Emergency Ultrasound in Trauma Anthony J Weekes MD





 l CAT Scan")











 patients w/ free fluid on “gold standard” l All patients:")






 l Consists of 4 views – Subxiphoid –")







 l Coagulating blood – First")










 is smaller than liver")








")

























- Slides: 91
Emergency Ultrasound in Trauma Anthony J Weekes MD, RDMS Janet G. Alteveer, MD Sarah Stahmer, MD
Clinical Case l GR is a 62 y male who hit his right torso when he slipped on an icy sidewalk. He denies head trauma, and can walk without a limp. Two hours later the pain in his lower chest has increased he comes to the ED.
Clinical Case l PE: BP 116/72, pulse 109, RR 24. l There is a minor abrasion to right lateral chest, which is tender to palpation. Diffuse mild abdominal tenderness. l Meds: Coumadin for irregular heartbeat
Clinical Case 2 large IV’s placed, CXR done. Blood tests sent. l Bedside ultrasound done. l CXR revealed lower rib fractures, no HTX or PTX l
Clinical Case l FFP l He ordered and OR notified. is found to have a liver laceration and 500 cc of blood in the peritoneal cavity.
Diagnostic Modalities in Blunt Abdominal Trauma l Diagnostic Peritoneal Lavage (DPL) l CAT Scan l Ultrasound (FAST exam)
Diagnostic Peritoneal Lavage l Advantages – Very sensitive for identifying intraperitoneal blood – 106 RBC/mm 3 approx. 20 ml blood in 1 L lavage fluid – Can be done at the bedside – Can be done in 10 -15 minutes l Disadvantages – Overly sensitive, may result in too high a laparotomy rate – Invasive – Difficult in pregnancy, or with many prior surgeries – Can not be repeated
CT Scan l Advantages l Disadvantages – Identifies specific – Expensive equipment injuries – Good for hollow viscus and retroperitoneal injury – High sensitivity and specificity – 30 -60 minutes to complete study – Only for stable patients – Not for pregnant patients
Focused Abdominal Sonography in Trauma FAST
FAST l Advantages l Disadvantages – Can be performed in 5 – Operator dependent minutes at the bedside – Non-invasive – Repeat exams – Sensitivity and specificity for free fluid equal to DPL and CT – May not identify specific injury – Poor for hollow viscus or retroperitoneal injury – Obesity, subcutaneous air may interfere with exam
FAST Principles Detects free intraperitoneal fluid l Blood/fluid pools in dependent areas l Pelvis l – Most dependent l Hepatorenal fossa – Most dependent area in supramesocolic region
FAST Principles l Pelvis and Supramesocolic areas communicate – Phrenicolic ligament prevents flow l Liver/spleen injury – Represents 2/3 of cases of blunt abdominal trauma
FAST- principles l Intraperitoneal fluid may be – Blood – Preexisting ascites – Urine – Intestinal contents
FAST – limitations l US relatively insensitive for detecting traumatic abdominal organ injury l Fluid may pool at variable rates – Minimum volume for US detection – Multiple views at multiple sites – Serial exams: repeat exam if there is a change in clinical picture l Operator dependent
Evidence supporting use of FAST l Multiple studies in USA by EM and trauma surgeons l Studies from Europe and Japan l Policy statements by specialty organizations
Emergency department ultrasound in the evaluation of blunt abdominal trauma. Jehle, D. , et al, Am J Emerg Med, 1993 – Single view of Morison’s pouch in 44 patients – Performed by physicians after 2 weeks training – US compared to DPL and laparotomy – Sensitivity 81. 8% – Specificity 93. 9%
Trauma surgical study l A prospective study of surgeon- performed ultrasound as the primary adjuvant modality of injured patient assessment. 1994 Rozycki et al. l N=358 patients l Outcomes used: US detection of hemoperitoneum/pericardial effusion
Results l 53/358 (15%) patients w/ free fluid on “gold standard” l All patients: Sens 81. 5%, spec 99. 7% l Blunt trauma: Sens 78. 6%, spec 100% l PPV 98. 1%, NPV 96. 2% l Overall accuracy was 96. 5% for detection of hemoperitoneum or pericardium
Trauma Study l Rozycki G, et al 1998 Surgeon-performed ultrasound for the assessment of truncal injuries. Lessons learned from 1540 patients l FAST exam on patients with precordial or transthoracic wounds or blunt abdominal trauma
Protocol: + Pericardial fluid Stable OR CT Unstable OR +IP fluid l Results – N= 1540 pts, 80/1540 (5%) with FF – Overall: Sens 83. 3%, Spec 99. 7% – PPV 95%, NPV 99% – Precordial/Transthor : Sens 100%, Spec 99. 3% – Hypotensive BAT: Sens 100%, Spec 100%
FAST – Specialty Societies Established clinical role in Europe, Australia, Japan, Israel l German Surgical Society requires candidates’ proficiency in ultrasound l United States l – US in ATLS – US policies by frontline specialties l l American College of Surgeons ACEP, SAEM & AAEM
FAST Perform during – Resuscitation – Physical exam – Stabilization
Equipment Curved array l Various “footprints” – Small footprint for thorax – Large for abdomen l Variable frequencies – 5. 0 MHz: thin, child – 3. 5 MHz: versatile – 2. 0 MHz: cardiac, large pts
Time to Complete Scan l Each view: 30 -60 seconds l Number of views dependent on clinical question and findings on initial views l Total exam time usually < 3 -5 minutes l 1988 Armenian earthquake – 400 trauma US scans in 72 hrs
Focused Abdominal Sonography for Trauma (FAST) l Consists of 4 views – Subxiphoid – Right Upper Quadrant – Left Upper Quadrant – Pouch of Douglas
FAST Increased sensitivity with increased number of views l Will identify pleural effusions l Reliably detects as little as 50 -100 cc in the thorax l Sensitivity >96%, specificity 99 -100% l
Clinical experience with FAST l Intraperitoneal fluid – Sensitivity 82 -98%, specificity 88 -100% l Morison’s pouch alone 36 -82% sensitivity l Increased sensitivity with – Increasing number of views – Trendelenberg – Serial examinations l Can detect as little as 250 cc of free fluid
Clinical Experience l Solid organ disruption – 40% sensitivity for all organs – 33 -94% for splenic injury l Hollow viscus injury – Sensitivity 57% l Retroperitoneal injury – Sensitivity for identification of hemorrhage <60%
RUQ Probe at right thoracoabdominal junction l Liver : large acoustic window l Probe marker cephalad l Rib interference? l – Rotate 30° counterclockwise
Scan Plane l Same image if probe positioned – Anterior – Mid axillary – Posterior
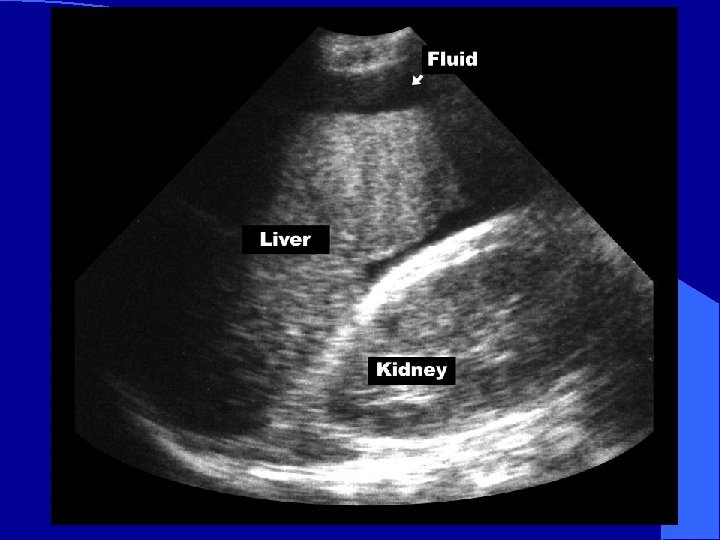
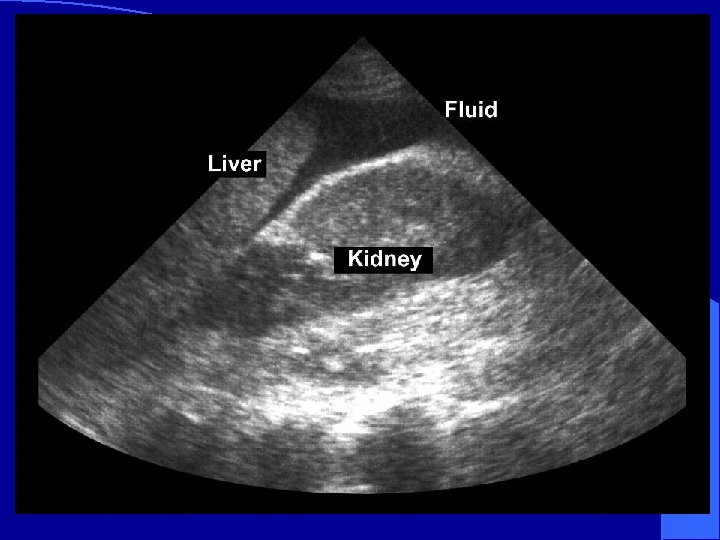
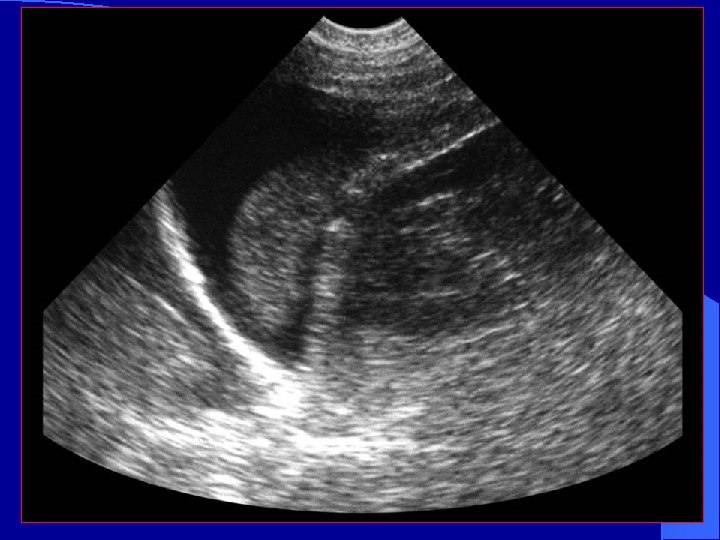
RUQ l Image on screen: – Liver cephalad – Kidney inferiorly – Morison’s Pouch*: space between Glisson’s capsule and Gerota’s fascia * *
Normal RUQ l Image kidney – Longitudinally – Transversely l Two toned structure – Cortex/medulla – Renal sinus
Appearance of blood l Fresh blood – Anechoic (black) l Coagulating blood – First hypoechoic – Later hyperechoic
Normal Morison’s Pouch Free fluid in Morison’s Pouch
Branney, S. W. et al: Quantitative sensitivity of ultrasound in detecting free intraperitoneal fluid J Trauma: 1995: 39 l Peritoneal lavage fluid infused in 100 patients l Simultaneous scan of Morison’s pouch – By physicians ( Surgery, EM, Radiology) – Blinded to volume and rate of infusion – Mean volume of detection: 619 cc – Sensitivity at 1 liter: 97% – 10% physicians detected less than 400 cc
Volume Assessment by US l Caveat to Branney study: – Artificial condition: infused fluid – Fluid in Morison’s after pelvis overflow l Tiling et al : – 200 -250 ml detected by US – Collection >0. 5 cm suggests over 500 ml l Transvaginal/rectal – 15 ml of free intraperitoneal fluid
Detection of Fluid by Ultrasound Affected by positioning l Location of bleed l Rate of bleeding l Operator Experience l l Value of sensitivity of Ultrasound: – Detects clinically injuries – Non-detection of fluid l May indicate self- limited bleeding
All Fluid is not Blood l Ascites l Ruptured Ovarian Cyst l Lavage fluid l Urine from ruptured bladder
Mimics of Fluid in RUQ l Perinephric fat – May be hypoechoic like blood – Usually evenly layered along kidney – If in doubt, compare to left kidney l Abdominal inflammation – Widened extra-renal space – Echogenicity of kidney becomes more like the liver parenchyma
Pitfalls l RUQ – Not attempting multiple probe placements – Not placing the probe cephalad enough to use the acoustic window of the liver Scanning too soon before enough blood has accumulated l Not repeating the scan l
LUQ l Probe at left posterior axillary line l Near ribs 9 and 10 l Angle probe obliquely (avoid ribs)
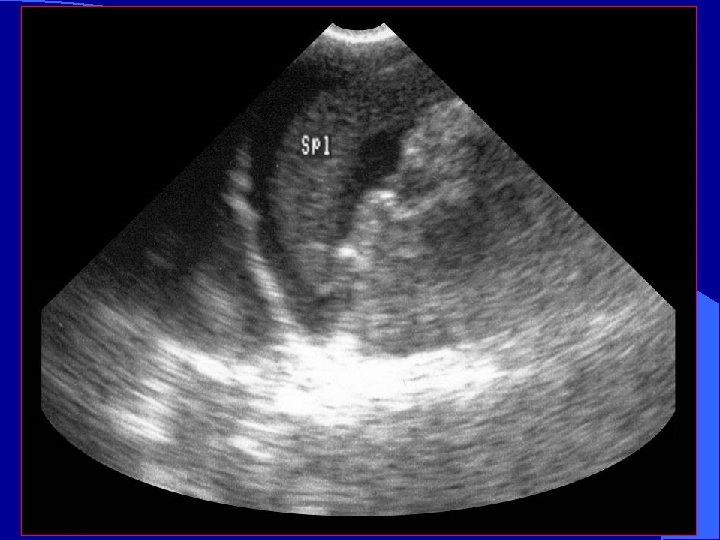
LUQ Scan Plane l More difficult – Acoustic window (spleen) is smaller than liver – Mild inspiration will optimize image – Bowel interference is common
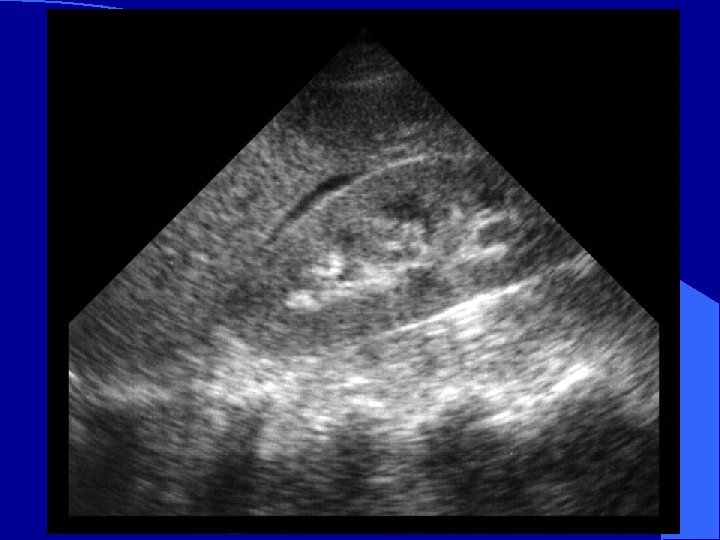
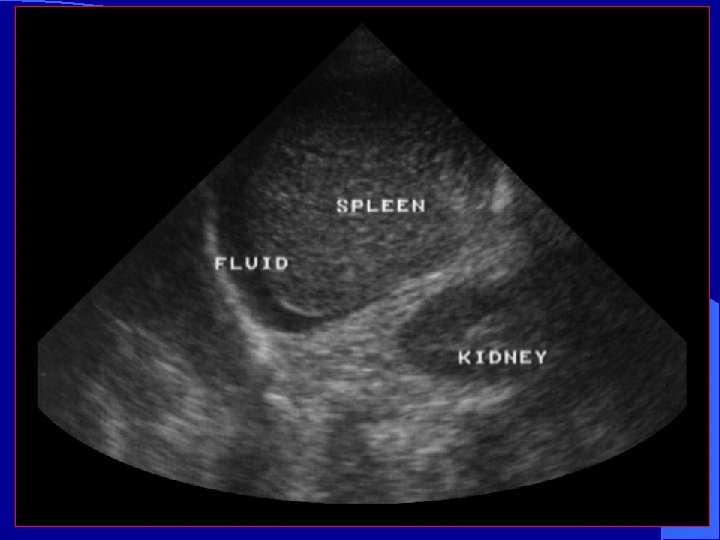
LUQ Scan spleen * * * kidney * *Splenorenal fossa – a potential space
Normal Spleno -renal view Free fluid around spleen
To Evaluate the Thorax l Move probe – cephalad – longitudinal l Image Liver Diaphragm Pleural space
Hemothorax liver fluid diaphragm
Small Pleural Effusion Large Pleural Effusion
Ma O John, Mateer J, Trauma Ultrasound Examination Versus Chest Radiography in the Detection of Hemothorax Ann Emerg Med: March 1997 l 240 trauma US study patients l 26 had hemothorax ( CT or chest tube) l CXR and US – 0 false positive – 1 false negative – 25 true positive – 214 true negative
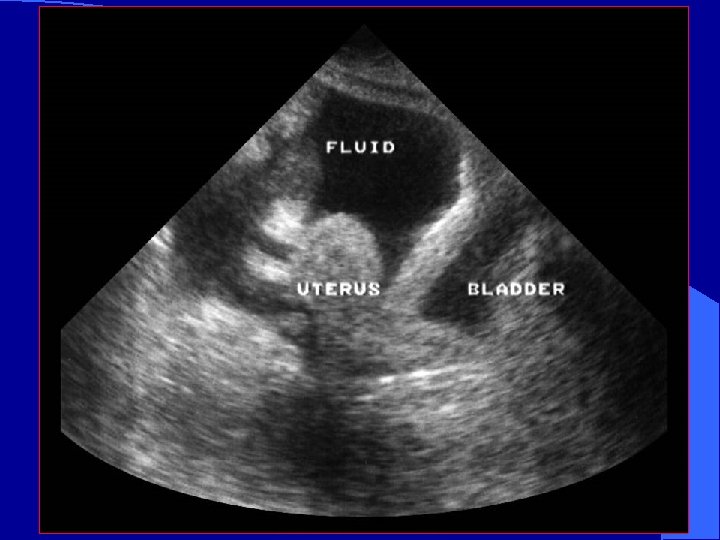
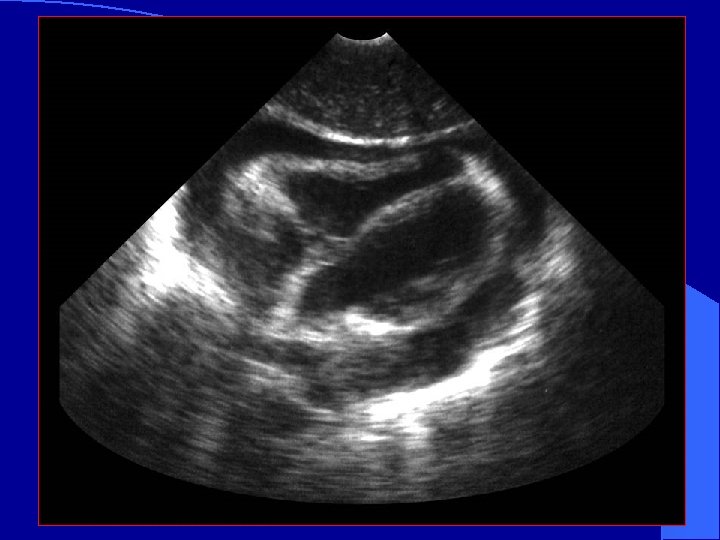
Pelvic View Probe should be placed in the suprapubic position l Either can be transverse or longitudinal l Helpful to image before placement of a Foley catheter l
Pelvis (Long View)
Pelvis: Transverse
Normal Transverse pelvic Fluid in pelvis
Pelvic View – Sagittal clot Fluid in front of the bladder l If bladder is empty or Foley already placed: Trick of trade l – IV bag on abdomen – Scan through bag bladder
Blood in the Pelvis
Free fluid in the pelvis
FAST Algorithm
Ultrasound in the Detection of Injury From Blunt or Penetrating Thoracic Trauma
Penetrating Thoracic Injury l Clinical challenge – Where is the penetration? – What was the weapon? – What was the trajectory? – What organ(s) have been injured? – Improved outcomes in patients with normal or near-normal vital signs
Penetrating Cardiac Trauma l Pericardial effusion – May develop suddenly or surreptitiously – May exist before clinical signs develop l Salvage rates better if detected before hypotension develops
Clinical Case l QD is 37 year old male brought in by EMS for ingesting entire bottle of unidentified red and white pills. In the ambulance bay he pulls out a knife and stabs himself in the left nipple.
Clinical Case l Initial BP 116/72, pulse 109 RR 24. IV’s placed. l No JVD, Clear breath sounds, non tender abdomen l As CXR is about to be done, pulse increases to 134. l Bedside ultrasound is done while cartridge is developed.
Clinical Case
Clinical Case l Patient is taken to the OR l Penetrating cardiac wound is repaired
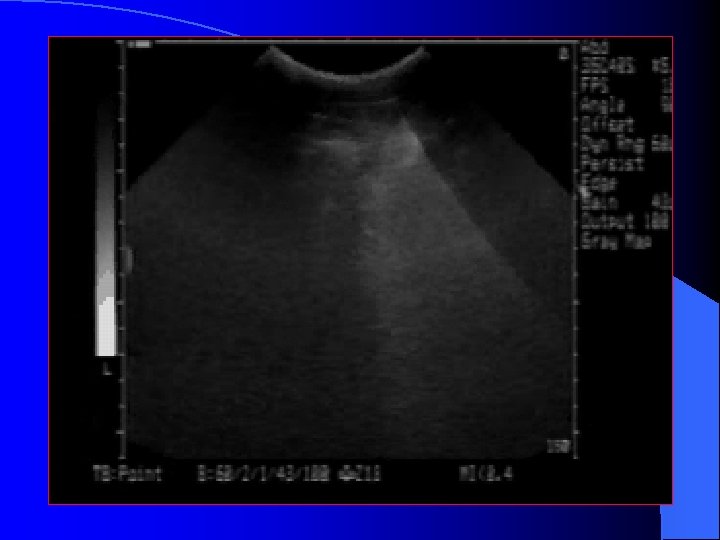
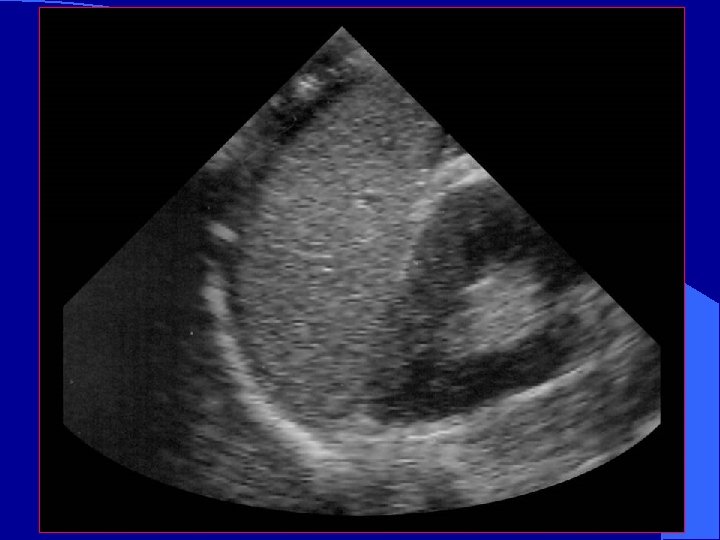
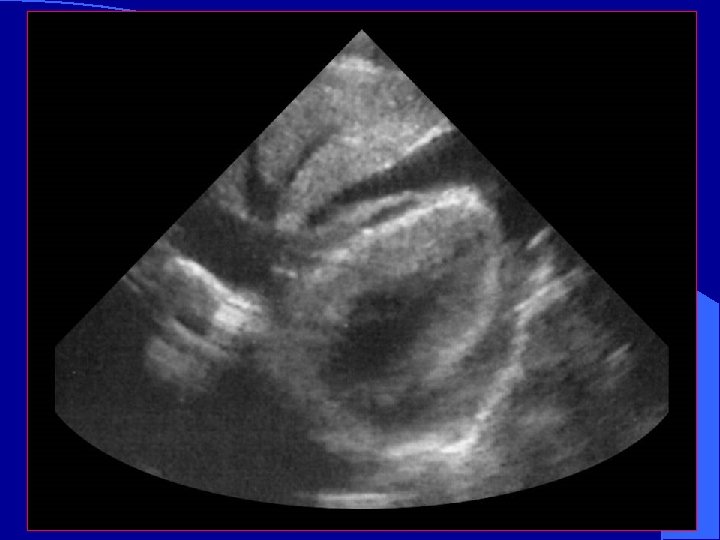
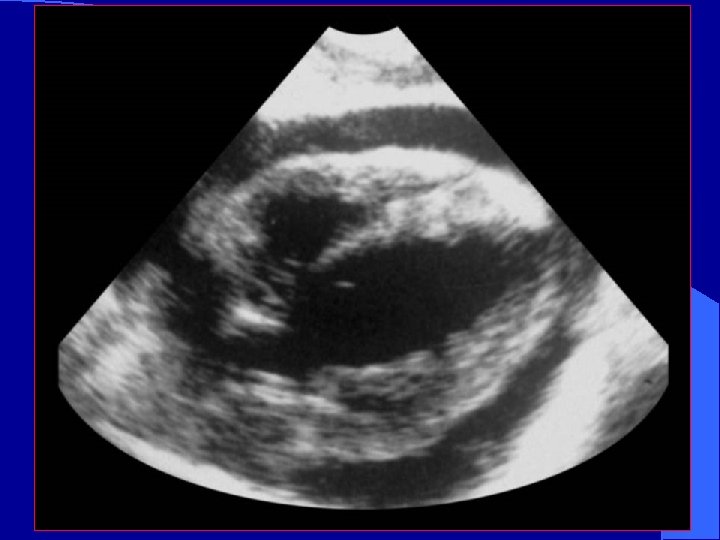
Subcostal View l. Most practical in trauma setting l. Away from airway and neck/chest procedures l. Also called Sub- Xyphoid view
Subcostal View
Subcostal View
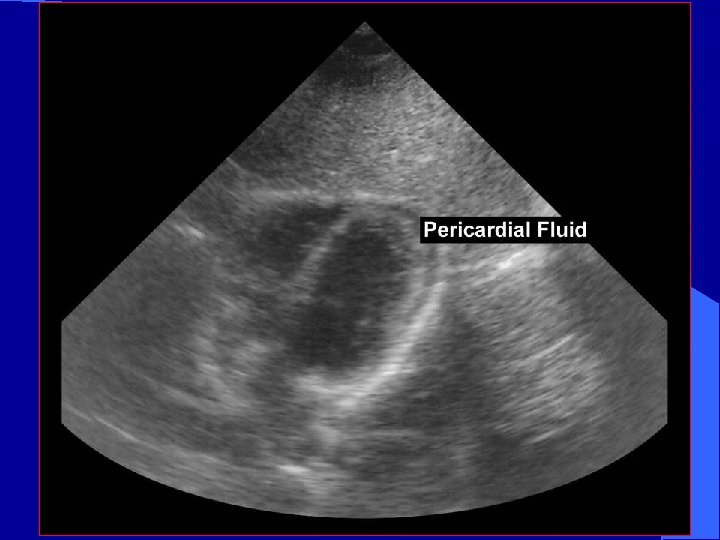
Pericardial Fluid fluid
Occult Penetrating Cardiac Trauma l Observation unreliable l Subxiphoid window – Invasive – 100% sensitive, 92% specific – Negative exploration rates (as high as 80%) l Ultrasound reliable indicator of even small pericardial effusion
Trauma Study The role of ultrasound in patients with possible penetrating cardiac wounds: a prospective multicenter study. Rozycki GS: J Trauma. 1999 Pericardial scans performed in 261 patients l Sensitivity 100%, specificity 96. 9% l PPV: 81% NPV: 100% l Time interval BUS to OR: 12. 1 +/- 5. 9 min l
Avoid Pitfalls l Normal echo does not definitively rule out major pericardial injury l Repeat echo with clinical picture l Epicardial fat pad may easily be misinterpreted as “clot” l Hemothorax may be confused with pericardial effusion
Blunt Cardiac Trauma l Basic Assessments – Pericardial effusion – Assess for wall motion abnormality – RV: l l closest to anterior chest wall Most likely to be injured l Advanced Assessments – Assess thoracic aorta – may need TEE to see all of thoracic aorta l l l Hematoma Intimal flap Abnormal contour – Valvular dysfunction or septal rupture
Blunt cardiac trauma l Injuries difficult to assess by FAST – Valvular incompetence – Myocardial rupture – Intracardiac thrombosis – Ventricular aneurysm – Coronary Thrombosis – Intra-cardiac Thrombosis
“ The most important preoperative objective in the management of the patient with trauma is to ascertain whether or not laparotomy is needed, and not the diagnosis of a specific organ injury”