ENDOCRINE PANCREAS o Diabetes Mellitus o Islet Cell

ENDOCRINE PANCREAS

o Diabetes Mellitus o Islet Cell tumors

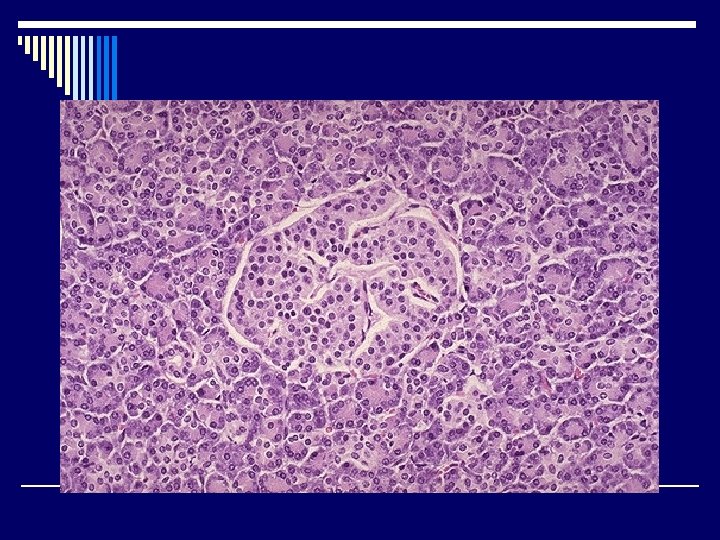
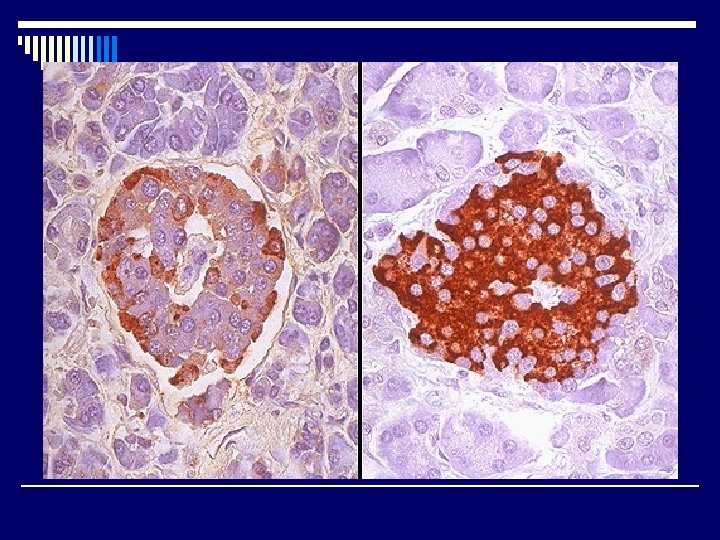
INTRODUCTION o One million islets of Langerhans o Several types of cells “Immunohistochemistery” n ß (beta) -> 70% insulin n А (alpha)-> 20% glucagons n D (delta) -> 5 -10% somatostatin n P. P Cell -> 1 -2% pancreatic polypeptide n Other rare cells: D 1 cells VIP ( vasoactive intestinal polypeptide ) Enterochromaffin cells 5 HT-(serotonin) - - -
")
o Each type of pancreatic islet cells may give mainly benign tumour -> (ADENOMA) called Islet cell tumours: Insulinoma Glucagonoma Somatostatinoma VIPoma Carcinoid tumours Gastrinoma n Multiple Endocrine Neoplasia (MEN)

DIABETES MELLITUS

DEFINITION o Diabetes Mellitus is a chronic disorder of carbohydrate, fat, and protein metabolism. o In which there is impaired glucose utilization due to defective or deficient insulin secretory response inducing hyperglycemia
 Diabetes Mellitus n Type-1 (Insulin Dependent Diabetes Mellitus) p Type-1")
CLASSIFICATION o Primary (idiopathic) Diabetes Mellitus n Type-1 (Insulin Dependent Diabetes Mellitus) p Type-1 A (immune mediated) p Type-1 B (idiopathic) n Type-2 (Non-insulin Dependent Diabetes Mellitus) p* Non-obese NIDDM p * Obese NIDDM p * Maturity onset diabetes of the young (MOD) p * Gestational DM

o Secondary Diabetes Mellitus: - Chronic pancreatitis p- Post pancreatectomy p- Hormonal tumours (acromegaly, Cushing’s ---) p- Drugs (corticosteroids) p- Haemochromatosis p- Genetic disorders e. g. lipodystrophy p- Gestational DM p

Primary Diabetes Mellitus is by far the most common in our countery and worldwide. Type 1 and type 2 have different pathogenetic and metabolic characeristics. Simillar long term comlications occur in both types.
: n n n Young Rare Linked to")
o MODY (maturity-onset DM of the Young): n n n Young Rare Linked to chrom. 7 & 20 Autosomal dominant Mild hyperglycemia

o ACUTE METABOLIC COMPLICATIONS:

Diabetic Ketoacidosis coma: n n In Type I Diabetes Mellitus Due to severe insulin deficiency with increase glucagons. Decrease insulin lipolysis free fatty acids Increase Glucagon oxidation of FFA in liver Ketoacidosis Coma
 Elderly Uncontroled")
Non ketotic Hyperosmolar Coma: n n n In Type II DM (NIDDM) Elderly Uncontroled DM Sustained hyperglycemic diuresis Severe dehydration coma Lack of symptoms (nausea, vomiting and respiratory difficulties) Delay the seeking of medical attention. o Hypoglycemia Coma

Morphology & Late Complications o Depends on : n n n - Duration - Metabolic control - Genetic factors

o Microangiopathy: Thickening of basement membrane PAS + Advanced glycosylation end product. n - Renal Glomeruli ( (nephropathy n - Retina ( (retinopathy n - Nerves (neuropathy)

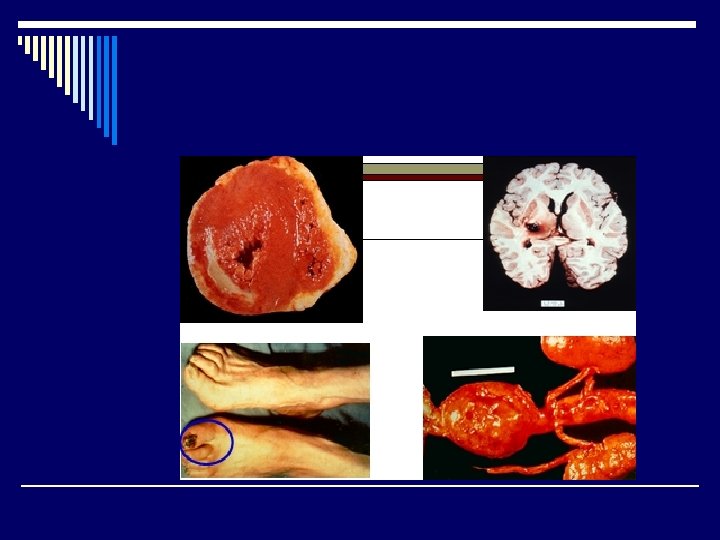
o Atherosclerosis: n n - Myocardial infarction Cerebral stroke. Aortic aneurysm. Gangrene of lower extremities

o Neuropathy: n n n - Symmetric peripheral neuropathy. - Sexual impotence. -Bowel and bladder dysfunction.

Diabetic Nephropathy Glomerular involvement : o 1. 2. Diffuse glomerulosclerosis. Nodular glomerulosclerosis “ Kimmel. Stiel – Wilson lesion ” Nephrotic Syndrome Arteriolosclerosis: Pyelonephritis (acute & chronic) o o n * Necrotizing papillitis.

Diabetic Ocular complications: o - Retinopathy : n Non – proliferative retinopathy ( hemorrhage, oedema, exudates microaneurysms and microangiopathy) n Proliferative retinopathy Neovascularization and fibrosis blindness (macula ) o - Vitrous hemorrhage. o - Cataract formation. o - Glaucoma *Diabetes Mellitus are more susceptible to infection.

ISLET CELL TUMOURS o Rare o Adult o Multiple / solitary o May be functional o Mainly benign / can be malignant
 of")
ISLET CELL TUMOURS Three Syndromes: 1. Hyperinsulinism & hypoglycemia : n n (insulinoma) of Beta cells solitary adenomas multiple Can be malignant
 n n - Multiple ulcer")
ISLET CELL TUMOURS 2. Zollinger – Ellison Syndrome (Gastrinoma) n n - Multiple ulcer disease - Gastric hypersecretion - Islet cell tumour Malignant 60% & benign 40% 3. MEN (1, 2 A, 2 B)
- Slides: 27