from inflamed tissue have 2 effects on nociceptive neurons 1. Prostaglandins Sensitize neurons e. g. “throbbing” pulpal pain caused by sensitized pulp nociceptors firing in response to the patients heartbeat 2. Inflammatory Growth Factors alter the structural properties e. g. nerve sprouting increases the size of the receptive field Overcome by increasing the volume of LA to be administered

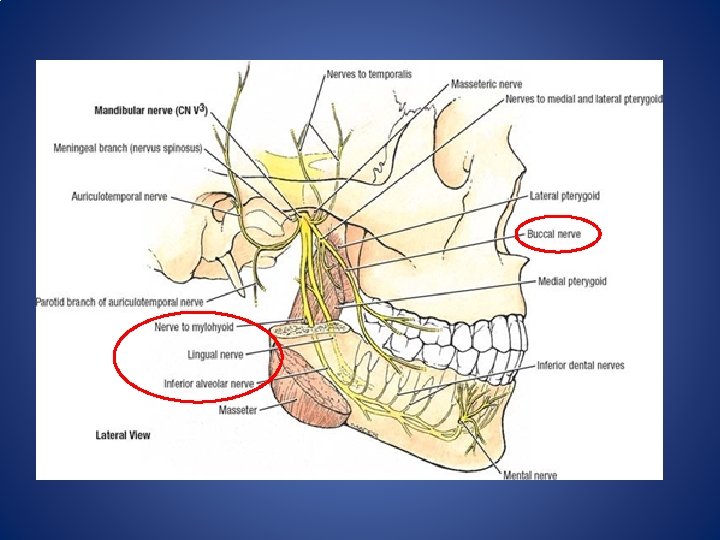
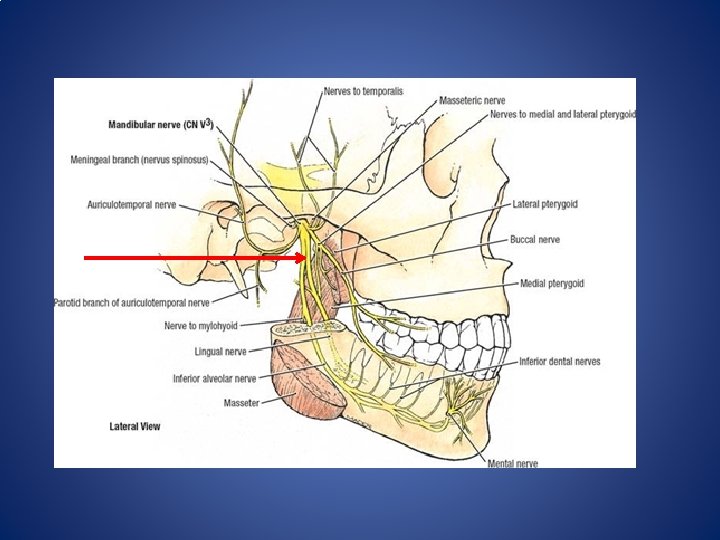
Hypotheses for LA failure Anatomical Causes: erratic distribution of LA within pterygomandibular space accessory innervation Mylohyoid nerve Lingual nerve Buccal nerve Transverse Cervical nerve Over come by use of Gow Gates technique / Akinosi Technique OR a high IAN block

V nerve - Sensory Root Three branches which supply the skin of the entire face and the mucosa of the oral cavity. 1) Opthalmic Div. – exits through the superior orbital fissure into the orbit 2) Maxillary Div. – exits through Foramen Rotundum into the pterygopalatine fossa and emerges onto the surface of the face through the infraorbital foramen. - Post. Sup. Alv. n. divides in the pterygopalatine fossa - Mid. & Ant. Sup. Alv nerves divide in the infraorbital canal 3) Mandibular Div. – Anterior division – motor and sensory (buccal nerve distribution). Branches at the level of the lateral pterygoid m. - Posterior division – sensory and motor (to mylohyoid m. )
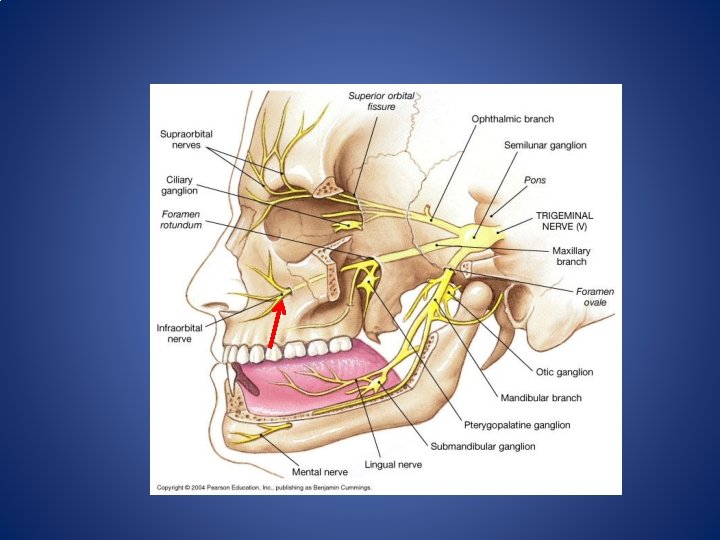

V nerve - Sensory Root Three branches which supply the skin of the entire face and the mucosa of the oral cavity. 1) Opthalmic Div. – exits through the superior orbital fissure into the orbit 2) Maxillary Div. – exits through Foramen Rotundum into the pterygopalatine fossa and emerges onto the surface of the face through the infraorbital foramen. - Post. Sup. Alv. n. divides in the pterygopalatine fossa - Mid. & Ant. Sup. Alv nerves divide in the infraorbital canal 3) Mandibular Div. – Anterior division – motor and sensory (buccal nerve distribution). Branches at the level of the lateral pterygoid m. - Posterior division – sensory and motor (to mylohyoid m. )

Local Anaesthesia Techniques Local infiltration Inferior Alveolar Nerve block Gow Gates Block Akinosi Technique Periodontal ligament injection Intrapulpal injection Intraosseus injection
 Low")
Gow Gates Nerve Block Advantages: Advantages Very high success rate (upward of 95%) Low incidence of positive aspiration Low incidence of accessory innervation being an issue Disadvantages: Time of onset is longer due to size of nerve trunk being anaesthetised Learning curve is longer

Gow Gates nerve block Target area - the neck of the condyle IAN Block GG Block

Gow Gates Nerve Block Extra Oral: Align the needle with the plane extending from the corner of the mouth to the intertragic notch on the side of the injection Intra Oral: Aim just distal to the palatal cusp of the upper second molar Insert the needle slowly and advance until bone is contacted (average depth = 25 mm). Withdraw the needle 1 mm and aspirate Deposit the LA solution Ask the patient to remain open for approximately 20 secs.


Gow Gates Nerve Block Palpate the coronoid notch or the anterior border of the ramus as high as possible. Extra Oral: Align the needle with the plane extending from the corner of the mouth to the intertragic notch on the side of the injection Intra Oral: Aim just distal to the palatal cusp of the upper second molar Insert the needle slowly and advance until bone is contacted (average depth = 25 mm). Withdraw the needle 1 mm and aspirate Deposit the LA solution Ask the patient to remain open for approximately 20 secs.

 Anti-inflammatory -")
Use of Intra-canal Medicaments Odontopaste / Ledermix Paste Mode of Action: 1) Anti-inflammatory - only effective for post operative pain in cases involving vital tissue. Ineffective in cases of chronic infection or necrosis - capable of decreasing periapical inflammation Barker BCW. & Lockett BC. (1971)

Ledermix paste - Diffusion: Diffusion Abbott P et al Endod. Dent. Traumatol. 1988, 1989 Initially: Rapid release Then: Slow, steady release Rate of Release 1 day 1 week 1 month 3 months

Ledermix paste - Diffusion: Triamcinolone Measured peri-radicular and apical concentration Detected in nanomolar range Sufficient for anti-inflammatory action Abbott et al EDT 1988, 1989 Measured concentration outside the tooth - too low to have any systemic effect Abbott P. IEJ 1992
2 Effect on Ledermix: → triamcinolone - ↓ anti-inflammatory effect -")
Combined Ledermix : Ca(OH)2 Effect on Ledermix: → triamcinolone - ↓ anti-inflammatory effect - prolonged release → demechlocycline - prolonged release - no effect on antibacterial properties Effect on Ca(OH)2: → no ↓ in p. H in radicular dentine → same antibacterial spectrum → no influence on diffusion characteristics

Pain Medication NSAIDS Incl. - COX-2 inhibitors - Paracetomol Opioids Steroids

Non-narcotic Analgesics When tissues are damaged arachidonic acids are released from the phospholipids component of the cell membrane → acted upon by cyclo-oxygenase to form PG, s. → act on peripheral pain receptors to produce a state of hyperalgesia. They act by interfering with the cyclo-oxygenase system and inhibit PG synthesis eg. Ibuprofen, Diclofenac, Celebrex, Paracetomol - well absorbed in the gut - metabolized in the liver, excreted thru the kidneys - 400 mg of ibuprofen is more effective than upto 60 mg of codeine - adverse effects – GIT irritation → avoid if peptic ulcer, pregnancy, asthmatics - dosage = 400 – 600 mg ibuprofen every 4 -6 hrs. + 1000 mg paracetomol

Narcotic Analgesics Primarily affect the CNS. Effectiveness is greatly reduced given orally because absorption thru the gut results in a first pass thru the liver where 50% are metabolised before reaching the CNS. Common side effects are vomiting, nausea, dizziness, respiratory depression e. g. Codeine, Tramadol, Endone A major component of post-endodontic pain is inflammatory in nature. Narcotics → poor efficacy c. f. anti-inflammatory analgesics. Drug interactions: Alcohol – causes increased CNS and respiratory depression. Dosage: maximum analgesic effect is obtained with 60 mg. Repeat every 4 -6 hrs.

Steroids The adrenal cortex synthesises corticosteroids from cholesterol. Two types: glucocorticoids and minerocorticoids. Glucocorticoids – act at multiple sites to inhibit inflammation and immune reactions. Chemical modification of cortisol has produced a number of synthetic corticosteroids that have a longer half life and greater anti-inflammatory properties. eg Prednisalone, Triamcinalone, Dexamethasone • Contraindications: Systemic fungal infections, known sensitivity to the drug, ulcerative colitis, diverticulitis, pregnancy, renal insufficiency, peptic ulcer, diabetes mellitus, osteoporosis, history of tuberculosis, acute psychosis. Dosage: Prednisalone 25 mg / day for 3 days

Infection

Emergency management of the Acute Apical Abscess → Caused by infected root canal system Procedure: Adequate LA Endodontic therapy. If possible establish lengths and debride canals to at least size 25 file If tooth is draining – let it drain! Dry canals Dress tooth with 50: 50 dressing / Ca. OH 2 Temporise. Reappoint 3 -4 weeks N. B. Often the tooth requires draining again. Do not leave the tooth open – this will not prevent the need to redrain!
 As an antibacterial (OH-")
Use of Intra-canal Medicaments Calcium Hydroxide Mode of Action: 1) As an antibacterial (OH- ions) → Damage to the bacterial cytoplasmic cell membrane → Protein denaturation → Damage to the DNA 2) As a stimulator of hard tissue formation (Ca 2+ ions) → High p. H → activation of alkaline phosphatase → inhibition of acid phosphatase →Ca 2+ ions → directly stimulate activation of ATP required for hard tissue formation

Diffusion properties • Hydroxyl ions are able to diffuse through radicular dentine • Limit by - buffering capacity of dentine - diameter of dentine tubules - cementum • Most bacteria killed @p. H = 9. 0 – 9. 5 • • One week for Ca(OH)2 to reach outer surface 2 -3 weeks for Ca(OH)2 to reach peak conc. on outer surface • More rapid in coronal one third Nerwich et al. JOE 1993; 19: 302 -6 Picture – micro paper and p. H values (summary 10. 8 @ 1 -2 hrs → 9. 7 @ 1→ -2 hrs 9. 26 @ ← 2 -3 wks ← 9. 0@ 2 -3 wks

Time of use of Medicaments • Minimum interappointment period: 2 weeks • Ideal interappointment period: 3 -4 weeks • Maximum interappointment period: dependent on the medicament used → 100% Ledermix paste = 6 – 8 weeks → 50: 50 combination = 3 – 4 months → 100% Calcium hydroxide = 3 – 5 months

Antibiotic Therapy – used to supplement not to replace. Indications: correct type of infection signs of the infection spreading systemic involvement/systems (e. g. malaise, fever, lymphadenopathy, swelling) immuno-compromised / immuno-suppressed Contraindications: no systemic involvement chronic alveolar infections inflammatory pulp conditions acute infections with adequate drainage
: Procaine Penicillin (Pen G) 600")
Recommended regimens for antibiotic therapy Injection of antibiotics (IM): Procaine Penicillin (Pen G) 600 mg 4 hrly Oral Administration: Phenoxymethyl Penicillin (Pen V) 1 g stat. & 500 mg qid Clindamycin 300 mg stat & 150 mg tds Metronidazole 400 mg tds N. B. Amoxycillin - used routinely (500 mg tds) - has a very broad spectrum with increased potential for resistance - better compliance

Space Infections Canine Fossa Infraorbital Space Buccal Space Submandibular Space Submental Space Sublingual Space

Canine Fossa Infection

Infraorbital Space Infection

Buccal Space Infection

Submandibular Space Infection

Intraoral and Submental Space

Ludwig’s Angina A life-threatening cellulitis that can advance into the pharyngeal and cervical spaces resulting in airway obstruction

Ludwig’s Angina Sublingual Space Submandibular Space Submental Space

Drainage Through the tooth Through the soft tissue Through the bone

Drainage through the tooth Apical trephination - placement of a size 10/15 file through the apical foramen

Incision and Drainage Through the Soft Tissue

Drainage through the bone Cortical trephination - small incision through soft tissue adjacent apex of involved tooth - #2 round bur through the cortical plate - #25 file to apex of tooth → “creating a sinus tract”

Prevention of Emergency Visits a. k. a. “Rules of Disengagement” Talk about expectations Consider creating artificial drainage Reassure patients of your availability Provide appropriate prescriptions Schedule follow-up visits Know when to cut your losses
- Slides: 54