Endocrine System Collection of small glands and organs


 Endocrine System (indirect) Uses: electrical impulses Uses: hormones that travel through")


")



 The more receptors a cell")








")
stimulates adrenal cortex to release")




 that prevents")

 – works together w/ • Thyroxine (T")





")















- Slides: 66
Endocrine System
• Collection of small glands and organs that directly or indirectly influences the functions of the body • Some of the glands are also part of the nervous system (hypothalamus, adrenal and pineal) • This overlap allows the system of integrate their responses to our body’s needs
Nervous System (direct) Endocrine System (indirect) Uses: electrical impulses Uses: hormones that travel through blood Controls: muscles & some glands Controls: tissues (homeostasis) Feedback: quick Feedback: seconds Example: texting/emailing a friend…. . Example: mailing a letter months
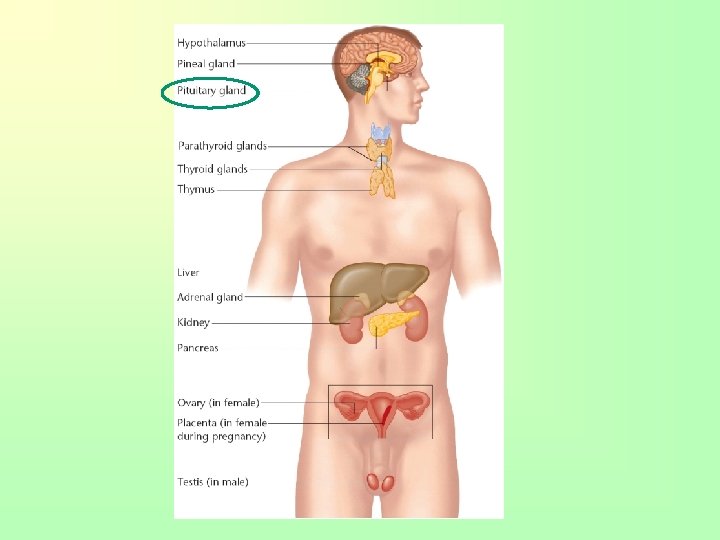
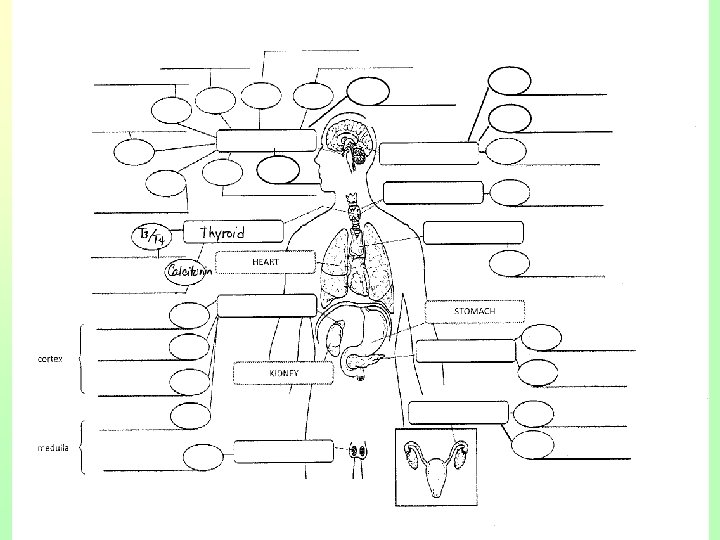
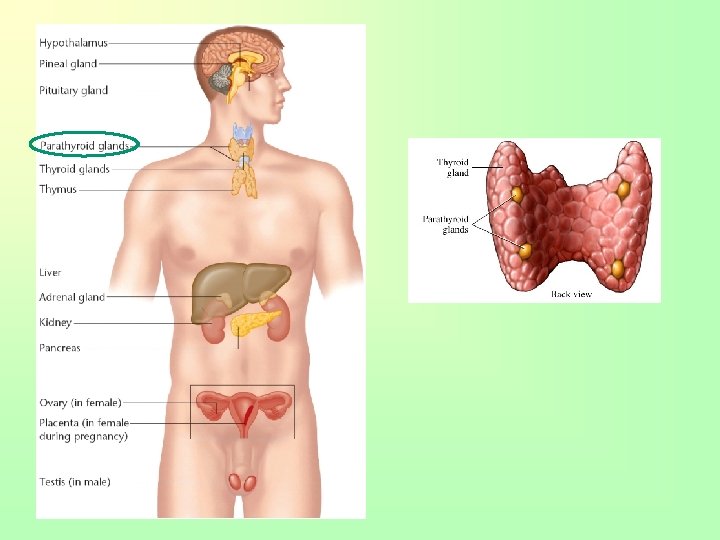
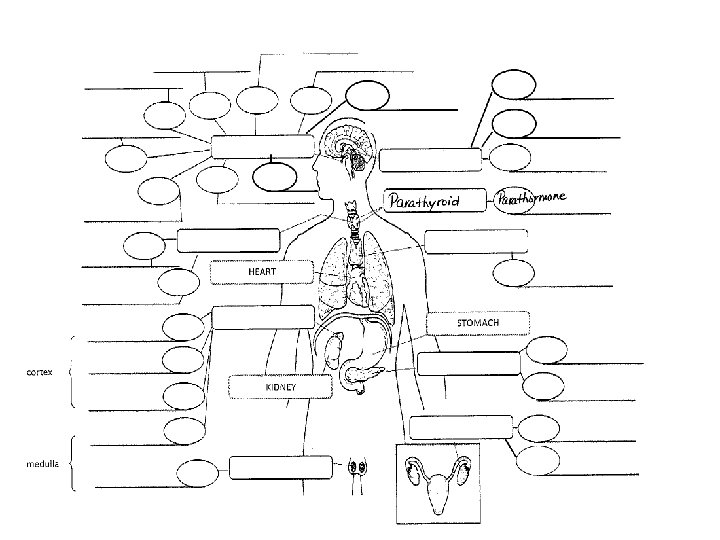
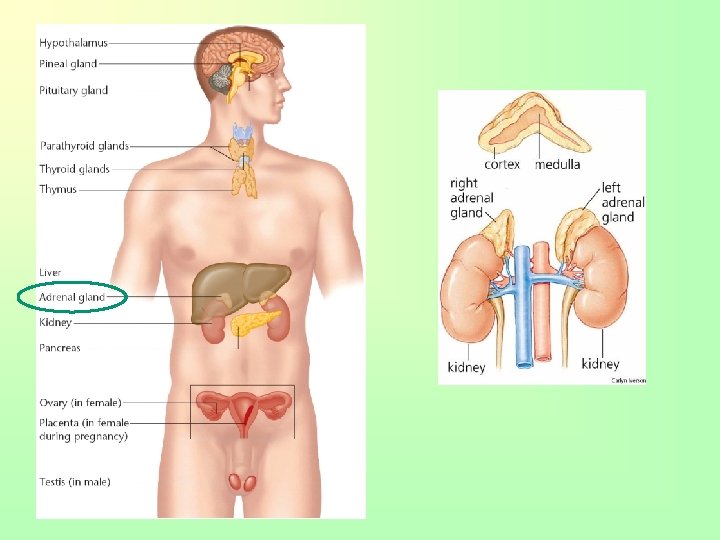
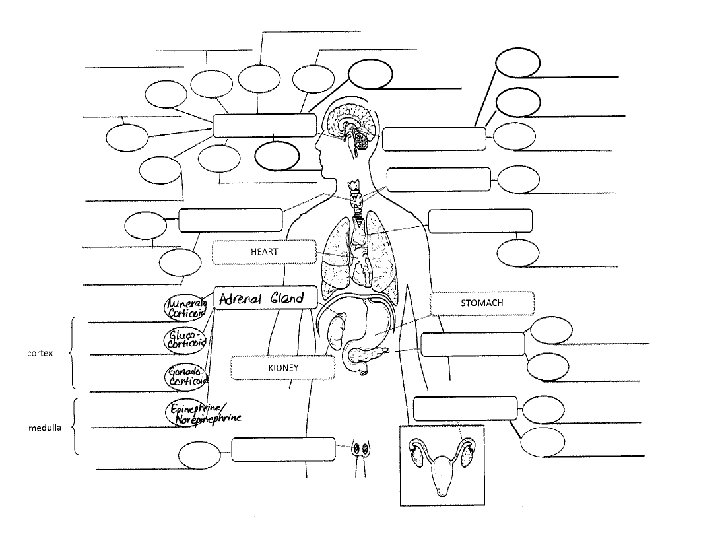
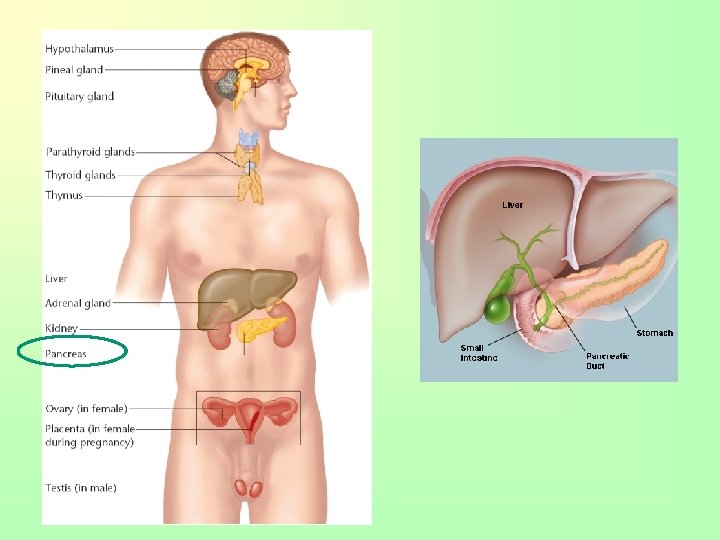
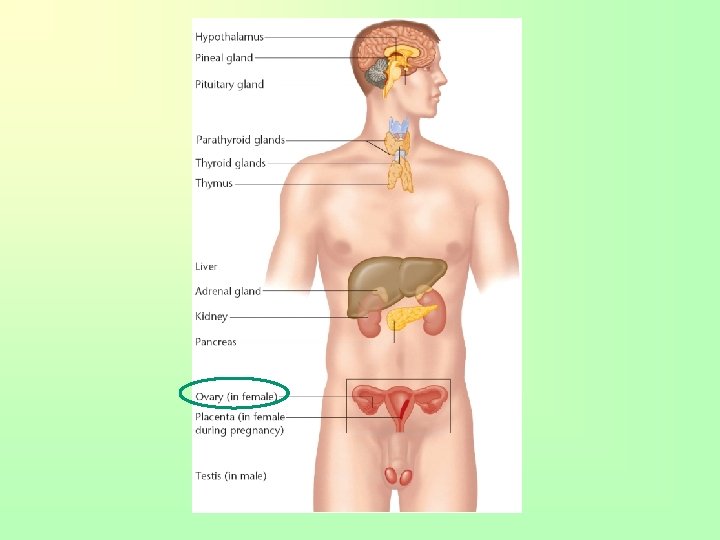
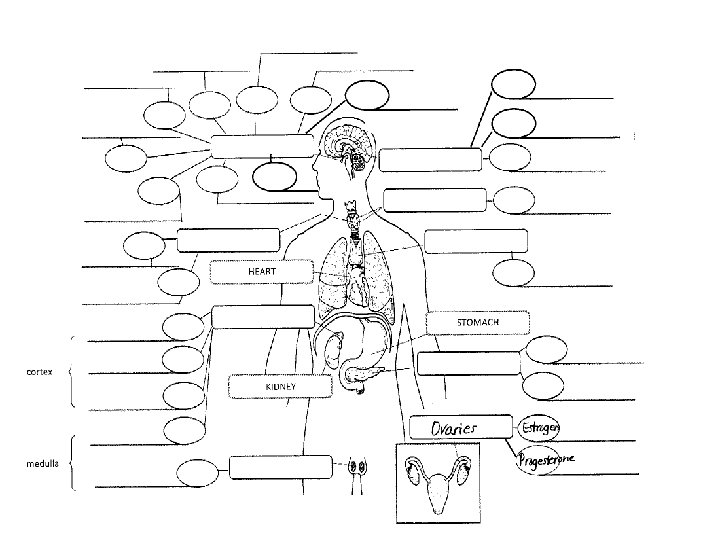
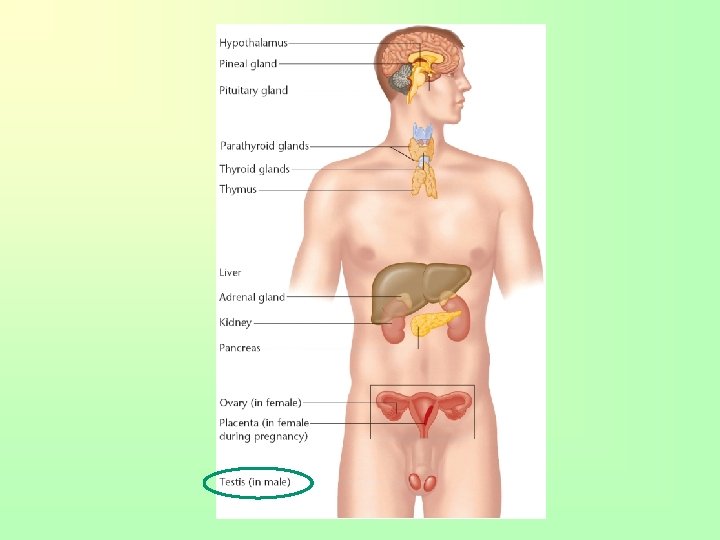
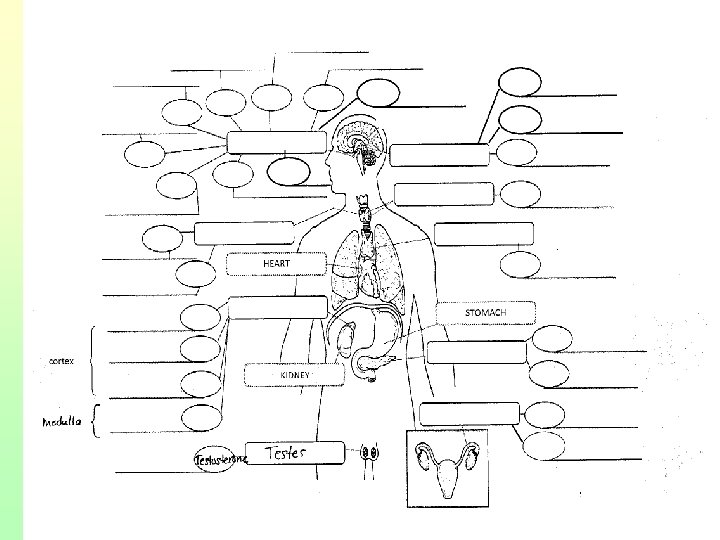
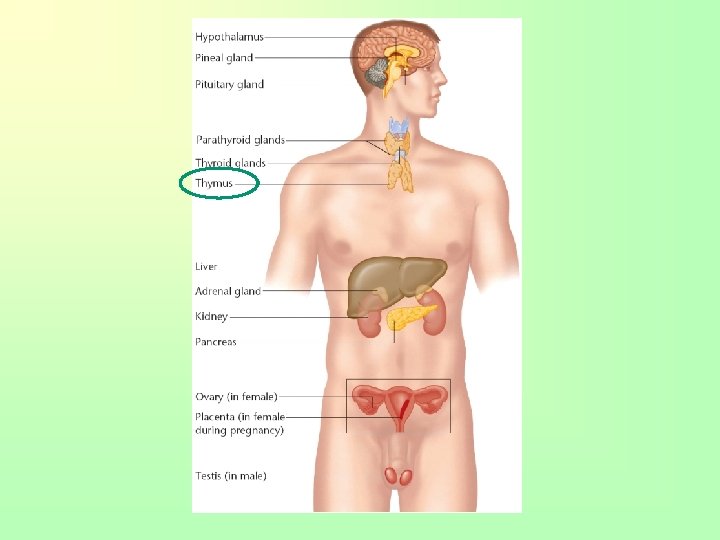
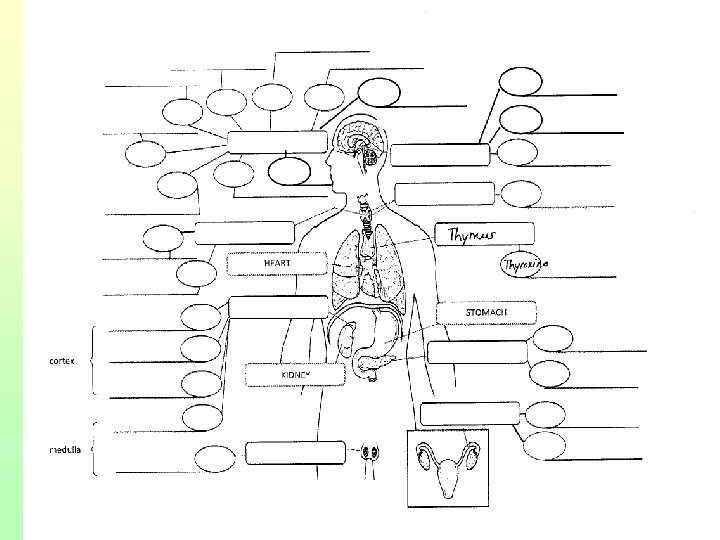
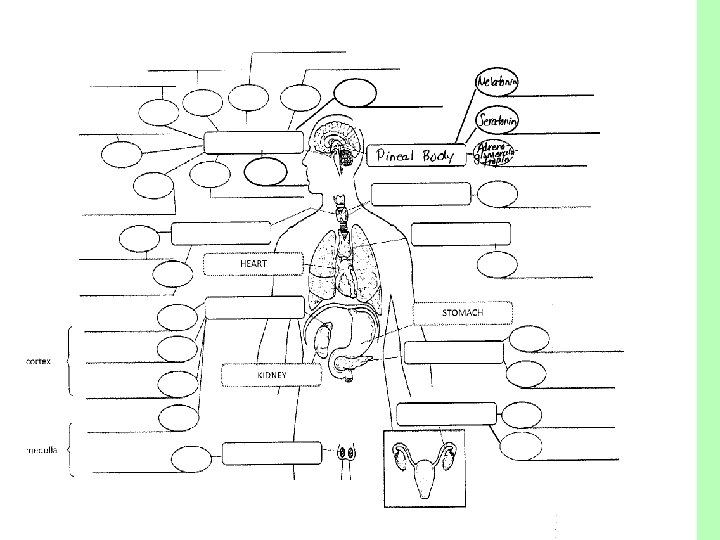
Functions • To secrete hormones “chemical messengers” that coordinate and direct activities of target cells and target organs • Transported throughout the body by the bloodstream performing certain functions and stimulating other • • Major glands Pituitary Pineal body Thyroid Parathyroid Thymus Adrenals Pancreas Gonads (ovaries/testes)
MAKE-UP OF GLANDS
Endocrine glands • Referred to “ductless glands” because they don’t secrete their product (hormone) outside of itself through a tube or duct • These glands make their product (hormone) and the capillaries come into (endo-) the gland pick it up • Tube/duct is NOT needed – Only exception is the pancreas
Hormones: “chemical messengers” affected by - Targets Types Actions Timing • Blood levels • Receptor numbers • Bonding strength • Amino acid • Steroid • Prostaglandin • Permeability • Synthesis of protein • Enzyme activity • Secretory activity • Onset and duration of activitation Release control • Hormonal • Humoral • Neural
Hormones & their target • Hormones travel through blood and lymph “bumping” into cells • When they find the cell/tissue they have a message for, they “fit” into the receptor of that cell – (target cell) – Think of it as trying multiple keys on a lock to try and unlock it • A target cell has the specific receptor for that hormone. This ensures that the hormone “talks” to the right cell/tissue
• How well the hormone finds the target and binds with it, depends on 3 factors: 1. Level of hormone in the blood a) If hormone level is too low, cells can’t produce or make changes to the level needed b) If hormones level is too high, cells work too hard and cause too much of a change which can cause problems with the body
2. Number of receptors in/on the target cell a) The more receptors a cell has can improve its chances of the hormone binding to it. b) Cells can change, increase or decrease, number or receptors needed to make it more or less sensitive to hormones 3. The strength of the bond between the receptor and hormone a) The shape of the hormone must fit the receiving shape of the receptor in order to form a strong bond and initiate the message
Types of Hormones 1. Amino acid based – Made of proteins and are too large to fit into the cell so most use a carrier protein in the blood to help them find their way and then use a second message (helper inside the cell) to deliver the message 2. Steroid based – Made of cholesterol and are very small so move easily through the cell membrane. Once inside the cell they move to the nucleus or mitochondria where they bond to the receptor 3. Prostaglandin based – More for cell-to-cell communication
4 actions that hormones cause on target cells 1. Change the permeability of the membrane 2. Increase/decrease the synthesis of protein synthesis for repair/healing 3. Increase/decrease enzyme activity 4. Increase/decrease secretory activity
Timing • Onset and duration of hormone activation on target cells vary due to – Amount of hormone in blood – Heart rate – Blood pressure – Kidney/liver function – Intercellular enzyme levels • Hormones enter the blood stream and find their target cells, in mean time, kidneys/liver filter them out. The time the hormone remains in the blood is call “half life”. Some hormones last for less than 1 minute, some can last hours to days
Control • Hormones must be released when needed and removed when not needed. This is done through “negative feedback system” • Negative feedback occurs when there is a drop in hormone level which triggers a response to increase the amount of hormone in the blood • 3 mechanisms for hormone release:
1. Hormonal stimulation – Negative feedback system 2. Humoral stimulation – Detection of a specified level of hormone, electrolyte, water and sugar in the blood 3. Neural stimulation – Release of hormone due to motor neuron stimulation of gland. Fastest way for hormones to be stimulated but also least used • “Fight or flight”
Negative Feedback re: thyroid Blood levels of a hormone change Hormone raises the blood level rises which causes the hypothalamus to shut off Hypothalamus in brain gets the message Stimulating hormones goes to the gland to produce its hormone Hypothalamus responds by sending releasing hormone to the pituitary gland The pituitary gland responds by releasing a stimulating hormone
GLANDS AND THEIR HORMONES
Pituitary Gland • Tiny structure about the size of a grape at the base of the brain • Connected to the hypothalamus (“brain” of the brain – stimulates release of hormones from the pituitary gland) • Master Gland • Produces many hormones that affects other glands • Contains 2 lobes each producing its own hormones
Pituitary-hypothalamus interaction • Hormones of the anterior pituitary are controlled by releasing chemical (factors) produced by the hypothalamus • As hormones are needed, the hypothalamus releases a specific releasing factor for each hormone
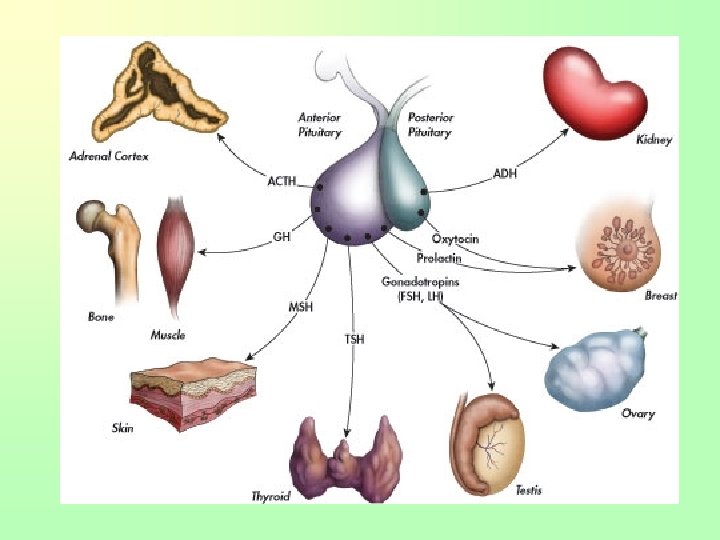
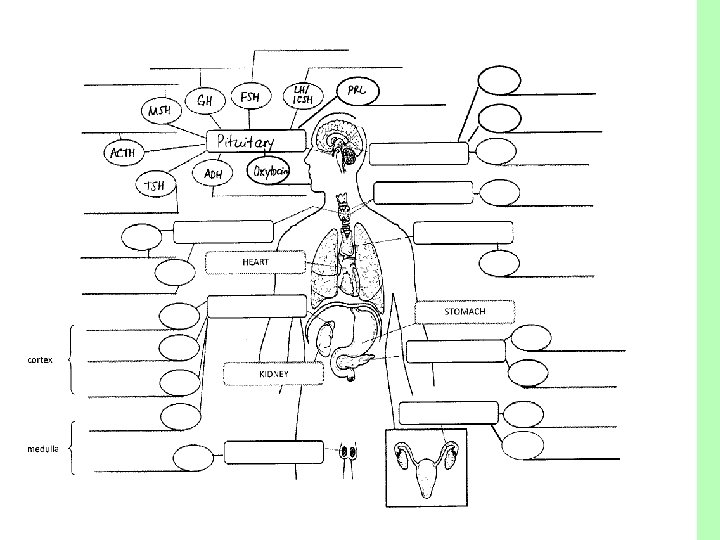
Hormones of the Pituitary ----Anterior Pituitary ---- • Adrenocorticotropic (ACTH)stimulates adrenal cortex to release cortisol and help resist stress • Somatotropin (GH)- growth hormone; affects all cells, growth plate and skeletal muscles • Melanocyte (MSH) production of melanin pigment in the skin to protect from UV rays • Thyrotropin (TSH)- stimulates growth of the thyroid gland • Follicle stimulating (FSH) – stimulation of egg and sperm formation; helps with release of estrogen and testosterone • Luteinizing (LH) – stimulates ovulation and produces progesterone in females; Interstitial Cell Stimulating Hormone (ICSH) - name used in males – stimulates testosterone production in males • Prolactin (PRL) - develops breast tissue & secretion of milk from mammary glands; in males enhances effects of ICSH ----- Posterior Pituitary---- • Oxytocin (pitocin) – released during childbirth; causes contraction of the uterus during childbirth • Vasopressin/antidiuretic (ADH) – instructs kidneys to pull water out and place it into the blood
Diseases of Pituitary
Gigantism • Over-secretion of growth hormone prior to puberty. • Excessive growth of long bones • Treatment: drug therapy to inhibit GH release
Acromegaly • Over-secretion of growth hormone during adulthood • usually from tumor • Enlargement of the extremities and/or face • Treatment: drug therapy to inhibit GH release
Dwarfism • Under-production of growth hormone during childhood • Long bone growth is decreased • Body is proportioned and intelligence is normal • Treatment: early diagnosis & injections of GH for 5 or more yrs.
• Diabetes insipidus – Decreased secretion of antidiuretic hormone (posterior lobe) that prevents water from being absorbed in blood leading to an excessive amount of water and electrolyte loss in urine
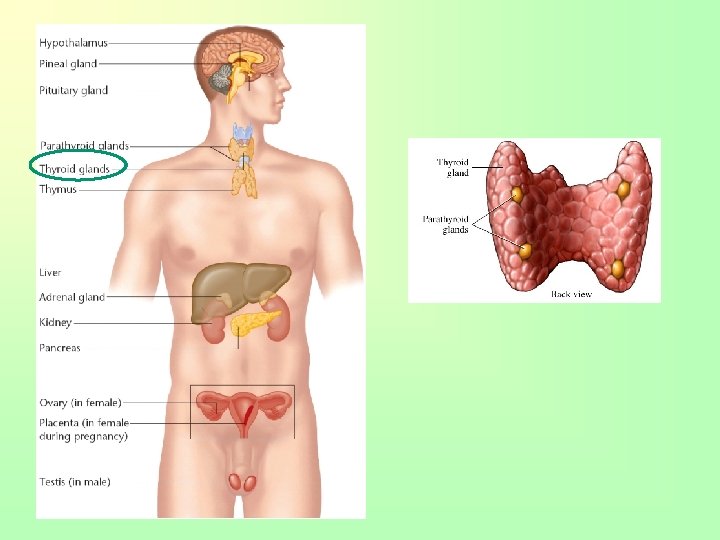
Thyroid Gland • Butterfly shaped mass found in front of the trachea; shaped like an H • One of the largest endocrine glands • Requires iodine to produce its hormone which is found in foods and salt • The hormones produces by the thyroid gland are controlled by the TSH in the pituitary gland
Thyroid Gland Hormones • Triiodothyronin (T 3) – works together w/ • Thyroxine (T 4) – controls rate of body’s metabolism, how cells use glucose and oxygen to produce heat/energy; controls levels of calcium in the blood; stimulates physical and mental growth • Calcitonin – accelerates storage of calcium in bones and lowers blood calcium levels; 99% of calcium in the body is stored in bones, necessary for blood clotting, and holding cells together – Proper secretion prevent hypercalcemia in
Diseases of the Thyroid gland
Hyperthyroidism • Over-activity of thyroxin leading to enlargement of the gland • Consume large quantities of food, but loss of body fat and weight • Tx: total or partial removal of thyroid gland or radiation to suppress the activity
Grave’s disease • Severe form of hyperthyroidism • More common in women • Symptoms: strained and tense facial expression, exophthalmia, goiter, nervous irritability goiter exophthalmos
Hypothyroidism • Under-secretion of thyroxin; due to los T 3 & T 4 levels or high TSH levels • Adult hypothyroidism may be due to iodine deficiency • Major cause due to inflammation of the thyroid which destroys the ability of the gland to make thyroxine • Dry/itchy skin, dry/brittle hair, constipation, muscle cramps
Myxedema • Face becomes swollen, weight increases and memory begins to fail • Treatment is daily thyroid hormone • Follow-up tests to measure TSH blood levels are important Cretinism • Develops early in infancy or childhood • Lack of mental/physical growth resulting in mental retardation and malformation • Sexual development and physical growth does not reach beyond 7 -8 year old children • Normal development cannot be completely restored w/ tx.
Parathyroid Gland • Four small glands behind the thyroid (size of grains of rice) • Parathormone (PTH) Regulates calcium in blood and stimulates bone cells to break down bone tissue and release calcium/phosphates into the blood • Maintains proper levels of circulating calcium
Diseases of the Parathyroid gland
• Hyperparathyroidism – Over-activity of parathyroid resulting in increased calcium in the blood – Leads of kidney stones, GI disturbances – Bones become weak, deformed and fracture easily because calcium is drawn from the bone • Hypoparathyroidism – Under-activity of parathyroid gland causing a low level of calcium in blood – Tetany, hyperirritability of nervous system, twitching – Death can occur if the larynx and respiratory muscles are involved.
Adrenal Gland • “suprarenal” glands because found above each kidney • 2 parts: cortex (outer portion) & medulla (inner portion) • ACTH from the pituitary stimulates activity of the cortex • Cortex hormones known as corticoids – Very effective as anti-inflammatory drugs – classified in 3 catagories:
Adrenal Gland hormones Cortex • Mineralocorticoids which aid with absorption of sodium into the blood stream and the excretion of potassium from the blood stream; speeds up absorption of water in the kidneys • Glucocorticoids which aid in metabolism by increasing glucose in the blood; help body resist stress • Gonadocorticoids which reduce inflammatory responses and act as sex hormones stimulating male/female sexual Medulla • epinephrine & norepinephrine activates nervous system to act in stress & causing “flight or fight” syndrome
Diseases of the Adrenal glands
• Addison’s disease – Decreased function of adrenal cortex – Excessive pigmentation, low blood pressure when standing, muscular weakness/fatigue, diarrhea, wt. loss, vomiting – Tx. Replace – hormone • Cushing’s syndrome – Hypersecretion of glucocorticoids – Causes hyperglycemia, hypertension, poor wound healing, bruising, “moon” face and obesity
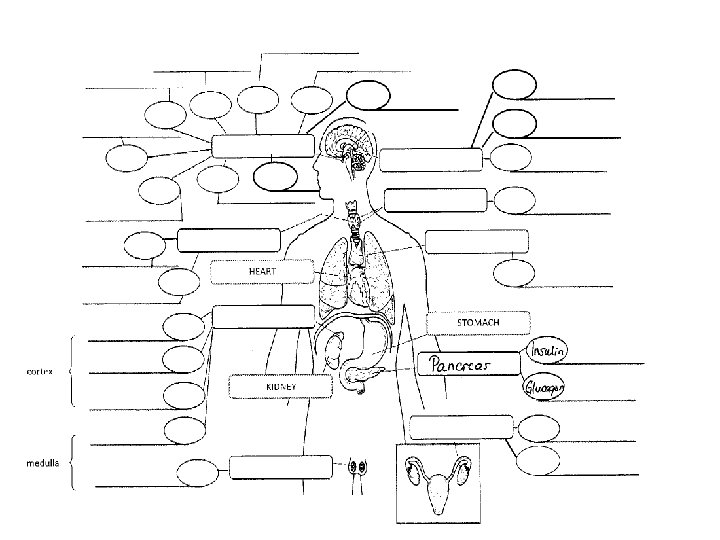
Pancreas • Fish-shaped organ behind stomach • Exocrine (secretes pancreatic juices that are carried to small intestines to aid in digestion) and endocrine gland (produces insulin needed for cells to absorb sugar from the blood)
Hormones of Pancreas Insulin Glucagon • Targets every cell in the body and promotes glucose uptake by cells • Glucose is used for cellular energy • Essential for providing lifesustaining energy • Maintain blood glucose levels • When glucose levels are low, glucagon is stimulated
Diseases of Pancreas • Diabetes mellitus – Decreased secretion of insulin w/ affects metabolism of carbs, proteins, fats – 2 types of D. M. • Type 1: juvenile onset; thought to be an autoimmune reaction involving genetic and virus factors that destroy parts of the pancreas – More severe, requires insulin injections • Type 2: adult onset; most common in adults over 45, overweight, heredity, certain ethnic groups – Frequently occurs in obese adults and may not be insulin dependent – Controlled w/ diet – Hyperglycemia, polyuria, polydipsia, polyphagia, glycosuria, weight loss, fatigue, slow healing of skin infections and vision changes
Ovaries • Female sex glands • Located behind pelvic cavity • Secretes hormones that regulate menstruation and secondary sexual characteristics
Hormones of Ovaries Estrogen Progesterone • promotes growth and development of sex organs in female • Assists in regulation of menstrual cycle and ovulation • maintains lining of the uterus for pregnancy • Assists (with estrogen) in regulating menstrual cycle and ovulation
Testes • Male sex gland • Located in scrotal sac and suspended outside the body • Testosterone regulates sexual characteristics of male
Thymus • Mass of tissue found under the sternum • “school for white blood cells” – where lymphocytes mature • Active in early life activating cells in the immune system • Atrophies during puberty • Produces only one hormone – thymosin which stimulates production of antibodies in early years
Pineal Body • Small structure attached to the third ventricle in the brain • Little known about the gland • Secreted 3 main hormones • Melatonin – regulates sleep/wake cycle; may delay puberty by inhibiting sex hormones • Adrenoglomerulotropin – stimulates adrenal cortex • Seratonin – prevent vasoconstriction of blood vessels in the brain
Placenta • Temporary endocrine gland produced only during childbirth • Estrogen – stimulates growth of reproductive organs • Human Chorionic gonadotropin – causes ovaries to continue secretions • Progesterone – maintains lining of uterus to provide fetal nutrition • Promotes milk production in breasts • Expelled after birth of child • “afterbirth”