Emergency Department Management of the Abused Child Jim

Emergency Department Management of the Abused Child Jim Holliman, M. D. , F. A. C. E. P. Professor of Military and Emergency Medicine Uniformed Services University of the Health Sciences Clinical Professor of Emergency Medicine George Washington University Bethesda, Maryland, U. S. A.



Child Abuse Lecture Objectives ŸPresent background information on definition and epidemiology ŸRecognize signs of abuse ŸPhysical exam findings ŸRadiographic findings ŸEmergency Department (E. D. ) management of cases ŸFollowup and prevention

Child Abuse Historical Landmarks Ÿ 1940's : Caffey described the syndrome Ÿ 1962 : Kempe coined term "battered child syndrome" Ÿ 1963 : Fontana coined term "maltreatment syndrome in children" Ÿ 1970's : Increasing recognition and identification of cases

Child Abuse Definitions Ÿ"Any interaction or lack of interaction between family members or caretakers, which results in nonaccidental harm to the child's physical or developmental state" ŸOr "any deliberate harm inflicted on a child by a caretaker" ŸAlso termed : Ÿ"child battering" ŸNon-Accidental Trauma (NAT) Ÿ"Shaken baby syndrome"

Child Abuse Types or Classification ŸPhysical abuse ŸBlows or strikes ŸPulls or twists (causing fractures) ŸStrangulation ŸBurns or scalds ŸForced restraint ŸDrowning ŸHair pulling ŸForced ingestions
 ŸSexual abuse ŸInappropriate exposure ŸInappropriate touching ŸSexual intercourse")
Child Abuse Types or Classification (continued) ŸSexual abuse ŸInappropriate exposure ŸInappropriate touching ŸSexual intercourse ŸSodomy ŸObject insertion ŸSurgical alteration of genitalia (such as clitorectomy)
 ŸPhysical neglect ŸUncleanliness ŸMalnutrition ƒ Growth disturbance ŸSusceptibility")
Child Abuse Types or Classification (continued) ŸPhysical neglect ŸUncleanliness ŸMalnutrition ƒ Growth disturbance ŸSusceptibility to infections ŸHyper- or hypo- thermia ŸAccidental injuries or ingestions by the child
 ŸEmotional abuse or neglect, causing : ŸAnxiety, depression,")
Child Abuse Types or Classification (continued) ŸEmotional abuse or neglect, causing : ŸAnxiety, depression, even suicide ŸNightmares, sleep disturbances ŸHeadaches, other nonspecific physical complaints ŸRegression to earlier developmental levels ŸDrug or alcohol abuse ŸRefusal to speak ŸInadequacy in education
 Ÿ\"Munchausen's by proxy syndrome\" ŸIs false reporting of")
Child Abuse Types or Classification (continued) Ÿ"Munchausen's by proxy syndrome" ŸIs false reporting of symptoms in a child by a caretaker ŸOr infliction of medical signs (induced fever, apnea, skin lesions, etc. ) ŸFirst reported in 1977 Ÿ"Goal" is subconscious desire by caretaker for attention ŸVery difficult to "cure" the caretaker

Child Abuse Scope of the Problem ŸProminent problem in all countries and cultures Ÿ? increasing incidence versus increasing recognition in last 20 years ŸAnnual incidence in U. S. A. : Ÿ> 1, 000 physical abuse cases Ÿ> 3000 deaths Ÿ> 300, 000 sexual abuse cases Ÿ> 250, 000 psychological abuse cases

Child Abuse : Parental Factors Correlated with Being an Abuser ŸTeenage parent ŸSingle parent ŸLow socioeconomic status ŸDivorced or separated ŸDrug or alcohol abuser ŸArrests for violence acts ŸCrowded household ŸLow self esteem ŸThemself abused as a child ŸEmotionally immature ŸDepression ŸPoor impulse control ŸUnrealistic expectations ŸRecent loss of job or family member

Child Abuse : Children Prone to Being Abused Ÿ< 6 years old ŸPhysically or mentally handicapped ŸTwins ŸUnwanted pregnancy ŸChronically or recurrently ill

Features of the Medical History Which May Indicate Child Abuse ŸHistory not consistent with severity or type of injury or with child's development level ŸDelay between time of injury and presentation ŸHistory of multiple or recurrent prior injuries ŸDifferent history of injury from caretaker(s) than from the child ŸCaretaker reacts inappropriately to situation (either "under-" or "over-" reaction) ŸCaretaker(s) do not know etiology of the injury ŸHistory changes when asked again or repeated ŸChild is afraid of caretaker

Physical Exam Findings Indicative of Possible Child Abuse ŸMultiple injuries of various ages ŸBruises in different stages of devlopment and in areas not over bony prominences ŸPerioral, perineal, anal, or genital injuries ŸBizarre injuries such as cigarette burns, bite or belt or rope marks ŸSharply demarcated burns ŸRetinal hemorrhages ("shaken baby syndrome")

Child Abuse : Usual Aging Appearance of Bruises Age in Days 0 to 1 Appearance Tender, swollen 0 to 5 5 to 7 Black and blue Green 7 to 10 Yellow 10 to 14 Brown Over 14 Resolve or clear (this progression is not always consistent, however)


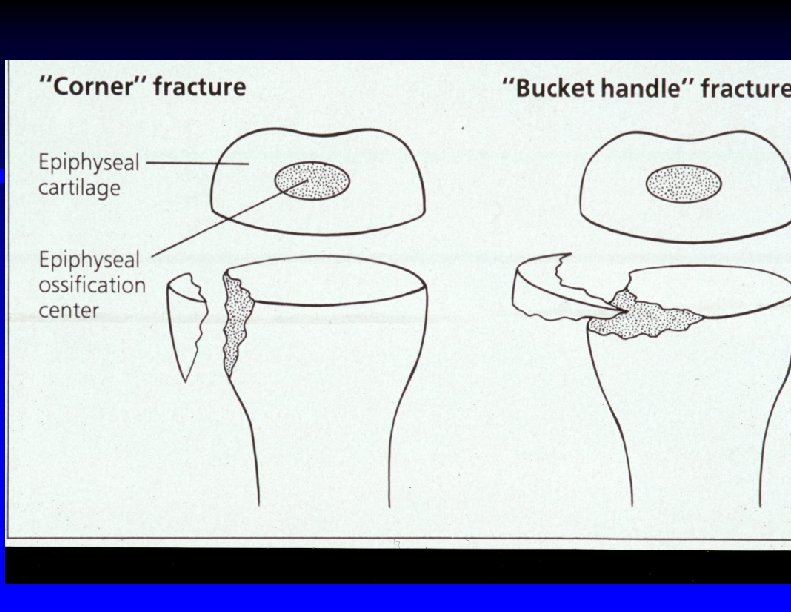
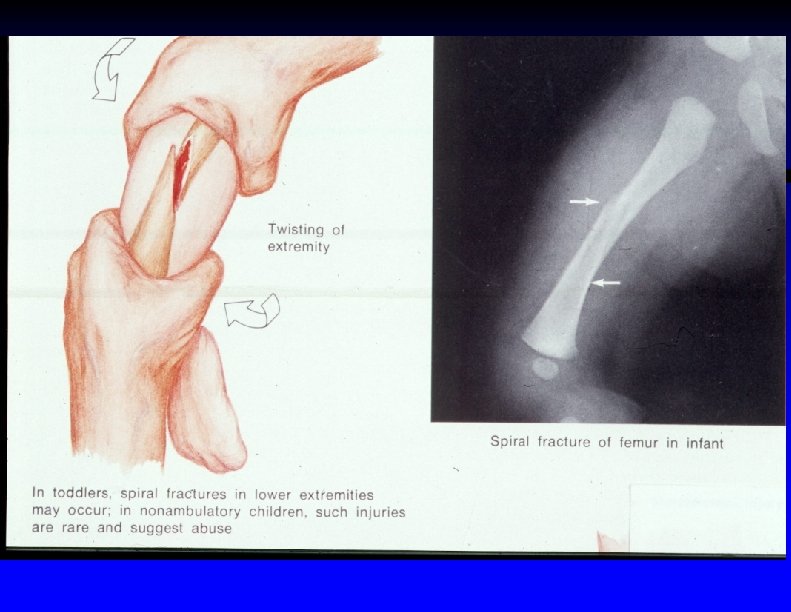
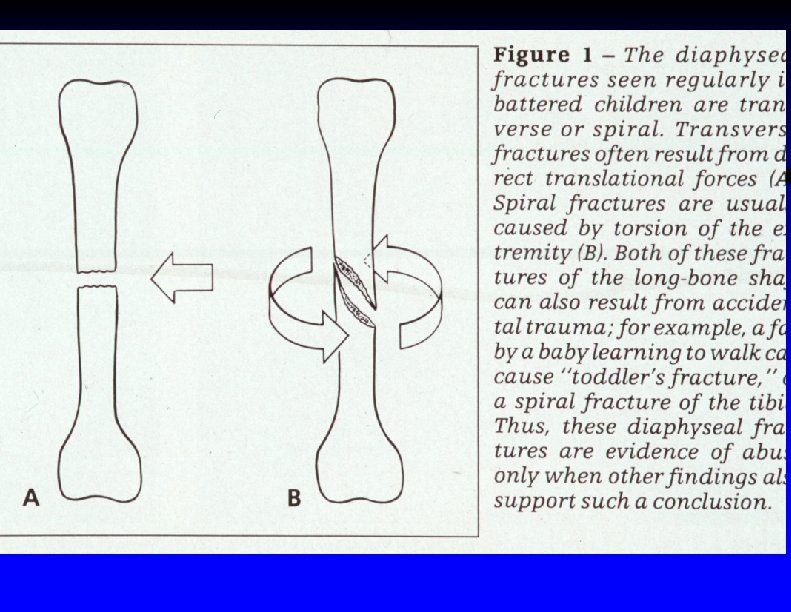
Child Abuse : X-Ray Findings Indicating Possible Child Abuse ŸMultiple fractures in different stages of healing ŸMultiple rib fractures Ÿ"Bucket handle" metaphyseal fractures ŸSpiral fractures of long bones ŸFemur fractures in preambulatory infants

Multiple forearm fractures in an abused child

")
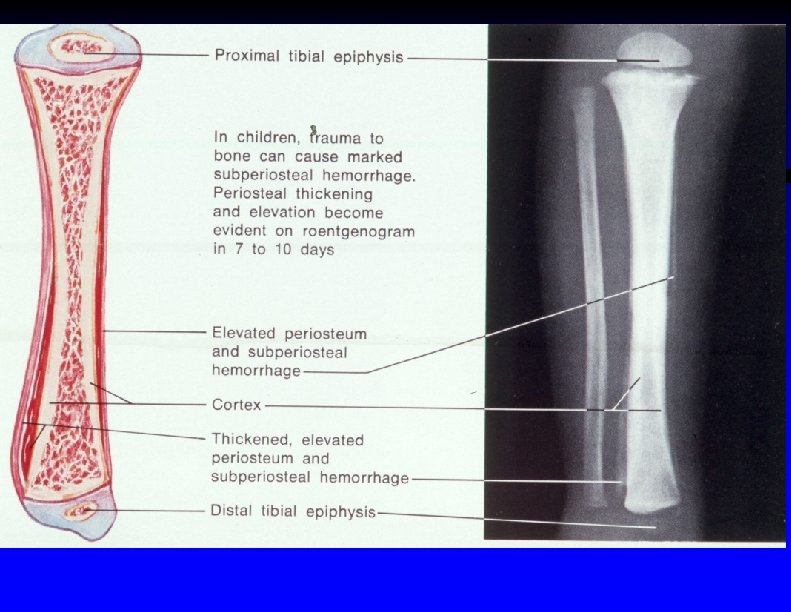
Periosteal cloaking in an infant (small arrows show subperiosteal hematoma)

Mechanism of metaphyseal fractures

Metaphyseal avulsion fracture of distal radius

Metaphyseal corner fracture in a 5 month old boy

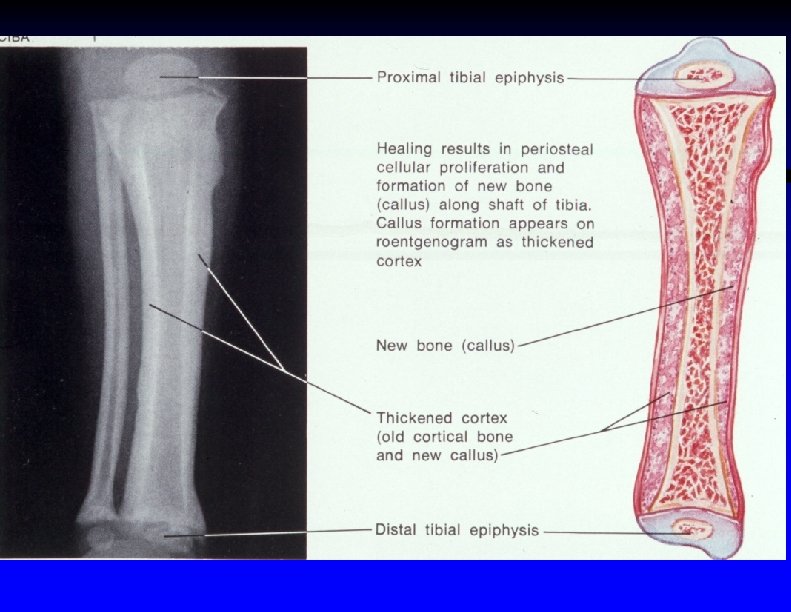
Callus from old bucket handle fracture in a 4 month old male

Metaphyseal fracture caused by jerking the limb

Spiral fracture of left humerus in a 9 month old female
")
Femur fracture in 4 month old male (arrow shows callus starting to calcify)

Healing spiral fracture of right femur in a 2 year old male with osteogenesis imperfecta tarda

Vertebral compression fractures caused by abuse in an 8 month old male

Skin Conditions That May Mimic Signs of Child Abuse ŸMongolian spots ŸOther "birthmarks" such as hemangiomas ŸFolk treatments such as "cupping" or "coining" ŸThrombocytopenia or congenital coagulation disorders ŸAlopecia areata or tinea infections

Medical Conditions Which Can Mimic Skeletal Findings of Child Abuse ŸOsteogenesis ŸCleidocranial imperfecta ŸDisuse osteopenia ŸProgeria ŸProstaglandin therapy ŸRickets ŸScurvy dysostosis ŸCongenital syphilis ŸHomocystinuria ŸHypophosphatasia ŸMeningomyelocele ŸMenkes disease ŸMetastatic bone tumors

Signs Which Indicate Possible Munchausen Syndrome by Proxy ŸExperienced physicians caring for the child are perplexed by the case ŸChild has received care at multiple different sites ŸChild's symptoms are persistent, recurrent, & do not respond to therapy ŸChild's symptoms never occur when witnesses are present ŸSymptoms resolve in a monitored environment ŸMother is overly attentive & enthusiastic about additional tests ŸMother has a medical or para-medical background ŸLaboratory results do not correlate with the case

Aspects of Munchausen Syndrome By Proxy ŸOverall mortality 9 % Ÿ 98 % of perpetrators are biologic mothers ŸExamples : ŸLying about symptoms such as persistent vomiting ŸGiving poisons, ipecac, salts, or insulin to induce apnea, seizures, emesis, or diarrhea ŸSimulating bleeding with exogenous blood ŸInducing or simulating fever ŸInducing skin rashes or lesions ŸMay be history of unusual death in a sibling

Aspects of Head Trauma in Child Abuse ŸLeading cause of fatal child abuse Ÿ 10 % of abused children show signs of head trauma ŸMost severe injuries in children < age 2 ŸSkull fractures are second most common skeletal injury with abuse ŸSuspect child abuse if "complex" skull fracture (multiple or "eggshell", displaced, diastatic, comminuted, or cross suture lines)

Child Abuse "Shaken Baby Syndrome " ŸMay present with coma or seizures without obvious evidence of scalp trauma ŸRecent studies indicate most cases not caused by shaking alone but by thrown impact of head against wall or object ŸSo suggested to rename syndrome "Shaken Impact Syndrome" ŸRetinal hemorrhage in up to 80 % ŸOnly seen in 3 % of accidental head trauma cases ŸCan lead to blindness
 ŸSkull")
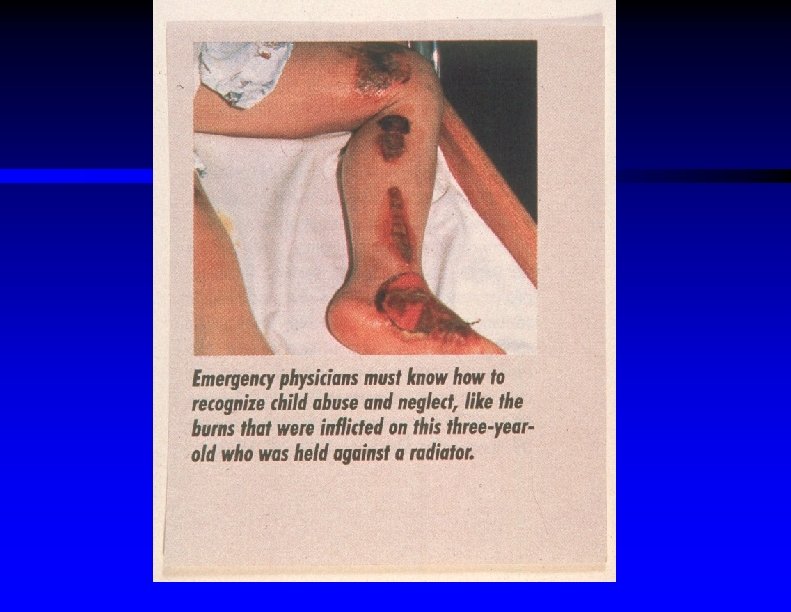
Summary of Major Injuries Seen With Physical Child Abuse ŸHead trauma (10 %) ŸSkull fractures, intracranial bleeding ŸLimb fractures (30 %) ŸChest trauma, mainly rib fractures ŸAbdominal trauma (second leading cause of death) ŸMay have organ perforation, obstruction, or rupture ŸSkin bruises, lacerations, or burns ŸPerineal or genital injuries ŸMay not always represent sexual abuse, but may be punishment for toilet training accidents

Immersion scald burns due to abuse

Inflicted scald burns

Inflicted scald burns

Scalp laceration from hit with belt buckle

Belt injury marks
 Management of the Abused Child ŸInitially be non-judgemental")
Initial Emergency Department (E. D. ) Management of the Abused Child ŸInitially be non-judgemental ŸPriority is to protect the child ŸResuscitation and exam same as for other trauma patients ŸNotify child protection authorities (and law enforcement authorities) ŸMay need to photograph the patient ŸMay need protective admission to hospital

Secondary E. D. Management of the Abused Child ŸConsider radiographic "skeletal survey" to look for old fractures ŸMay consider radionuclide bone scan if older injuries suspected, plain films indeterminate, or metabolic bone disease possible ŸComputed tomography if head or abdominal trauma ŸBloodwork to assess coagulation status ŸMay need other bloodwork to assess nutritional status

Bone scan showing multiple rib fractures

Two year old boy with healing spiral fracture of right femur

Considerations to Confirm Diagnosis of Munchausen By Proxy Syndrome ŸMay require hidden video monitoring of patient and caretaker ŸMay require forensic testing such as test emesis for ipecac ŸShould check status of other siblings ŸOut of home placement usually needed ŸLong term psychiatric treatment for mother and child ŸNotify law enforcement & other medical facilities

E. D. Management of the Sexually Abused Child ŸSensitive interview and gentle exam ŸColposcopy may be helpful ŸDocument "in child's words" ; may need photos ŸCulture pharynx, vagina, rectum for gonorrhea, chlamydia ŸConsider VDRL, HIV serologies ŸPregnancy testing for older children ŸConsider prophylaxis with estrogen ŸConsider prophylactic antibiotics (not usually needed) or topical antibiotics for skin injuries ŸArrange counseling and check on siblings ŸNotify appropriate authorities

Adult configuration of the vagina diagnostic of abuse

Urethral prolapse which can be mistaken for abuse

Child Abuse Long Term Management ŸAssess safety for child to return home versus need for foster care ŸArrange for followup exam and / or counseling ŸVerify followup of lab tests results ŸPsychotherapy for parents ŸAttempt to reduce household stress ŸInvolve entire family in counseling ŸPlay therapy or special education for the child

Child Abuse Prevention ŸEducate patients and families about need for prevention ŸTelephone hotlines Ÿ"Crisis" nurseries ŸRegular home visits by nurses or social workers ŸSelf-help groups

Child Abuse Summary ŸRecognition is key E. D. function ŸChild protection is first priority ŸKnow ahead of time what personnel should be notified ŸAlso evaluate situation for siblings ŸArrange followup & counseling ŸAssist in prevention efforts
- Slides: 62