Emergency Contraception Hormonal method PGD training Pharmacists South
 PGD training Pharmacists South Tyneside and Gateshead Dr Janet Gallagher")











 • Now (P) •")














 vs Ulipristal")
















- Slides: 51
Emergency Contraception (Hormonal method) PGD training Pharmacists South Tyneside and Gateshead Dr Janet Gallagher Assoc. Specialist Sexual Health Services Gateshead and South Tyneside 2019 Clarion Hotel Boldon
• • • Your training and preparation Acronyms used Audit findings pharm outcomes Calculating the risk of pregnancy Why EHC is needed Levonelle Deciding which Ella. One one to use Emergency IUCD Questions to ask, why and how Safeguarding, CSE Referral information Testing your understanding
Modules • Contraception • Emergency contraception • Safeguarding children and vulnerable adults • *AUTHORISED and current within last 3 years* • Declaration of competence • *Pharmoutcomes will confirm CPPE modules up to date. If not payment will not be given. * • *See Additional requirements*
Acronyms UPSI =unprotected sexual intercourse EC = emergency contraception LNG-EC= levonorgestrel 1. 5 mg QS= quick start of a suitable hormonal contraception • UPA-EC= ulipristal acetate 30 mg • Cu-IUD= copper intrauterine device • •
* • Highlights issues identified from audit of record keeping and CPPE modules stated as completed
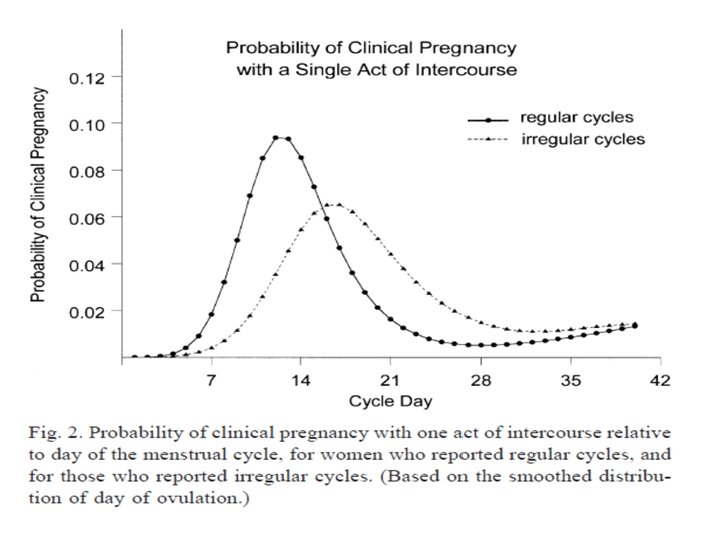
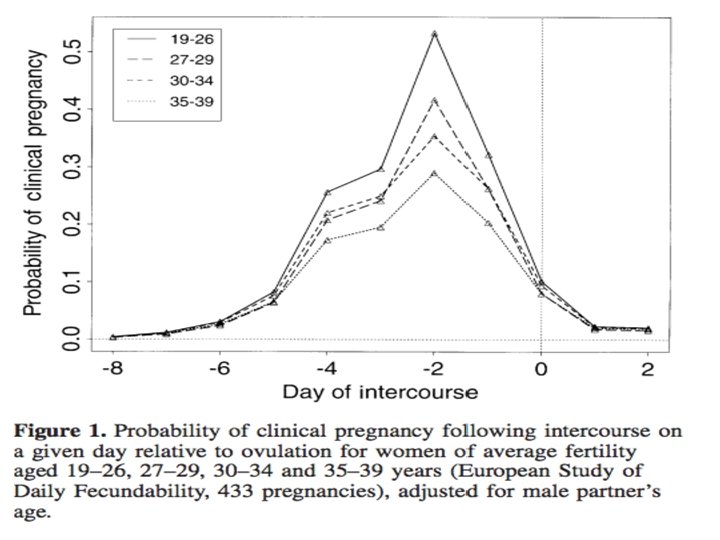
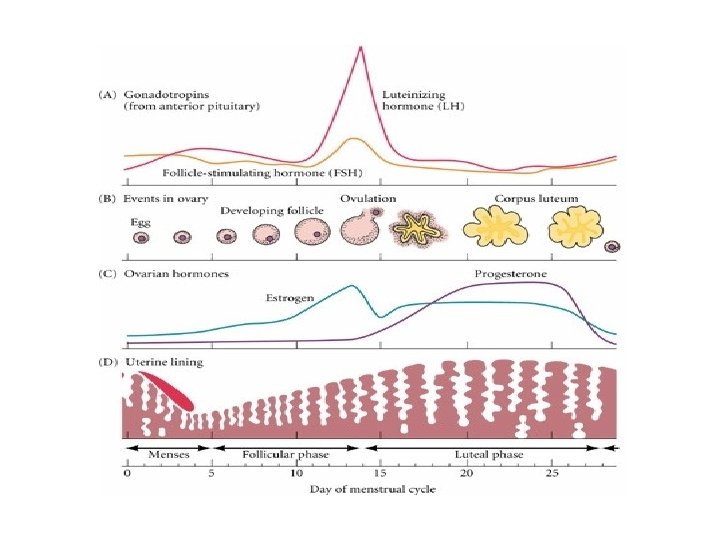
Risk of Pregnancy following UPSI • 2 -4% after a single act of UPSI anytime during the cycle • Highest risk if UPSI in 5 days before ovulation and that day of ovulation • No risk if before 21 days post natal • No risk days 1 -4 after TOP, miscarriage, ectopic • More irregular cycle , greater length of risk of pregnancy but less over all. • Can you calculate exact risk, science or art? • What about their weight ( BMI)?
Pitfalls in calculating risk • Sure of LMP- No woman has exactly 28 day cycle to the hour • Follicular and luteal phases are variable • Was there full ejaculation , did the condom slip of after • Has she taken hormones recently ( especially if UPA-EC considered) • How may times has she had sex • Variable natural fertility
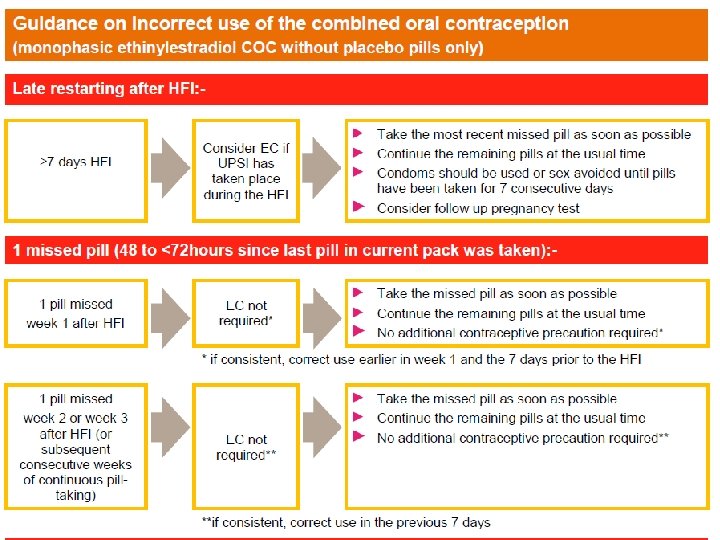
Why EC is needed • • UPSI Condom burst Missed or late contraceptive Out of date method
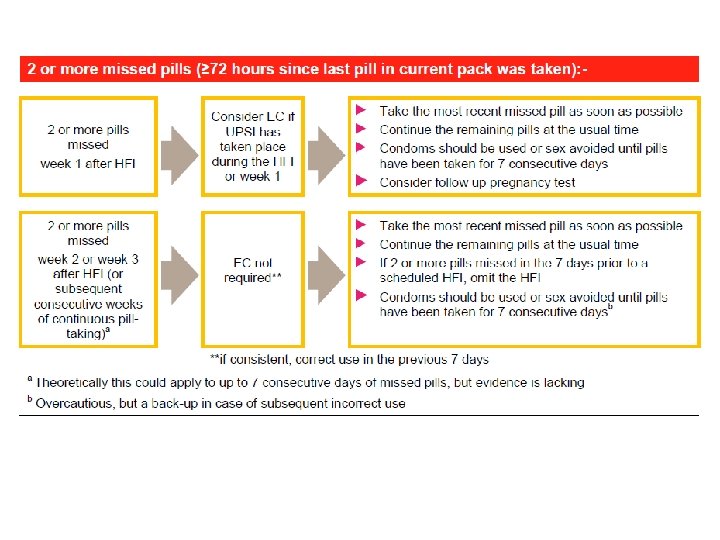
Progestogen only pills Missed or Late Previous pill taken <27 hours ago for LNG, NOR, < 36 hours DSG Continue pill taking as normal If not complied with this advice remember EHC needs Remember PIL states 7 days to work Previous pill taken >27 hours ago for LNG, NOR, <>36 hours DSG Take most recent pill missed Use condoms or NO sex for 2 days
Nexplanon user longer than 3 years IUD/ IUS use longer than prescribed length of use see following IUD’s last between 5 -10 years, IUS 5 years. Age at insertion changes length of use. Copper IUD’s inserted after 40 do not need replacing. IUS, Mirena, inserted after 45, stays in until not needed if women has no periods or until 55 Negligible risk between 5 -7 years of use IUS Negligible risk years 3 -4 for Nexplanon users If UPSI consider EC needs as if no method used
Late Depo Provera and Sayana Press and had UPSI Late by up to 14 days Late by > 14 days and UPSI after > 14 days since Depo due No need for EC Consider each episode of UPSI. Provide EC within 72 hours Be aware of lasting hormonal effect If multiple UPSI or > 72 hours Refer onward.
Hormonal IUS • If a woman is under 45 years at Mirena insertion and more than 7 years since insertion, replacement should be delayed until the woman has a negative pregnancy test at least 3 weeks after the last UPSI. May need EHC depending on when UPSI has occurred. Level of Levonorgestrel twice as high at 5 years than Jaydess at 3 • After 3 years for Jaydess users and 5 years for Kyleena users. They may need EHC if had UPSI
Licensed Methods in UK • Levonelle 1500 (introduced October 2005) • Now (P) • ella. One • Copper IUD
How effective is Levonelle • Only evidence of efficacy at 96 hours none at 120 hours PGD allows only up to 72 hours • Can be repeated in a single cycle • What are we treating, – Real risk – Anxiety • Both Levonelle and ella. One work to delay ovulation • Reduced effect if BMI >26 or Weight > 70 kg ( LNG EC) • UPA EC may be less effective BMI>30 or weight > 85 kg • Unlikely to be effective after ovulation
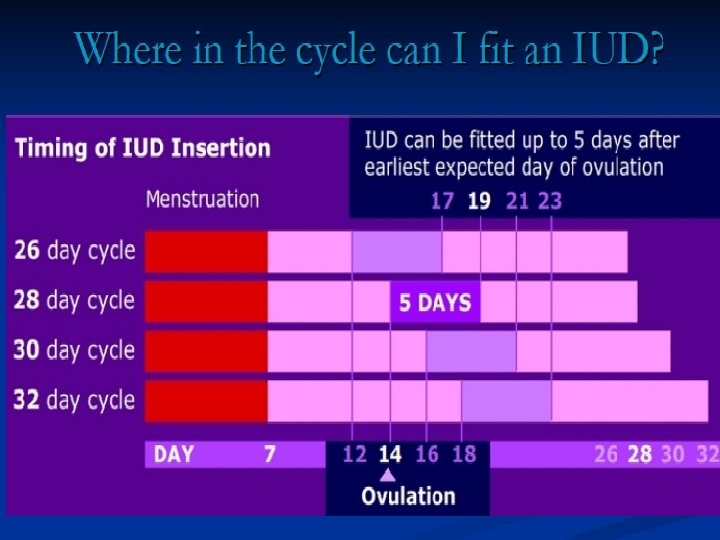
Specific points • Present within 72 hours even if previous UPSI ≥ 120 hours in the same cycle whether EC given or not. If UPSI > 21 days and has had no period, pregnancy must be excluded • Women choosing IUCD with no Contraindications for LNG EC or UPA EC should be given if the timing is correct.
• No more than 3 EC in same cycle whether LNG or UPA can be given • Amenorrhea for 2 years is and exclusion • Note about time of taking sooner the better • BMI important to consider dose • Genetic reasons and interactions noted GHD
BNF states specific cautions • With oral use as emergency contraception LNG • Active trophoblastic disease (until return to normal of urine- and plasma-gonadotrophin concentration)—seek specialist advice; past ectopic pregnancy; severe malabsorption syndromes
Caution UKMEC 2016 category 2 These conditions benefits outweigh risks • Current VTE on anticoagulants • Current or Past history of breast cancer • Inflammatory bowel disease( particularly if known to have significant malabsorption or small bowel resection following Chron’s) • Acute intermittent porphyria
In summary • It is far safer to give Levonelle than the risk of a pregnancy for women with medical conditions.
UPA-EC More effective than LNG-EC consider weight! Works before LH surge Up to 120 hours from UPSI Effectiveness reduced in takers of enzyme inducing drugs ( and for 28 days after stopped taking) • Not suitable for women who have severe asthma controlled by oral steroids • Unknown significance of PPI’s on UPA-EC. ? Lower level of UPA (when used for other reasons at higher doses) shown to be altered by esomeprazole • •
News highlights • Women not wanting to become pregnant should be offered EC after UPSI on any day of natural cycle ( even though it may not be very effective) • If chosen CU IUD then oral EC should be given in case IUD can not be inserted or woman changes mind or does not attend. • No disruption of an existing pregnancy and not associated with fetal abnormality. • History can be changed by patients.
In Summary for oral EHC UPA-EC can be used again in same cycle after further UPSI LNG-EC can be used again in same cycle after further UPSI If taken UPA-EC, LNG-EC should not be taken in next 5 days If taken LNG-EC , UPA-EC could be less effective in 7 days after taking. Remember other hormonal methods • After LNG-EC contraception can be started as a QS method and should be encouraged with condoms or abstain until this method is effective • After UPA-EC wait 5 days before starting hormonal contraception then wait until effective • See decision making tree Appendix 3 • •
• If Cu IUD is not chosen consider UPA-EC as first line EC for UPSI within last 120 hrs and or if likely to have occurred in 5 days prior to and including estimated day of ovulation. HIGH RISK • Breast feeders should express milk and discard for 1 week after taking UPA-EC • Breast feeders. . inform that limited evidence that LNG-EC has no adverse effect in breast feeding or infants • Inform that possible that higher weight or BMI could reduce the effectiveness of oral EC , particularly LNG-EC
Emergency IUCD • • • Most effective method of EC Not chosen by all Cover more UPSI effectively than oral methods Can remain in for future contraceptive needs Devices last 5, 10 and 12 years
Fig 1 Window of action of different emergency contraceptive methods in relation to ovulation. Prabakar I , Webb A BMJ 2012; 344: bmj. e 1492 © 2012 by British Medical Journal Publishing Group
Making decisions Algorithms for Emergency Contraception FSRH guidance 2017 Copper IUCD vs Oral EC ( adapted for pharmacists) Currently < 120 hrs since UPSI YES Additional UPSI > 120 hours ago? Yes or unknown Currently ≤ 5 days after earliest likely date of ovulation? Yes No Offer Cu IUD If not acceptable offer oral EC* and discuss suitable on-going contraception No or unknown Offer Cu IUD If not acceptable offer oral EC* and discuss suitable ongoing contraception Unknown NO ie > 120 hrs Currently ≤ 5 days after earliest likely date of ovulation? Yes Offer Cu IUD Oral EC* unlikely to be effective Refer onward for suitable quick start contraception Consider pregnancy test if UPSI this cycle > 21 days ago Offer oral EC* and discuss suitable on-going contraception No or unknown Cannot insert Cu IUD Oral EC unlikely to be effective Refer onward for suitable quick start contraception Currently ≤ 5 days after earliest likely date of ovulation? Yes Offer CU IUD If not acceptable offer oral EC* and discuss suitable ongoing contraception No or unknown Offer oral EC* and discuss suitable ongoing contraception See next slide for oral EC choices Note that there is no evidence that oral EC is effective if ovulation has already occurred
Decision making for oral EC Levonorgestrel E 0 C ( LNG EC) vs Ulipristal Acetate EC ( UP-A-EC) adapted for PGD The Cu IUD is the most affective form of EC. IF criteria for insertion of a Cu IUD are not met , cannot be arranged within time or a Cu IUD is not acceptable to a woman, consider Oral EC Last UPSI < 72 hours ago? No or unknown Yes UPSI likely to have taken place ≤ 5 days prior to the estimated day of ovulation? No Yes or unknown BMI > 26 or weight > 70 kg No Last UPSI < 120 hours ago? Yes or unknown No Oral EC unlikely to be effective Reconsider Cu IUD if currently within 5 days after likely ovulation Or QS contraception NOTETHAT ORAL EC IS UNLIKELY TO BE EFECTIVE IF TAKEN AFTER OVULATION LNG-EC + immediate QS Or UPA-EC + start contraception after 5 days Double (3 mg) LNG-EC + immediate QS Or UPA-EC + start contraception after 5 days Reconsider Cu-IUD if all UPSI within 120 hours or if currently within 5 days after likely ovulation If UPA-EC not suitable LNG-EC + immediate QS UPA-EC + Start contraception after 5 days LNG-EC unlikely to be effective Reconsider Cu-IUD if all UPSI within 120 hours or if currently within 5 days after likely ovulation
Who is it for? • *Women / girls 14 and over NOT for 13 year olds* • *Confirm Fraser competencies for 14, 15 year olds* • Consider Women 16 years and older with learning difficulties or mental capacity problems • *Consider child protection concerns* • Domestic or emotional abuse • *Child sexual exploitation* • Remember professional curiosity
Confidential interview and advice • However……sometimes………. . • Inform carefully that you may have to contact someone else and give them some information if they provide any information causing concerns about their safely or the safely of others • Aware that sex under 13 is a sexual offence and has to be reported, Sex under 16 is currently illegal however this is judged as confidential if there are no features that cause concern.
*Fraser checks for under 16’s* • Is a parent or guardian present? • If no parent/ guardian present, check who is with the under 16. • Are they mature enough to Understand the advice given and its implications • Try to Persuade them to talk to a parent or guardian about relationship and sexual health advice. • They are likely to continue being Sexually active with or without the advice • Without this advice or treatment their physical or mental Health would suffer • It is in their best Interest that treatment of advice is given without parental consent. • Remember UPSHI
After care and follow up Give written and verbal information on: • Efficacy, Side-effects • Future contraception choices • STI screening where appropriate • Pregnancy test if period> 5 days delay or lighter, or no withdrawal bleed in Pill free week ( if on COC) • Chlamydia screening…. . Available NOW from all C&SH services for under 25’s and some GP’s and for yourselves • Changes coming in Gateshead • Taking tests only Urine for male and Female………… Risks Missing diagnoses
Timing of next period • The next period should arrive ± 3 days of expected date. • Periods and bleeding may be irregular especially if other EC taken within the cycle • More times taken in any cycle, greater disruption of menses with less effectiveness of subsequent EHC
Future contraception • Abstinence or Effective contraception for the rest of the cycle • REMEMBER LASTING AND REVERSIBLE CONTRACEPTION LARC • EC use after “Missed pills” resume pills within 12 hours of taking EC ( not UPA-EC) • Discuss initiating a regular method of contraception • Refer to a service that provides all methods for choice • Quick start of methods after emergency contraception except Depo Provera
Management of a request for Emergency Contraception Where does it take place? *Documenting on pharmoutcomes * directly ( not paper) Confidentiality to be ensured No conversations overheard No added embarrassment Privacy and dignity
What and why do we ask? - AIMS • Check that they are not already pregnant • Identify level of risk of pregnancy, drugs or conditions that make EC less effective or increase health risks • Failure of previous contraceptive use and plans for the future • Determine risk of STI, (especially if under 25’s recent partner changes). Consider multiple partner history • Consider any issues of non- consensual SI • Legal guidance for Under 16’s • Consider child protection referral needs • Consider CSE
For advice. • Contact numbers safeguarding advisors • South Tyneside 0191 2831374 • safeguarding. sotw@nhs. net • Gateshead 03000031918 • hdftgateshead@nhs. net
For referral where child lives Contact numbers ST office hours 0191 424 5010 ST out of office ours 0191 4562093 During office hours (Monday - Thursday, 8: 30 am 5 pm and Friday, 8: 30 am-4: 30 pm) (0191) 433 2653 or R&ADuty@gateshead. gov. uk • Gateshead out of hours call emergency Duty team 0191 4770844 • Sunderland 0191 5205560 or 5205552 out of hours • Durham 03000267979 • •
Worried about something else • • • Gut feelings Think < 13 ( statuary rape, cannot consent) Signs of self harm Seen them before Remember girls or women of any age may be affected by domestic abuse or violence.
Some Signs, What may raise suspicions • • • May smell of alcohol Lack of eye contact and engagement Unexplained bruising, scalds, marks Have expensive phones, gifts , new possessions Should be at school ( so now missing from school) Have older boyfriend or girlfriend with them Staying with friends, sleeping on sofas( no home adress) Behaving aggressively Demanding inappropriately
Those at risk of Child sexual Exploitation • • • Missing from home or care Involved in offending Drug/alcohol abuse Repeat STI, pregnancies, TOPS Mental health problems, self harm, physical injuries Gifts from unknown source Changes or inappropriate appearance or behaviour Evidence of bullying Estranged from family Recruiting others into exploitative situations
Contact CSE or Child protection • If under 13 legally cannot consent to SI so is classed as sexual offence. • Ring 999 • What time of day and who is available
Referral Pathway South Tyneside onward contraception. Emergency IUCD or advice • South Tyneside 0191 4028191 all services to one location Palmer CH • Reception open in clinic times • C&SH service provides all methods. • Some GP surgeries insert IUD’s (5) South Tyneside • ( May not have appointment for emergency IUCD) • Some GP surgeries insert Nexplanon (5) • C&SH service open 6 days each week with • Emergency IUD insertion available each day Mon Fri
Referral Pathway Gateshead for onward contraception and Emergency IUCD Gateshead 0191 2831577 clinic reception Emergency IUCD Mon- Fri C&SH service open 6 days per week GP surgeries inserting IUD and inter-practice referrals but may not have appointment for emergency • C&SH service provides all methods. • Some GP surgeries insert Nexplanon • C&SH service open 6 days each week • •