Emphysema and Bronchitis Dr Sowmya Uthaiah Assistant professor

Emphysema and Bronchitis Dr Sowmya Uthaiah Assistant professor Dept of pathology

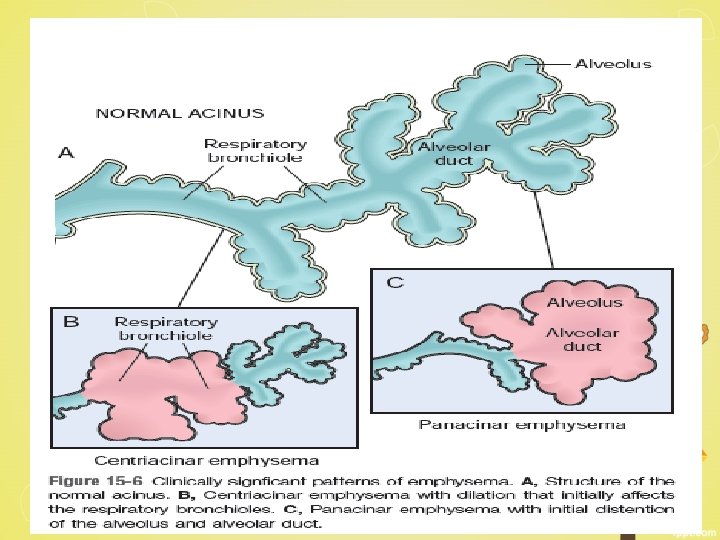
Emphysema Definition : Irreversible enlargement of the airspaces distal to the terminal bronchiole, accompanied by destruction of their walls without obvious fibrosis Emphysema is classified according to its anatomic distribution within the lobule. (1) Centriacinar (2) Panacinar (3) Paraseptal (4) Irregular
 emphysema • Most common- 95% • Heavy smokers, often in association with")
Centriacinar (centrilobular) emphysema • Most common- 95% • Heavy smokers, often in association with chronic bronchitis (COPD) • Central or proximal parts of the acini, formed by respiratory bronchioles • Distal alveoli are spared • Upper lobes, particularly in the apical segments • Inflammation around bronchi and bronchioles
, surrounded by relatively spared alveolar spaces.")
Centriacinar emphysema. Central areas show marked emphysematous damage(E), surrounded by relatively spared alveolar spaces.
 emphysema • Acini are uniformly enlarged from the level of the respiratory")
Panacinar (panlobular) emphysema • Acini are uniformly enlarged from the level of the respiratory bronchiole to the terminal blind alveoli • Lower zones and in the anterior margins of the lung • Most severe at the bases • Associated with α 1 -antitrypsin deficiency

Panacinar emphysema involving the entire pulmonary lobule.
 emphysema • Distal part involved • proximal portion of the acinus")
Distal acinar (paraseptal) emphysema • Distal part involved • proximal portion of the acinus – normal • more severe in the upper half of the lungs • more striking ü adjacent to the pleura ü along the lobular connective tissue septa ü at the margins of the lobules ü adjacent to areas of fibrosis, scarring, or atelectasis

§ Grossly: multiple, continuous, enlarged airspaces < 0. 5 cm to > 2. 0 cm in diameter, sometimes forming cystlike structures. § spontaneous pneumothorax in young adults
. • • acinus is irregularly involved associated with")
Airspace enlargement with fibrosis (irregular emphysema). • • acinus is irregularly involved associated with scarring small foci clinically insignificant

Other forms of emphysema § Compensatory hyperinflation § Obstructive overinflation § Bullous emphysema § Interstitial emphysema Bullous emphysema - large subpleural bullae

Pathogenesis

1. Inflammatory mediators and leukocytes Ø leukotriene B 4, IL-8, TNF etc Ø released by resident epithelial cells and macrophages Ø attract inflammatory cells from the circulation (chemotactic factors) Ø amplify the inflammatory process (proinflammatory cytokines) Ø induce structural changes (growth factors)

2. Protease-antiprotease imbalance Ø proteases are released from the inflammatory cells and epithelial cells Ø break down connective tissue components Ø relative deficiency of protective antiproteases

Deficiency of the antiprotease α 1 -antitrypsin Ø 1% of patients with emphysema Ø normally present in serum, tissue fluids, and macrophages Ø inhibitor of proteases eg. elastase Ø secreted by neutrophils during inflammation Ø injury (e. g. smoking)--- increases the activation and influx of neutrophils into the lung- local release of proteases- excessive digestion of elastic tissue and emphysema

3. Oxidative stress Ø tobacco smoke, alveolar damage, and inflammatory cells- produce oxidants Ø NRF 2 gene inactivation 4. Infection Ø bacterial and/or viral infections - exacerbate the associated inflammation and chronic bronchitis

Small airways are normally held open by the elastic recoil of the lung parenchyma loss of elastic tissue in the walls of alveoli that surround respiratory bronchioles reduces radial traction -----respiratory bronchioles to collapse during expiration------leads to functional airflow obstruction despite the absence of mechanical obstruction.

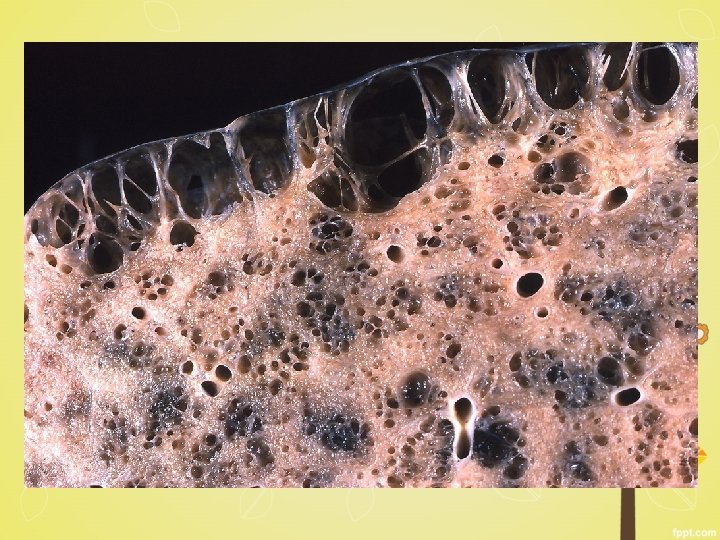
Gross: • voluminous lungs, often overlapping the heart • upper two thirds of the lungs • large apical blebs or bullae-irregular emphysema secondary to scarring and of distal acinar emphysema

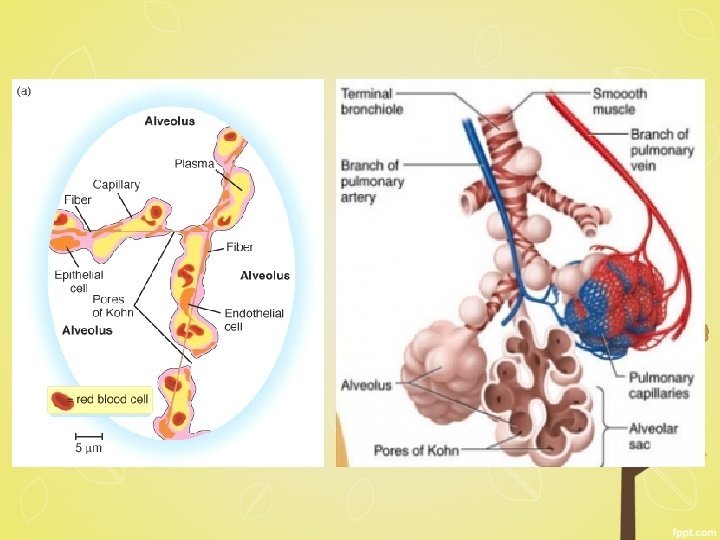
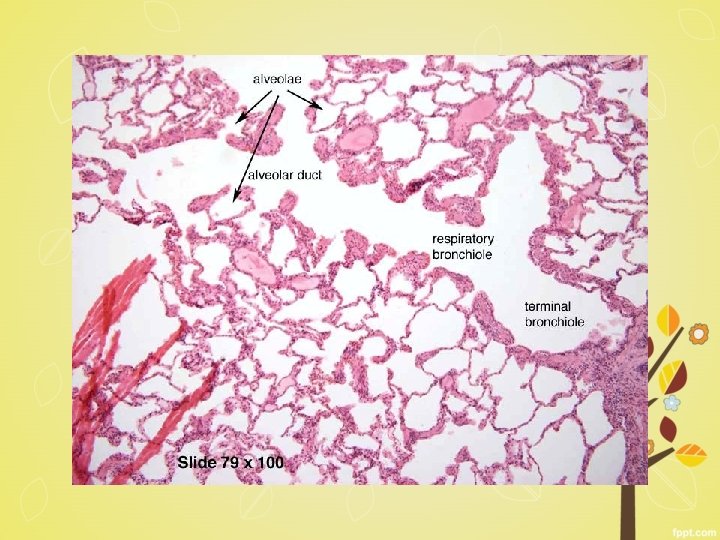
Microscopy § abnormally large alveoli are separated by thin septa with only focal centriacinar fibrosis § loss of attachments of the alveoli to the outer wall of small airways § large pores of Kohn- septa appear to be floating or protrude blindly into alveolar spaces with a clubshaped end. § alveolar walls destroyed - decrease in the capillary bed area § blebs or bullae-deform and compress the respiratory § bronchioles and vasculature of the lung.

Airway changes in emphysema § Goblet cell hyperplasia, with mucus plugging of the lumen § Inflammatory infiltrates in bronchial walls consisting of neutrophils, macrophages, B cells (sometimes forming follicles), and T cells § Thickening of the bronchiolar wall due to smooth muscle hypertrophy and peribronchial fibrosis narrow the bronchiolar lumen leads to airway obstruction

Dilated air spaces and loss of alveolar walls

Clinical features • dyspnea – insidious in onset & gradually progressive • cough or wheezing • cough and expectoration • Weight loss • Severe casesbarrelchested and dyspneic, prolonged expiration, sits forward in a hunched-over position, and breathes through pursed lips
 Coronary Artery Disease (2)")
• Overdistention---overventilate---well oxygenated--pink puffers • Death due to (1) Coronary Artery Disease (2) Respiratory Failure (3) Right Sided Heart Failure (4) Massive Collapse Of The Lungs

Treatment • smoking cessation • oxygen therapy • long-acting bronchodilators with inhaled corticosteroids • physical therapy • bullectomy • lung volume reduction • surgery and lung transplantation • α 1 -AT replacement therapy

Chronic Bronchitis -defined clinically as persistent cough with sputum production for at least 3 months in at least 2 consecutive years, in the absence of any other identifiable cause.

Pathogenesis • exposure to noxious or irritating inhaled substances such as tobacco smoke • dust from grain, cotton, and silica

cigarette smoke § damage airway lining cells § chronic inflammation § interferes with the ciliary action of the respiratory epithelium - prevents clearance of mucus increases the risk of infection

1. Mucus hypersecretion § in large airways § hypertrophy of the submucosal glands in the trachea and bronchi § inflammatory mediators such as histamine and IL-13 § increase in goblet cells in small airways—small bronchi and bronchioles---excessive mucus production---- airway obstruction

2. Inflammation § acute and chronic inflammatory - neutrophils, lymphocytes, macrophages § fibrosis involving small airways-chronic airway obstruction

3. Infection -does not initiate chronic bronchitis, -maintains and produces acute exacerbations Grossly § hyperemia, swelling, and edema of the mucous membranes § excessive mucinous or mucopurulent secretions § heavy casts of secretions and pus fill the bronchi and bronchioles
 § enlargement of the mucus-secreting")
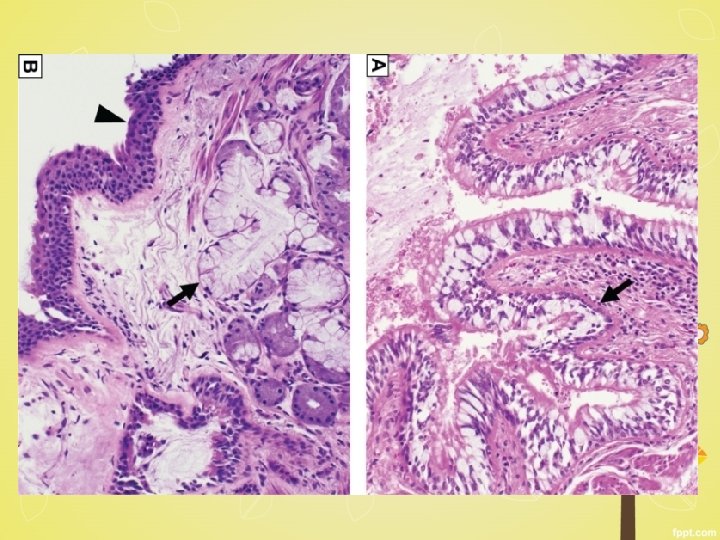
Microscopy § mild chronic inflammation of the airways (lymphocytes) § enlargement of the mucus-secreting glands of the trachea and bronchi § Hyperplasia of mucous glands § Bronchial epithelium- squamous metaplasia and dysplasia § marked narrowing of bronchioles -mucus plugging, inflammation, and fibrosis § Obliteration of lumen due to fibrosis (bronchiolitis obliterans).

Normal bronchial epithelium

Clinical features § persistent cough productive of sparse sputum § dyspnea on exertion § hypercapnia, hypoxemia, and mild cyanosis “blue bloaters” § cor pulmonale § cardiac failure -

Differences between emphysema and chronic bronchitis

- Slides: 39