Emergency Contraception Jackie Paterson Consultant Chalmers Centre Emergency

























- Slides: 29
Emergency Contraception Jackie Paterson Consultant Chalmers Centre
Emergency Contraception
3 methods of Emergency Contraception
IUD insertion in young people • A Phase III, single-arm study of LNG-IUS 8, a low-dose levonorgestrel intrauterine contraceptive system (total content 13. 5 mg) in postmenarcheal adolescents. • Gemzell-Danielsson K 1, Buhling KJ 2, Dermout SM 3, Lukkari. Lax E 4, Montegriffo E 5, Apter D 6.
IUD • 303 12 -17 year olds had Jaydess inserted (narrower insertion tube than Mirena, but similar to 5 year copper IUDs like UT 380) • 303 of 304 candidates had a successful insertion • Most reported an easy insertion without significant pain • No perforations. No pregnancies
Availability of EC • LNG available free from pharmacies in Scotland to those aged 13 or older.
When to offer EC • • UPSI COCP-missed 2 or more active pills POP Cerazette >36 hours Sex before menarche-it is possible to conceive before periods start.
What to ask • • • LMP and cycle length to allow estimation of ovulation date Timing of ALL episodes of UPSI in current cycle Missed pills if using contraception Medication which may effect EC efficacy Ongoing contraception-is it required STI screening
Medication • Cu IUD – unaffected by drug use • LNG- liver enzyme inducing drugs or if stopped <28 days previously may reduce contraceptive effect. Advise giving double dose LG. (Not an issue with most recent PEPSE regime but is a problem with PI containing regimes) • UPA-Not to be used with liver enzyme inducing drugs or for 28 days afterwards. Not to be used with drugs that increase gastric ph.
Ovulation • Difficult to determine the precise timing of ovulation. • Highly variable especially if irregular cycle. • Conception is most likely to occur following UPSI on the day of ovulation or in the preceding 24 hours. • First 3 days of cycle – negligible risk of pregnancy
Follicular and Luteal Phase
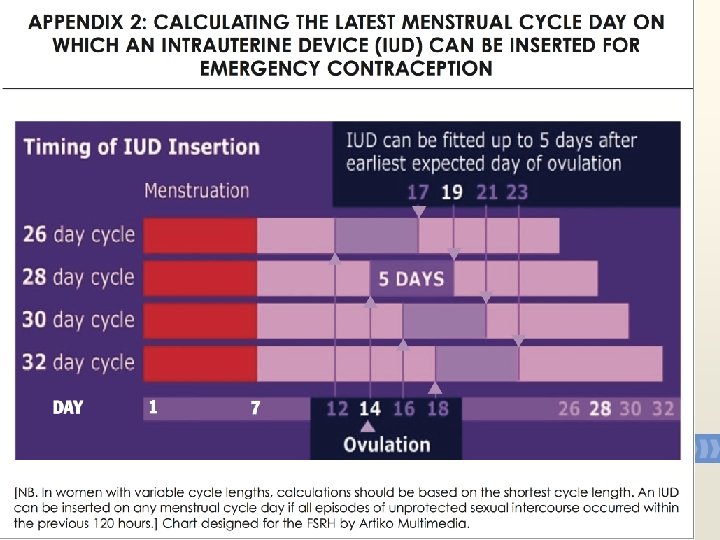
Timing from Ovulation to Implantation • Time from ovulation to implantation is between 6 -18 days • Therefore to ensure an IUD is inserted before implantation takes place the IUD must be inserted within 120 hours of first UPSI in a cycle or within 5 days of earliest estimated date of ovulation
How does EC work-IUD • Pregnancy begins at implantation not at fertilisation. -2002 Judicial Review • Cu IUD- Cu is toxic to ovum and sperm and works primarily by inhibiting fertilisation. Works immediately upon insertion • However if fertilisation has already occurred implantation is also prevented.
How does EC work-LNG • • LVG is thought to work by inhibiting ovulation Prevents follicular rupture/luteal dysfunction Must be taken prior to LH surge Then inhibits ovulation for 5 -7 days Any sperm present will become non viable in this time frame No better than placebo when given immediately prior to ovulation Not effective once fertilisation has occurred No congenital malformations
How does EC work--UPA • • • UPA Works by inhibiting or delaying ovulation for up to 5 days Can prevent ovulation after the start of LH surge But ineffective if given at time or after LH peak Endometrial effect? Prevents implantation No apparent effect on fetus if given after implantation has occurred
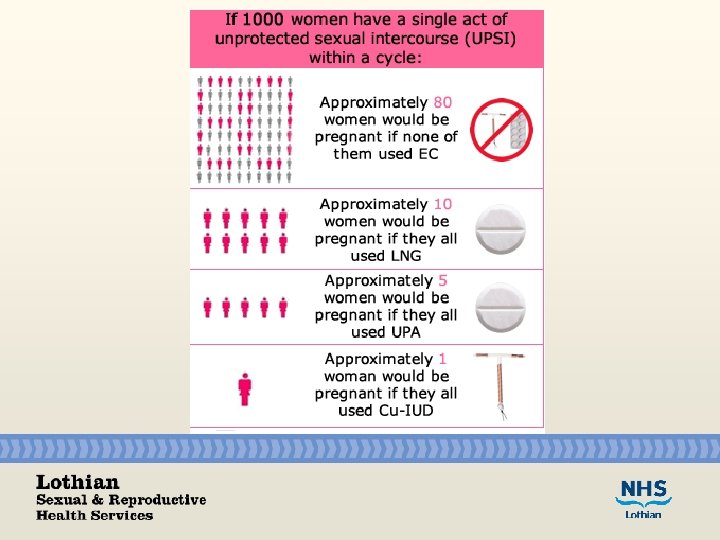
Effectiveness • Cu IUD failure rate 0. 1 % ref Cleland systematic review • UPA effective to 120 hours and pregnancy rate lower than with LVG. Failure rate 1 -2%. • LNG-licensed to 72 hours however some evidence suggests effective to 96 hours. Less effective than UPA
Side effects • Cu IUD-pain on insertion. NSAI, topical lidocaine, cervical block • LNG/UPA- bleeding may occur earlier than expected or later but within 7 days of expected time. • Nausea. Repeat dose if vomit within 2/3 hours of administration
More than once per cycle? • LNG- can be repeated in menstrual cycle if more than 1 episode of UPSI. • Can also be given to treat an episode of UPSI even if previous untreated episode within same cycle. • No evidence of teratogenicity
UPA • New CEU Guidance to be published soon! • UPA can be used more than once per cycle • After LNG-EC, UPA should not be given for about 5 days in case it reduces the effectiveness of the UPA. If LNG has been given within 5 days of a woman needing more EC, she should have more LNG. • If there is a risk of pregnancy from UPSI earlier in the cycle, but PT is neg, UPA can be given (no evidence of miscarriage or teratogenicity)
Pregnancy test • Consider before EC if: – uncertainty re LMP – Prior UPSI within cycle though only reliable >21 days post UPSI
STI screening • Offer NAAT testing for Gonorrhoea and Chlamydia. • Possible prophylactic abx cover pre IUD insertion
Ongoing contraception • If UPA given, no hormones for 5 clear days afterwards. • If recent hormone (eg missed pills, last taken 3 days ago) possible effect to reduce effectiveness of UPA, therefore consider LNG and immediate restart of pills (or ideally a better method as they had missed pills already!). • If important to quickstart (eg because won't turn up in 6 days for an implant) give LNG.
Quick starting contraception • LVG
EC QUIZ • Why should the Cu IUD always be offered? • How many times in a cycle can LNG be used? • What other medication can reduce the effectiveness of oral EC? • What advice would women taking enzyme inducing drugs be given? • How long after UPSI can a woman be sure she is not pregnant? • When will next period occur?
Summary • Consider IUD in young people requiring EC as: – Failure rate of 0. 1% – Insertion generally well tolerated by young people – Good method of ongoing contraception lasting 5 years. – Give ella. One prior to referring to Chalmers – ella. One should be used as first line oral EC unless taking enzyme inducers