ELBOW CONTRACTURES ARTHROSCOPIC RELEASE Nguyen Trong Anh et

ELBOW CONTRACTURES ARTHROSCOPIC RELEASE Nguyen Trong Anh et al

INTRODUCTION ELBOW CONTRACTURES: • Extra/intra-articular causes • Most contractures are mild, involve terminal extension, not significantly alter function. • Certain athletes complain lack of terminal extension after performance.

• Functional arc of motion: 30 -130 deg. • Arc of motion less than 100 deg. not well tolerated. • Functional use of hand depends on the elbow. -50% loss of elbow motion 80% loss of function to upper extremity. • Loss of elbow flexion not well tolerated. Females: inability to style their hair, make-up. Males: inability to fix a tie, shave

CAUSES • • Trauma: acute, chronic. Heterotopic ossification. Osteoarthritis. Inflammatory arthritis. Post-op scars. Infection. Burns.


Intra-articular finding lesions • • Capsular contractures Osteophytes: olecranon, coronoid. Loose bodies. OCD capitellum. Chondromalacia radial head. Adhesions Synovitis.
/lateral(Hastings) approach to anterior and posterior compartment. Effective with extra-articular")
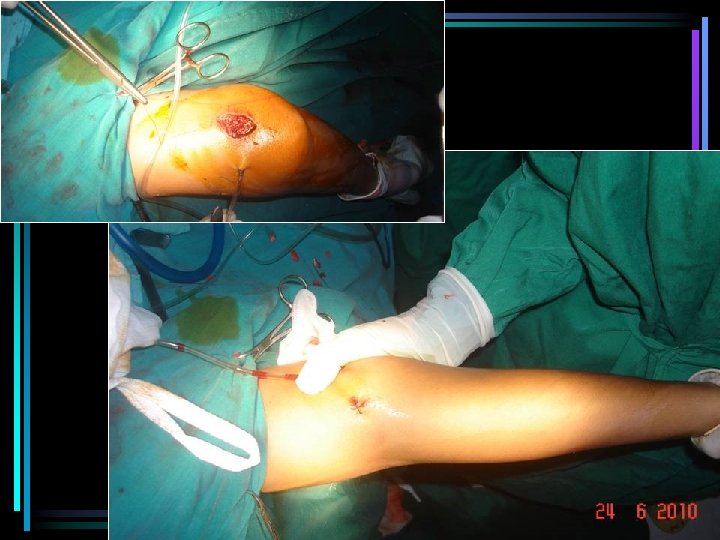
Surgical treatment: 1. Open: medial(Hotchkiss)/lateral(Hastings) approach to anterior and posterior compartment. Effective with extra-articular contracture Technically demanding, significant morbidity, prolonged rehab. 2. Arthroscopy: Anterior capsular release, loose body removal, osteophyte excision, olecranon fossa débridement to reach functional ROM. Faster, easier, more effective (The most technique and experience demanding) 3. Combined technique: arthroscopy anterior compartment. Miniopen with tenotomy posterior

Arthroscopic release: • Timmerman 1994: 29 mo f/u: 79% good-excellent. • Phillips 1998: 10 DJD, 15 post trauma 18 mo f/u: 25 pts increase ROM, decrease pain. • Kim 1995: 25 pts 25 mo f/u: 92% pt satisfied. • Savoie 1993: 22 mo f/u: all satisfied.

ELBOW ARTHROSCOPY: • 1930 Burman used arthroscopy to study elbow joint on cadaver. • Late 1970 s: diagnostic and treatment elbow arthroscopy • 1988, elbow arthroscopy only 0. 77% in 10. 000 arthroscopy cases small joint capacity and dangerous proximity to neurovascular structures

• Late 1990 s until now: more understanding of portals, surgery techniques and pathology, elbow arthroscopy has significantly progressed in diagnosis and treatment of many elbow lesions. • AAOS(2003): 7% orthopedic surgeons perform elbow scope.

Common applications: • Loose body removal. • Synovitis debridement. • Osteochondral lesion treatment. • Assessment and treatment of undiagnosed or chronic elbow pain. • Spur or osteophyte excision. • Arthroscopy-assissted management of fractures around elbow joint. • Stiff elbow release
 with: • Capsular contractures. • Bone")
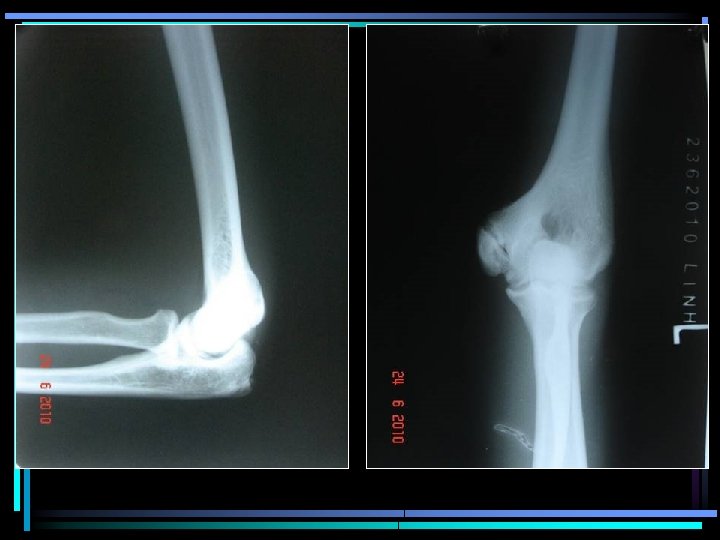
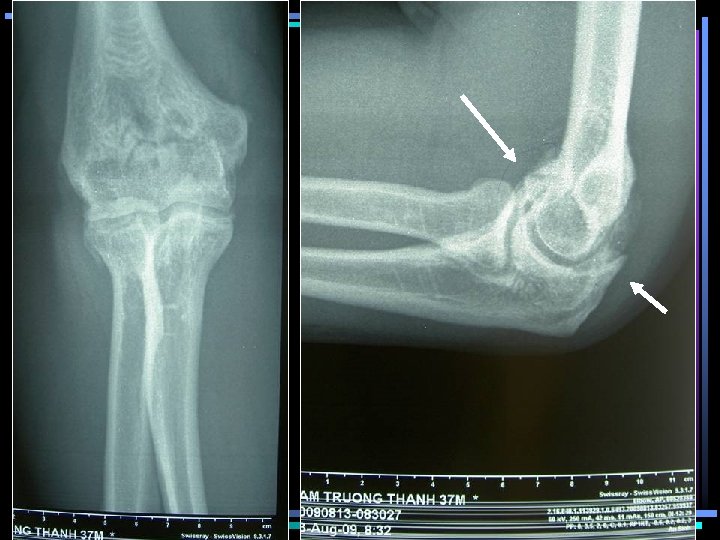
Indication 1. Loss of functional ROM (30 -120) with: • Capsular contractures. • Bone impingement: Osteophyte: ocleranon, coronoid process • Combined lesions: OCD, chondromatosis, synovitis, loose bodies… Failure to improve w physical therapy. 2. Pt requires specific ROM for occupation. (sport players)

Contraindication • Active infection • Bone/fibrous ankylosis prevents safe introduction of arthroscope. • Previous surgery alters normal anatomy, joint congruity, extra-articular contractures. • Intracapsular space severely constricted capsular distention NV damage risks.

History • • • Chief complaints: ROM limit, pain. Trauma? Repeated heavy use of arms. Sports. Mechanical impingement, pain at extremes of motion (ext>flex) or heavy carry.

Physical exam • Skin scars, burn. • ROM • Soft /hard end points soft tissue constraint/bone impingement. • Painful arc or extremes joint incongruity/degeneration or bone impingement. • Neurovascular exam: ulnar nerve(pathology/location) Xray, CT scan, MRI

MATERIALS 06/2005 - 10/2010: 36 cases • 15 post-trauma. • 7 sport related. • 1 radial head malunion. • 1 previous intercondylar fracture surgery. (27 yr) • 6 loose bodies. • 4 OA. • 1 RA. • 1 gout

OR SETUP • Scope: 4 mm, 300 • Water pump w 4050 mm. Hg. • Shaver and burr blades: 4 -5 mm • Arthrocare radiofrequency. • Grasper, cutter

PATIENT SET-UP • • General anesthesia Regional block. EUA for p. ROM, ulnar n. Prone/ LDP w free arm on holder. Supine? • Tourniquet. • All bone prominence padded.

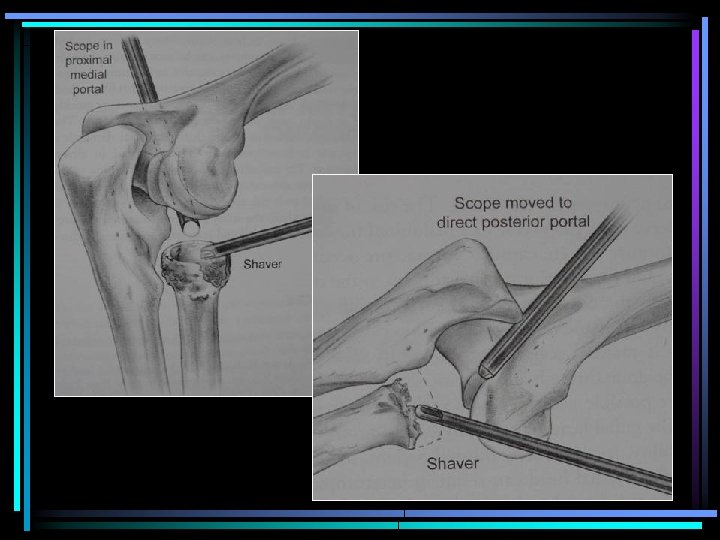
PORTALS 1. Anterior: 1. Proximal lateral 2. Proximal medial 2. Posterior 1. mid / direct lateral. 2. Central posterior 3. posterolateral

Cutaneous nerve branches around elbow hazardous mine traps!!!!

Proximal medial

Proximal lateral

Mid lateral

Straight posterior

Posterolateral

Technique procedures • Tourniquet. • Initial join distention w 20 -30 cc NS. • Proximal medial portal: Evaluating whole anterior compartment. • Posterolateral/ direct posterior: Evaluating whole posterior compartment.

Surgical steps Anterior compartment: • Adhesion release. • Loose body removal. • Coronoid process and fossa spur resection. • Capsular incision/resection from lateral to medial, to visualize brachialis fibers. Posterior compartment: • Ocleranon, fossa spur resection (± miniopen w osteotome). • Medial/lateral column impingement check • Post capsular, medial and lateral gutter release.

+ Tourniquet time !!! + Closed drainage Post op: • Ice scrubbing. • Nerve deficit and compartment syndrom evaluation. • Early motion exercises as tolerated.

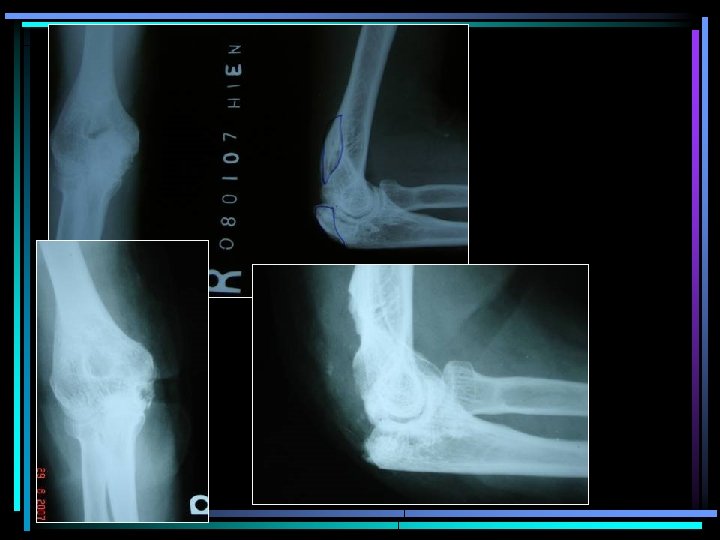
CASE 1

CASE 2


F/U 6 mo


CASE 3

CASE 4


CASE 5 • M, 38, 5 y injury, elbow pain. ROM limit.

PRE-OP POST-OP


CASE 6


CASE 7 F, 56 yo, 7 mo fall injury ROM: pre-op: 60 -110 post-op: 45 -160

CASE 7 M, 38 yo, 6 mo of elbow arthritis

PRELIMINARY RESULT >6 mo F/U • 24 Patients satisfy w surgery: no pain, ROM improvement. • 2 nerve deficit. (Ulnar/ Radial n)

CONCLUSION • Elbow arthroscopy allowed to perform accurate diagnosis and appropriate treatment to most intra-articular pathologies causing elbow pain and stiffness. • Significant ROM improvement, less morbidity, earlier postop rehab are provided.

• Combined arthroscopic and miniopen releases are effective in selective hard cases • Anatomy comprehension and experience are required to avoid neurovascular structure damage and improve long term results. • Good results need selective indication, early and long-term postop rehab.
- Slides: 55