Endocrine surgery from long incisions to minimally invasive

















 Ø Totally endoscopic techniques")






























- Slides: 65
Endocrine surgery from long incisions to minimally invasive surgery Nidal Younes MBBSc Professor of endocrine Surgery Secretary General JMC
How Uneducated Butchers and Barbers Became Today’s Skilled Surgeons
British surgeon Robert Liston and the 2 -3 min amputation
Morton Ether Inhaler at the Mass. General in 1847
June 17, 1867: Lister Cuts Clean, Saves Lives
The Nobel Prize in Physiology or Medicine 1909 was awarded to Theodor Kocher"for his work on the physiology, pathology and surgery of the thyroid gland
(September 18, 1889 — September 2, 1917
The first parathyroidectomy performed by Felix Mandel in 1925
Laparoscopic surgery Ø 1975 laparoscopic salpingectomy Ø 1970 -1980 gyneprocedures Ø 1981 Semm /Germany 1 st lap appendectomy Ø 1989 lap cholecystectomy
Surgery 101. up until the discovery of anesthesia Surgery 102. . 1847 - 1990 s traditional surgery Surgery 103 from 1990 s MIS
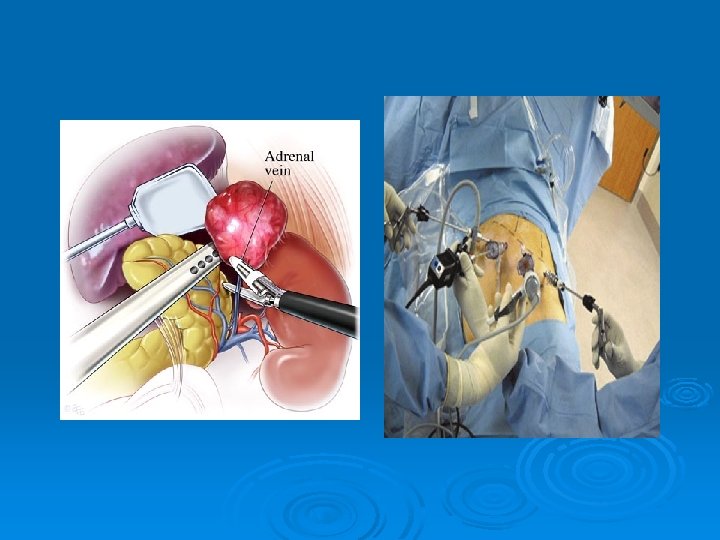
Scope of laparoscopic surgery Ø Cholecystectomy Ø Appendectomy Ø Adrenalectomy Ø Colectomy Ø Hernioplasty Ø Diagnostic Ø Hiatus Hernia repair Ø Bariatric surgery Ø Adhesiolysis
Advantages of Lap Surgery Ø Day care surgery Ø Shorter hospital stay Ø Improved cosmesis Ø Faster recovery Ø Minimal pain Ø Small scar Ø Better preservation of respiratory function
The Art of surgery Clinical judgment Knowledge Dexterity
Surgical management requires 1. localization 2. Access 3. Surg procedure
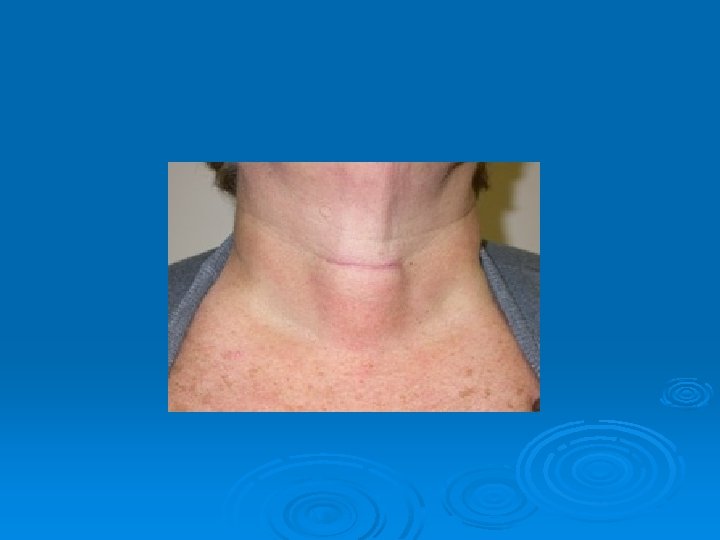
Minimally invasive thyroid surgery Ø Minimally invasive video-assisted thyroidectomy (MIVAT) Ø Totally endoscopic techniques that include an axillary approach, transcervical …
Outcome and prognosis Ø Better cosmesis Ø less postoperative pain and discomfort conventional thyroidectomy Ø shorter hospital stays.
Minimaly inavsive parathyroid surgery Ø Ø Ø Videoendoscopic- co 2 insufflations Videoendoscopic- gassless Videoassisted Radioguided Focused central mini incision Focused lateral mini incision
Targeted /minimally invasive surgery Ø Preoperative localizing techniques l U/S l CT l l l Sestamibi Spect CT MRI
Targeted Vs bilateral exploration RTCs comparing routine bilateral exploration vs limited exploration guided by IOPTH, show that bilateral exploration leads to the unnecessary removal of additional non-hypersecreting parathyroid glands Siperstein A, Prospective evaluation of sestamibi scan, ultrasonography, and rapid PTH to predict the success of limited exploration for sporadic primary hyperparathyroidism, Surgery 2004 Miccoli P, Endoscopic bilateral neck exploration versus quick intraoperativ e parathormone assay (q. PTHa) during endoscopic parathyroidectomy: A prospective randomized trial, Surgery 1999
Minimally invasive parathyroid surgery
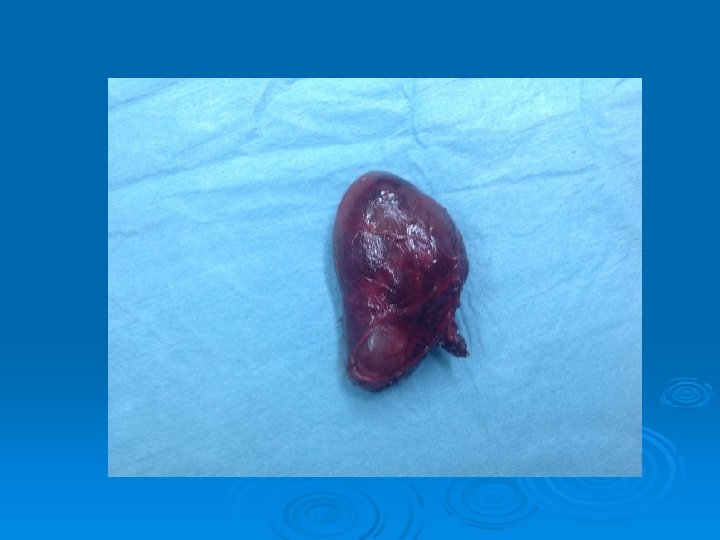
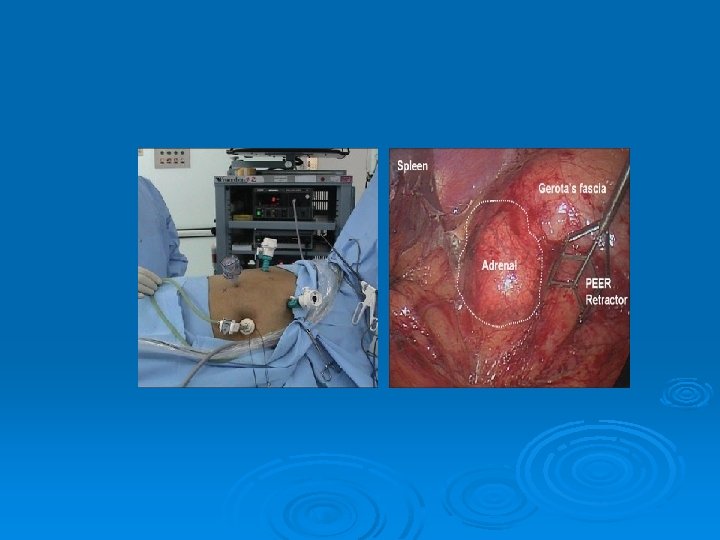
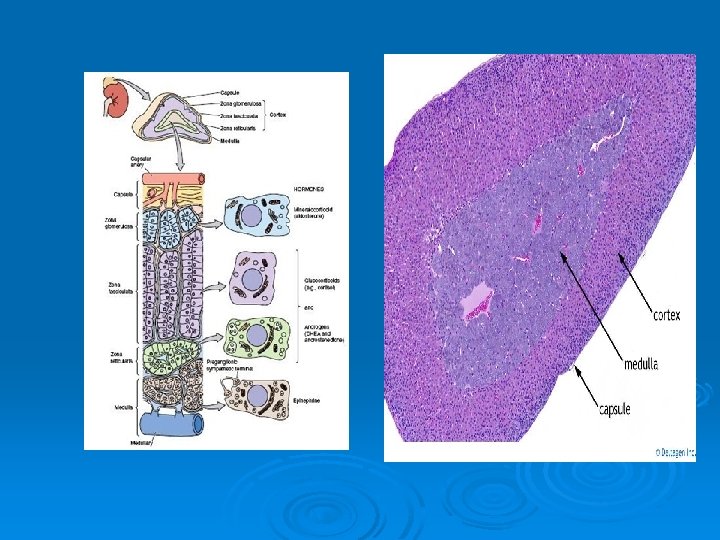
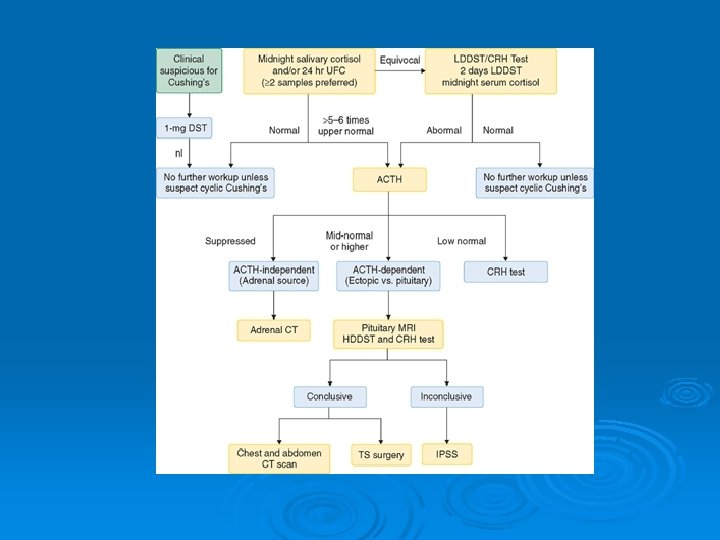
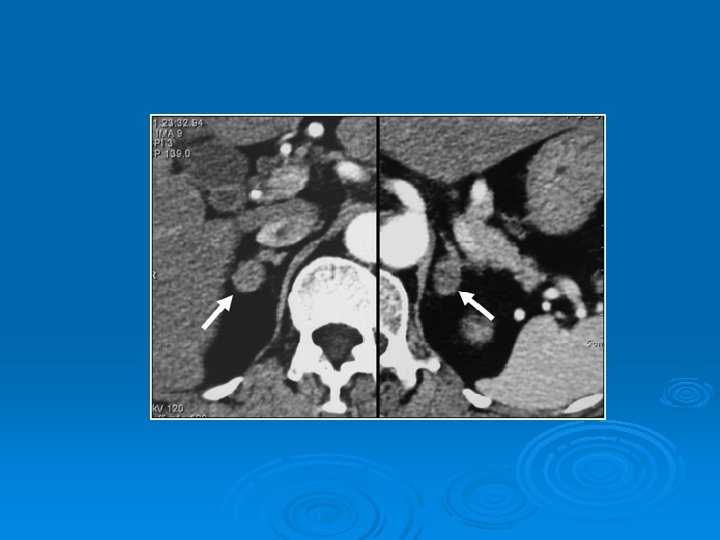
Indications for adrenalectomy Incidentalomas Ø Primary hyperaldosteronism Ø Cushing syndrome Ø Pheochromocytoma Ø Neuroblastoma Ø Adrenocortical carcinoma Ø During surgery for RCC Ø
DDx adrenal mass Cortical vs Medullary Ø Benign vs malignant Ø Functioning vs non functioning Ø Primary vs secondary Ø
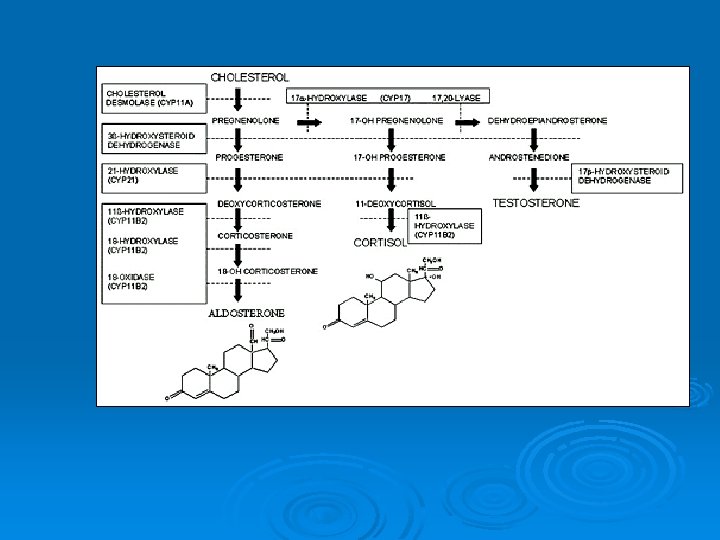
Adrenal tumors Ø Conn’s syndrome Ø Cushing's syndrome Ø Pheochromocytoma Ø Neuroblastoma 30% adrenal Ø Virilizing or feminizing syndromes Ø Myelolipoma Ø ACC (1 case per 1. 7 million)
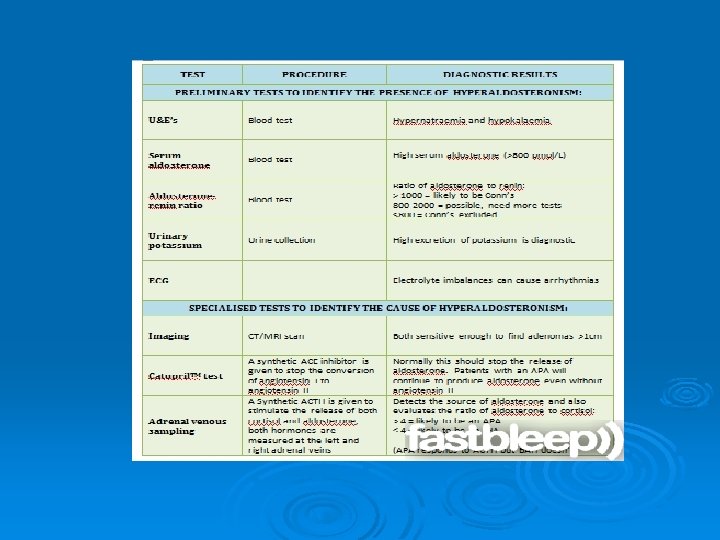
Conn’s syndrome ØA 25 y male presents to the clinic as a new patient. He takes no prescription medications, over-the-counter products or “alternative substances” Ø He came because his wife, a PA, noted hypertension and scheduled the visit Ø Lab results revealed K=2. 9
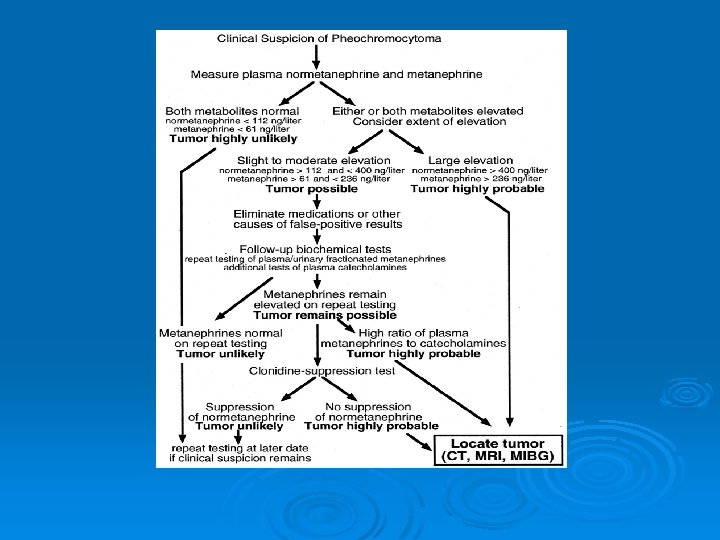
Pheochromocytoma
Adrenocortical carcinoma Ø Functioning l l Cushing's syndrome Conn’s syndrome Pheochromocytoma Virilizing or feminizing syndromes Ø Non Functioning
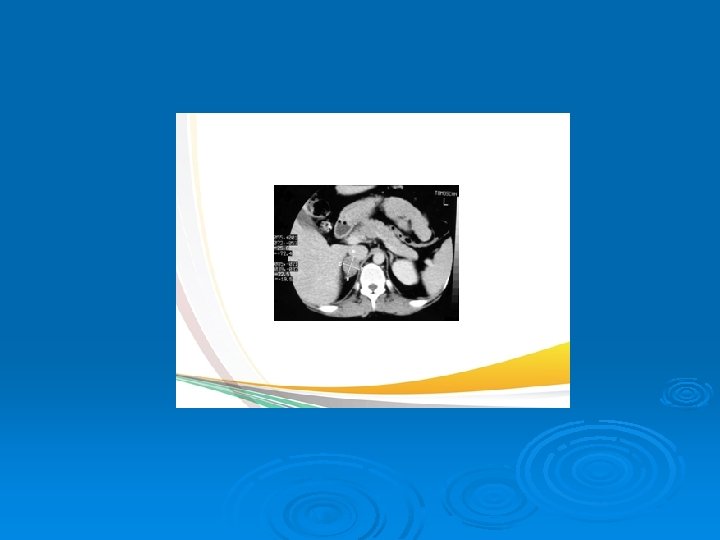
Adrenocortical tumors Ø Carcinomas are typically >18 units Hounsfield Ø In-phase/opposed-phase, MRIs. l l Ø benign lesions show a loss of signal intensity malignant lesions show no loss of signal Extra adrenal extension
ACC incidence is 1 in 1. 7 million. Ø Incidence of CA in incidentaloma 0%-25%. Ø Adrenocortical carcinomas are large with irregular borders on CT Ø By the time they are found, they are usually 12 cm in diameter. Ø Over 90% of adrenocortical carcinomas are >6 cm at presentation. Ø
Neck collar incision Ø Small incisions Ø Endoscopic Ø Robotic Ø Transaxillary incisions Ø Transoral incisons Ø
ROBOTIC SURGERY
Minicrab-like robots Minirobots
Nano. Robots
Transoral endoscopic thyroidectomy: A case report Vishwanath M. Pai et al International Journal of Surgery Case Reports Volume 12, 2015, Pages 99– 101
Surgery before anesthesia
Surgery after anesthesia
Operating Room with no People SRI International, Menlo Park, CA January, 2007