Electrolyte Disturbance Dr Alaa Mohammed Fouad Mousli Surgical

Electrolyte Disturbance Dr. Alaa Mohammed Fouad Mousli Surgical Demonstrator
 Neoplasm Drugs (Crbamazepine , cytoxan,")
Hyponatremia Causes of SIADH Infections (meningitis TB Pneumonia ) Neoplasm Drugs (Crbamazepine , cytoxan, tricyclic ) Postoperative Subarachnoid haemorrhage

Hyponatraemia Sever when below 120 mmol/l Symptoms depend on severity and rapidity of decline in serum sodium Chronic hyponatraemia is less symptomatic but should be corrected with great caution

Hyponatremia symptoms May be asymptomatic Weakness lethargy dizziness and decreased concentration Seizures confusion and even coma can be seen in sever cases particularly if developed quickly
 *(wt*.")
Hyponatremia Deficient can be calculated by ( Desired Na – Serum Na ) *(wt*. 6) Correction should at a rate of 1 -2 mmol/l Correction should be to mild hyponatremia Central pontine myelonysis is mainly seen in alcoholics

Hyponatremia investigations Plsma osmolality Urine Na concentration

Hyponatremia treatment Normal saline is indicated in volume depletion Diuretics induced Water restriction indicated in SIADH Oedema renal failure Hypertonic saline indicated in sever symptomatic hyponatremia

Hyponatremia treatment of SIADH Acute Water restriction Hypertonic saline Loop diuretics Chronic Water restriction Loop diuretic Demeclocycline
 Renal loss GI losses Hypothalamic disorders DI")
Hypernatremia causes Water loss (sweating Burns ) Renal loss GI losses Hypothalamic disorders DI

Hypernatremia symptoms Mainly neurological Lethargy weakness and irritability are early symptoms which can progress to seizures coma and death Symptoms are more with acute oncet

Hypernatremia treatment Dextrose infusion
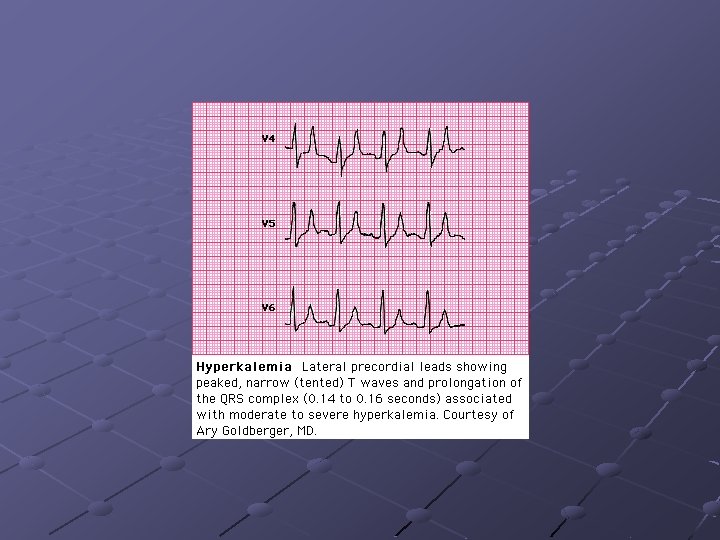
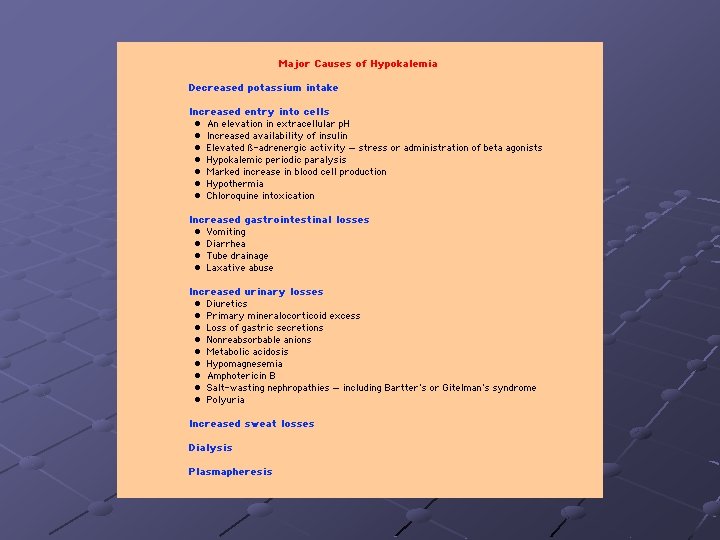

Hpokalemia symptoms Weakness lethargy If chronic may lead to polyuria Can lead to sever alkalosis May trigger cardiac arrhythmia in patients with ischemic heart disease or recent myocardial infarction

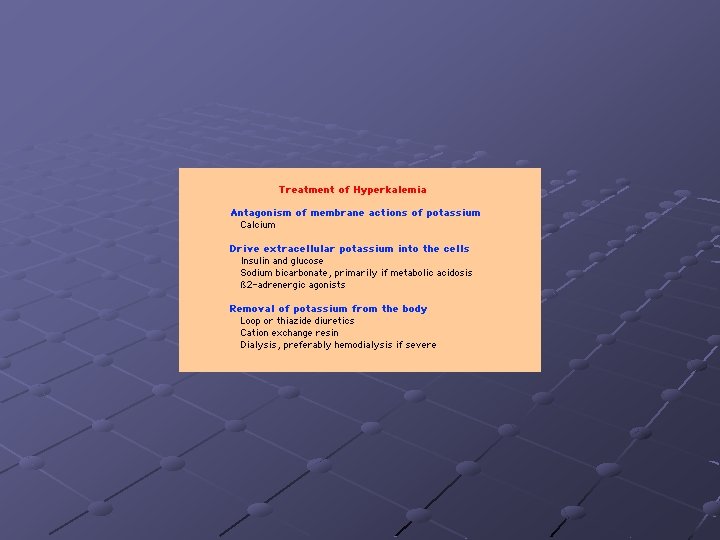
Hypokalemia Treatment K supplement either oral or intravenous K deficiency can not be calculated Usual requirement in the range of 60 m. Eq/24 hours Rapid KCL infusion is fatal IV KCL can be given in a maximum rate of 10 – 20 m. Eq/h this may require a central line
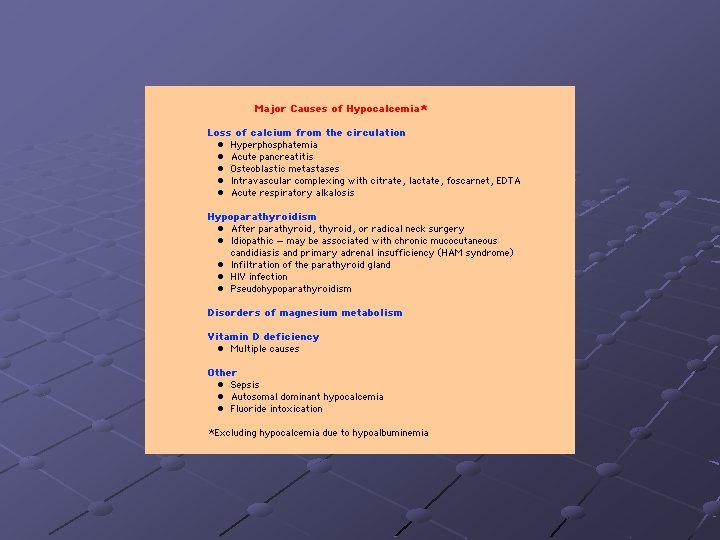
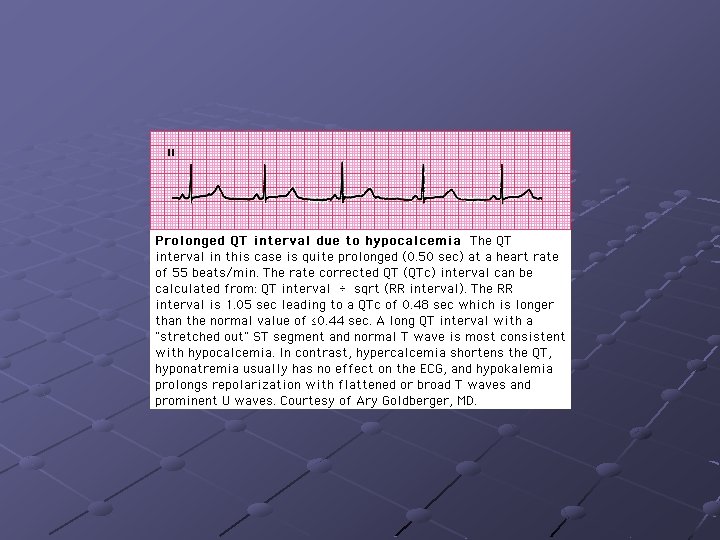

Hypocalcemia treatment Calcium and vitamin D supplement If symptomatic then intravenous Ca gluconate should be used ( Ca <0. 7 mmol/l ) Mg should be checked since if hypomagnesaemia present hypocalcemia can not be corrected
 Tubular disorders")
Hypomagnesaemia causes Diuretics Alcohol Hypercalcemia Nephrotoxins (cisplatinum Amphotiricin B) Tubular disorders
- Slides: 30