Endocrine disease Prepared by Siti Norhaiza Binti Hadzir

Endocrine disease Prepared by: Siti Norhaiza Binti Hadzir

Introduction • Endocrinology- the study of hormones, which are secreted from specialized glands into the blood to influence the activity of cells at distance sites in the body.
,")
Types of Hormones • • • Peptides or proteins- hypothalamic factor (thyrotrophin releasing hormones), and pituitary gonadotropin. Amino acid derivatives- e. g thyroid hormones and adrenaline Steroid hormones- derivatives from cholesterol (e. g estrogen)

Measurement of Hormones • • Radioimmunoassay Monoclonal antibodies

Endocrine Disease • • Described as over or under secretion of hormones Failure of hormones responsiveness

Oversecretion Cushing’s disease where a pituitary adenoma secretes ACTH Underscretion Primary hypothyroidism where thyroid gland is unable to make sufficient thyroid hormone despite continued stimulation by TSH Failure of hormone responsiveness Pseudohypoparathyroidism where pt become hypocalcemic despite elevated plasma PTH concentration because target organs lack a functioning receptor signaling mechanism Examples of Endocrine Disease

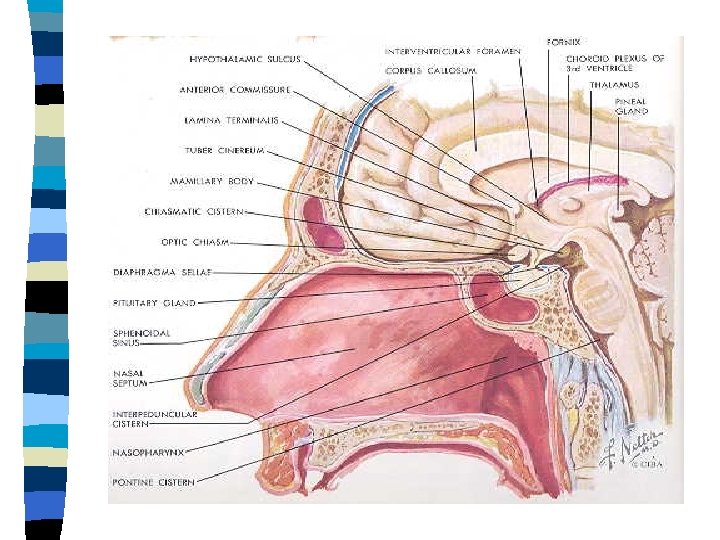
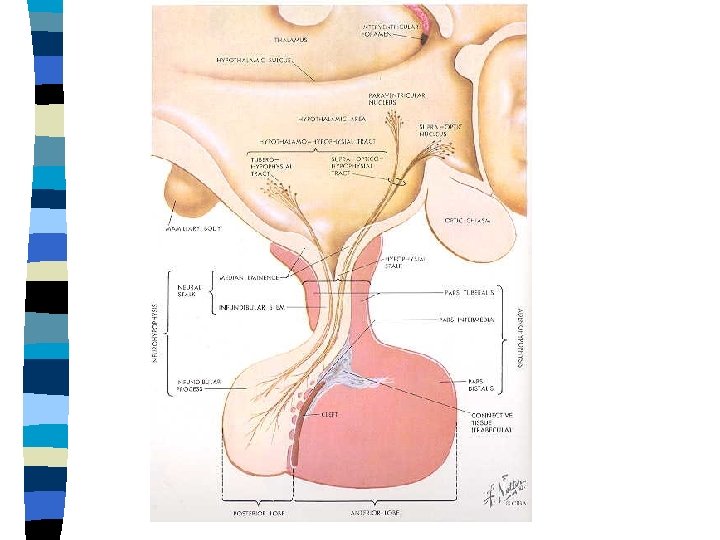
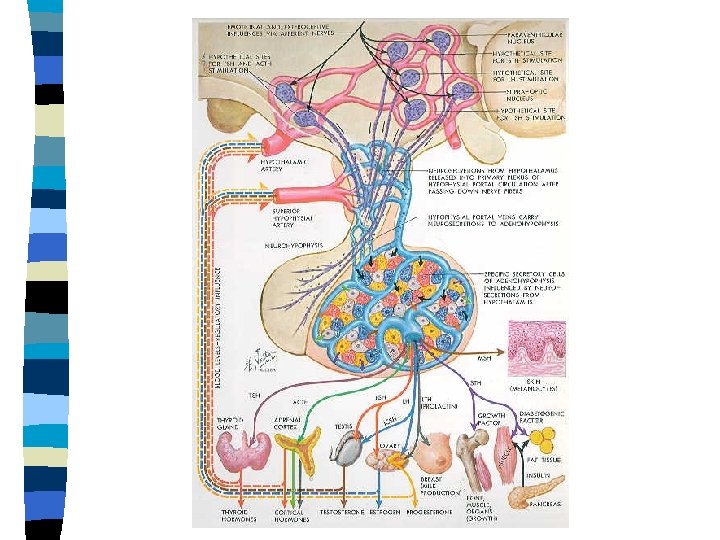
The Pituitary Gland • • • The location Anterior pituitary-hormone secreted Posterior pituitary-hormone secreted Hypersecretion-tumours (prolactin secreting adenoma the most common) Hypopituitarism-is uncommon; the clinical presentation depends on the age, sex or the person.
 rapid growth-1 st")
Growth disorders Growth in children can be divided into 3 i) rapid growth-1 st 2 years –condition in utero and nutrition ii) Steady growth-around 9 years-mainly controlled by GH iii) puberty- sex hormones and GH -Other hormones involve in growth •

Growth hormone insufficiency • • • Is a rare cause of impaired physical growth. Test of GH insufficiency: - serum GH in response to exercise, nocturnal sample - Stimulant (clonidine) Treatment: genetically engineered GH for children
. The condition is rare")
Excessive growth • • • Extremely rapid linear growth (gigantism). The condition is rare often due to pituitary tumor. Other causes; congenital adrenal hyperplasia, hyperthyroidism, inherited disorders. ↑GH later in life-Acromegaly due to pituitary adenoma

Diagnosis of Acromegaly • • OGTT- a normal person will suppress GH in plasma in response to glucose load. Acromegaly-not suppress ↑ IGF 1 Treatment-surgery, radiotherapy, drugs (octreotide-somastostatin analogue) and bromocriptine
 and")
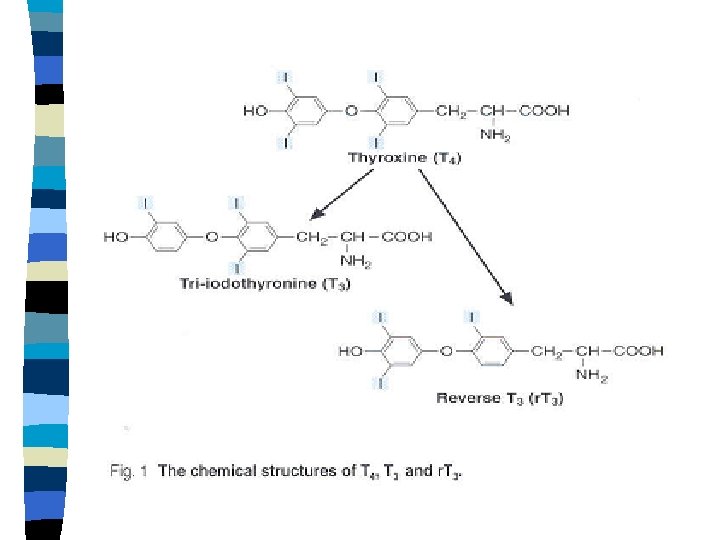
The Thyroid Gland • • • The location Thyroid hormone- thyroxine (T 4) and triiodothyronine (T 3). Most cells capable of taking up T 4 and deiodinating to the more biologically active T 3. It is T 3 which binds to receptors and triggers the end-organ effects of the thyroid hormones. T 4 can be metabolized to reverse T 3 (inactive)

Thyroid Hormone Action • Essential for the normal maturation and metabolism of all the tissues in the body. Plasma concentration Total (nmol/L) free (pmol/L) Extent of Half life protein (days) binding T 4 60 -144 9. 0 -26. 0 99. 98 6 -7 T 3 1. 0 -2. 9 3. 0 -9. 0 99. 66 1 -1. 5 Thyroid hormones in blood

Regulation of thyroid hormones _ Hypothalamus TRH + Anterior pituitary TSH + Thyroid T 4 + T 3 _
 Total T 4 (bound hormone")
Thyroid Function Test • • TSH (thyroid stimulating hormone) Total T 4 (bound hormone + free) Free T 4 TBG level Free T 3 Total T 3 (bound hormone + free) Titre of auto-antibodies to thyroid tissue antigens

TRH test • • Involves intravenous injection of TRH and the measurement of pituitary TSH secreted in response to the stimulation. Purposes: i) Investigation of pituitary disorders ii) Investigation of hyperthyroidism
 60 Primary")
Pituitary responses to TRH TRH Normal response TSH Hyperthyroidism 20 Time (minutes) 60 Primary hypothyroid TSH Normal response Secondary (pituitary) hypothyroid 20 Time (minutes) 60

Goitre • • A goitre is an enlarged thyroid gland. This may be associated with hypofunction, hyperfunction or indeed normal concentrations of thyroid hormones in blood.

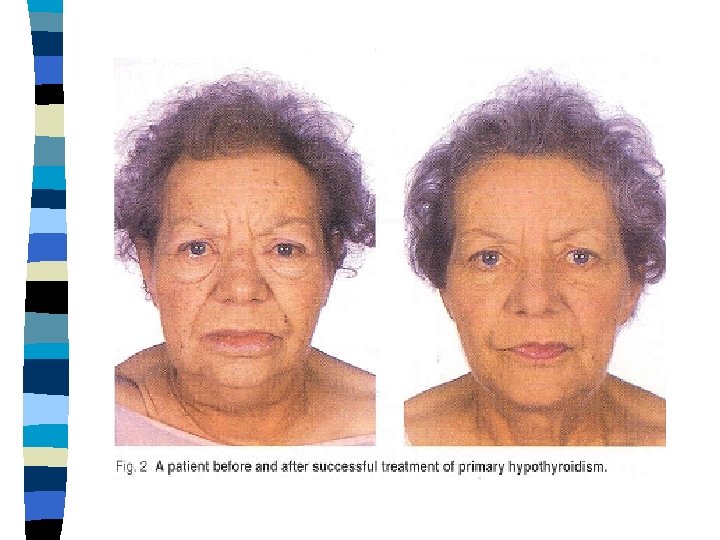
Hypothyroidism • 90% of cases of hypothyroidism occur as a consequence of: - autoimmune destruction of the thyroid gland (Hashimoto’s disease) - radioiodine or surgical treatment of hyperthyroidism

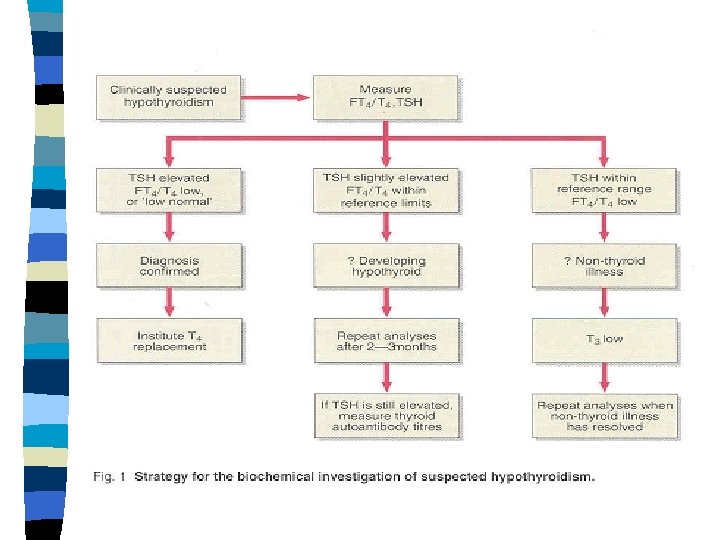
Diagnosis of Hypothyroidism • • Hypothyroidism is caused by a deficiency of thyroid hormones. Primary hypothyroidism – failure of the thyroid organ itself-elevated TSH concentration is diagnostic Secondary hypothyroidism-failure of pituitary to secrete TSH (less common). Treatment- thyroxine (tablet) therapy.

Non-thyroidal Illness • • • In systemic illness the normal regulation of TSH, T 4 and T 3 secretion and subsequently metabolism of the thyroid hormones, is disturbed. ↑ T 4 are converted to the reverse T 3. Reduction in thyroid hormone activity does not result in an increased serum TSH concentration. TSH secretion is suppressed→ ↓ T 4 and T 3. TBG decrease

Neonatal Hypothyroidism • • • The failure of the thyroid gland to develop properly during early embryonic growth. Children develop irreversible mental retardation and characteristic feature of cretinism. The screening test- ↑ blood TSH concentration.

Hyperthyroidism • Hyperthyroidism can be result from: - Graves’ disease, diffuse toxic goitre - Toxic multinodular goitre - solitary toxic adenoma - thyroiditis - exogenously administered iodine and iodine- containing drugs, e. g amiodarone - excessive T 4 and T 3 ingestion

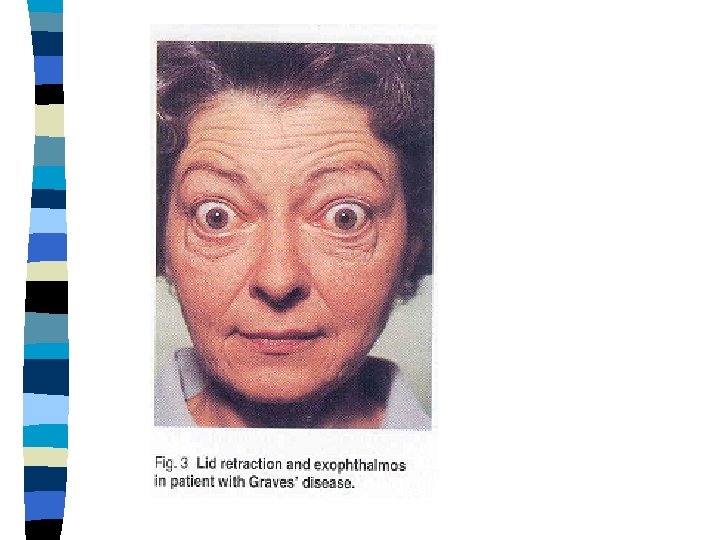
Graves’ disease • • • An autoimmune disease in which antibodies to the TSH receptor on the surface of the thyroid cells appear to mimic the action of the pituitary hormones. The normal regulatory controls on T 4 synthesis and secretion are lacking. Pituitary secretion of TSH is completely inhibited by the ↑ conc. of thyroid hormones in the blood-eyelid retraction

Diagnosis • • Suppressed TSH concentration, ↑ T 4 and T 3 - primary hyperthyriodism Occasionally, biochemical confirmation of suspected hyperthyroidism will prove more difficult e. g in pregnancy.
 55 -144)")
Pt T 4 nmol/L T 3 nmol/L TSH TBG mg/L (12 -30) 55 -144) (0. 9 -2. 8) m. U/L (0. 35 -5. 0) Free Comment T 4 pmol/L (9 -24) 1 130 2. 0 3. 4 25 18 Euthyroid 2 175 3. 6 1. 1 35 14 Euthyroid 3 190 5. 0 <0. 05 36 30 Hprthyroid Thyroid hormone and binding protein results in pregnancy
- younger patient Radioiodine-therapy")
Treatment • • • Anti-thyroid drugs (such as carbimazole and propylthiouracil)- younger patient Radioiodine-therapy with sodium I 131 is commonly used in older pt. Most will require eventually require replacement thyroxine. Surgery-thyroidectomy

Thank you
- Slides: 35