EL CORAZN EN LA ESCLEROSIS SISTMICA JOS LUIS







± pulse CYC* If:")










- Slides: 45
EL CORAZÓN EN LA ESCLEROSIS SISTÉMICA JOSÉ LUIS CALLEJAS UNIDAD DE ENF, SISTÉMICAS H. NUEVO SAN CECILIO, GRANADA
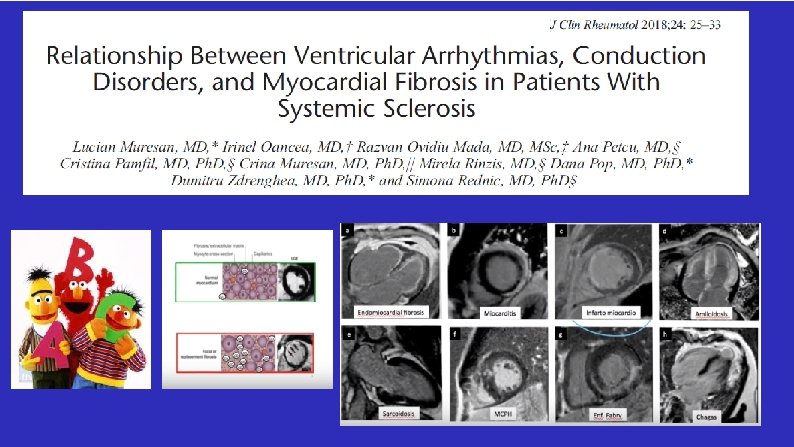
Myocardial involvement Atherosclerosis Arrhythmias and conduction defects Pericardial involvement SSc-related endocarditis
DARTH CORTICOIDE
LA ES, EL DERRAME PERICÁRDICO Y LA TOMA DE CORTIS
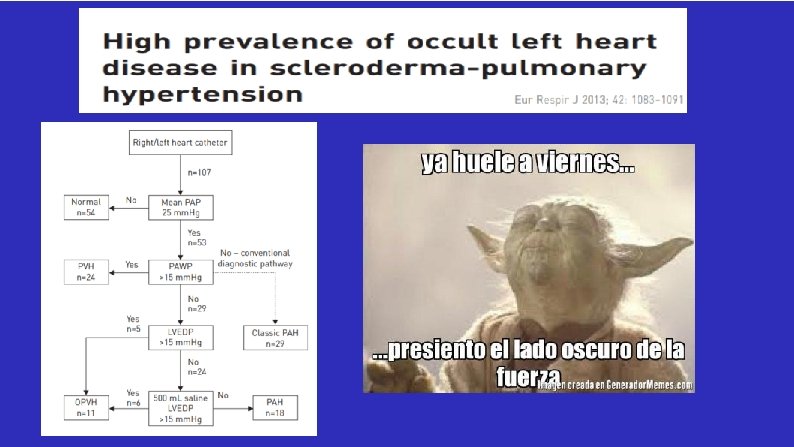
PACIENTE CON ESCLEROSIS SISTÉMICA CON DISNEA ¿ Tendrá una HP? . . BNP, DLCO, ecocardio-Doppler reposo/esfuerzo/CCD reposo/CCD esfuerzo ¿Tendrá una insuficiencia cardíaca? . . . BNP/ecocardiograma
DISFUNCIÓN SISTÓLICA V. I
ANTE LA DUDA…
The working group recommends: - moderate dose CS (<15 mg/ day)± pulse CYC* If: - a myocarditis or other features of SSc-CM are evident - moderate�severe LV dysfunction (not secondary to atherosclerotic heart disease) - and life-threatening cardiac arrhythmias *
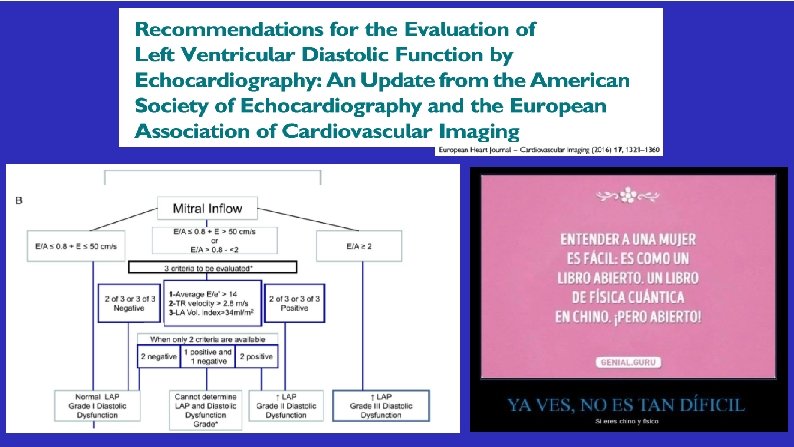
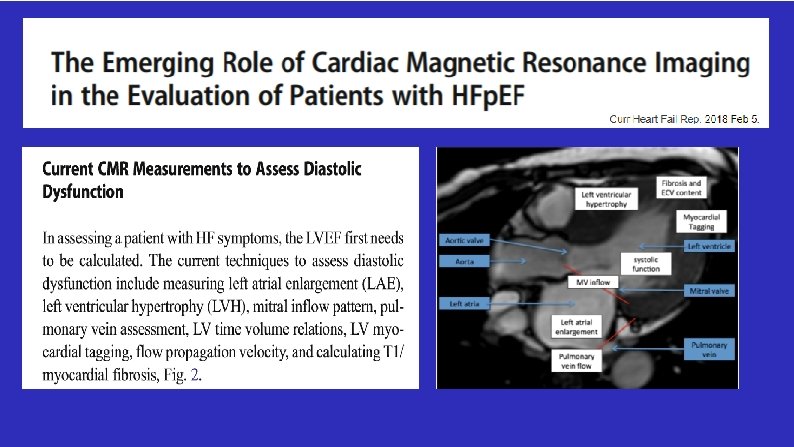
DI SFUNCIÓN DI ASTÓLICA
LA DISFUNCIÓN VENTRICULAR ES CAUSA DE DISNEA
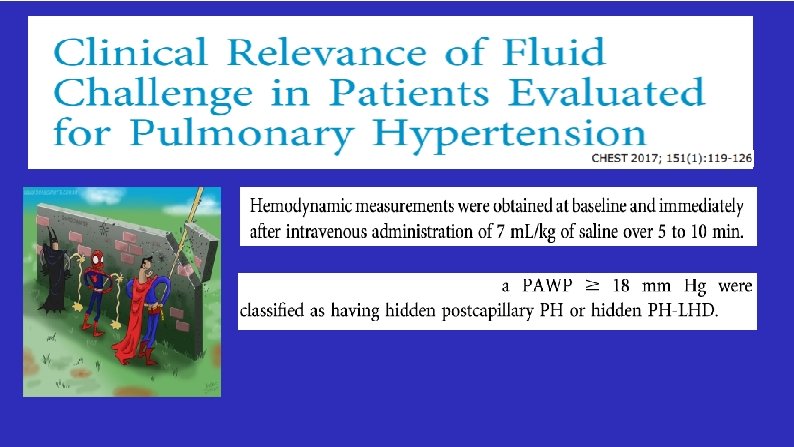
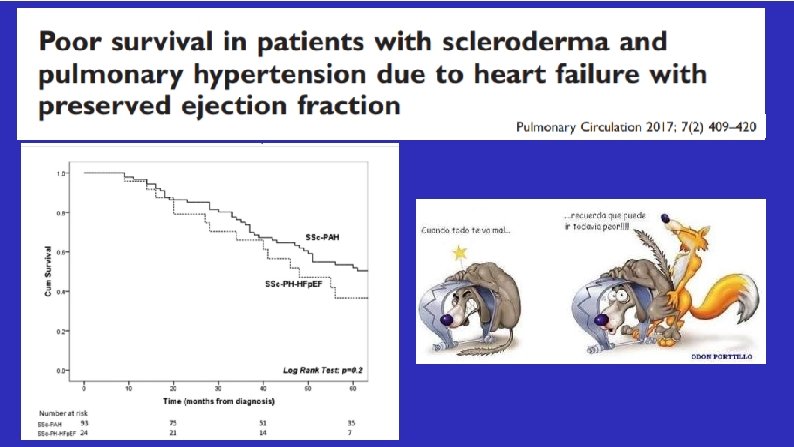
v - Patients with postcapillary PH were defined as having a DPG of <7 mm Hg - Combined PH were defined as having a DPG of ≥ 7 mm Hg However, randomized trials are needed in SSc patients with an elevated PAWP to determine the clinical utility of treatment with PHspecific medications.
HACER POR HACER
-CMR was performed early after diagnosis in 78 treatment-naïve CTDs
CMR was performed early after diagnosis in 78 treatment-naïve CTDs
- 7/62 with d. SSc and 2/20 with l. SSc, - In all 9 SSc patients, 3/3 indices were although they had no cardiac positive for myocarditis symptoms/signs, were positive for myocarditis 1. Seguir con tropos, BNP y ecocardio 2. Repetir RM a los positivos en 1 año 3. Repetir RM a todos, ya que la miocarditis puede ser, de hecho era, asintomática 4. Irme a Lago Louis una semana, si es posible en buena compañía 5. Poner tratamiento con IS
CMR was performed in 16 consecutive patients with SSc, of recent onset, immediately after the diagnosis Stress perfusion defects of left ventricle were detected in six out of 16 (37. 5%)
HACER POR HACER POS HABRÁ QUE HACER. PROPUESTA ESTUDIO PARA AADEA.