Endocrinology Acromegaly Acromegaly Very rare Prevalence in the




,")



- Slides: 11
Endocrinology Acromegaly
Acromegaly �Very rare �Prevalence in the order of 1 in 200, 000 �Usually diagnosed between age 40 and 60 �No difference in gender susceptibility �Insidious onset
Pathogenesis �Most commonly caused by pituitary adenoma Ø Increased secretion of growth hormone Ø Acts in liver to release IGF-1 (insulin-like growth factor)
So what are the symptoms? �Tumour �Growth hormone �IGF-1
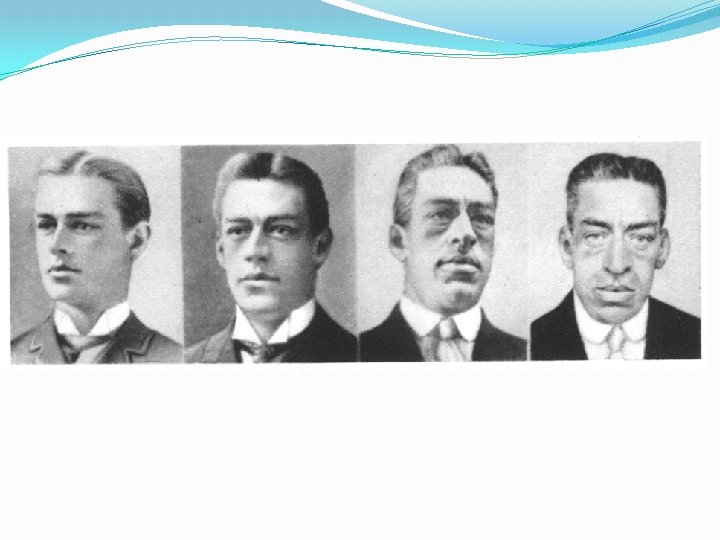
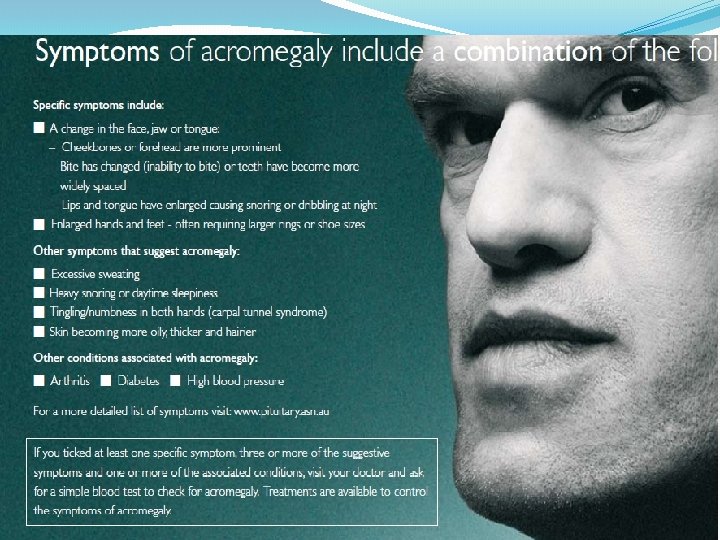
On examination �Characteristic facial appearance: Coarse, Frontal bossing, ↑sinuses, ↑ tongue, Prognathism (jaw protrusion), separation of teeth �Deep voice �Carpal tunnel syndrome �Hand & foot enlargement �Visual fields (bitemporal hemianopia) �Organomegaly: Goitre, Hepatosplenomegaly
Investigations �Glucose tolerance test with measurement of growth hormone level. Ø (Should be inhibited by glucose) Ø (Growth hormone secretion is episodic and so a random GH alone is unlikely to be useful) �Evidence of other pituitary involvement �MRI scan to identify adenoma
Management � Surgery: trans-sphenoidal adenomectomy or craniotomy for very large tumours. � Pituitary radiotherapy: useful if tumour is not fully removed and reduces GH progressively over years. � Drugs: Ø Somatostatin analogues (octreotide, lanreotide) suppress GH in 60% Ø Dopamine agonists (bromocriptine, cabergoline) lower but rarely normalize GH Ø GH receptor antagonist (pegvisomant) normalizes IGF-I in >90% of pts.
Bonus marks management Management of: �↑ Cardiovascular morbidity & mortality – from HTN, impaired GTT (25%), Diabetes Mellitus (10%) �↑ Cardiac failure (heart muscle disease), ↑IHD, ↑CVD �Obstructive sleep apnoea �Arthropathy (50%) �Osteoporosis �Colorectal cancer Complication of treatment: hypopituitarism