Efficacy and safety of apixaban compared with warfarin

Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: observations from the ARISTOLE trial Ambulatory Journal Club Akika Ando, MD R 1, Internal Medicine 2014/Aug/20

Outline • • My patient-case presentation Clinical question Introduction/Background information on topic Journal article Critical Appraisal Limitations Clinical question revisited Conclusion

My Patient Pt is a 73 yo Hawaiian M with PMH of HTN, morbid obesity, depression, severe OSA, asthmatic bronchitis, chronic atrial fibrillation on Coumadin, CAD s/p CABG 2005 here to reestablish care.

【PMHx/PSHx】 - HTN - Morbid obesity - Depression - Severe OSA - Asthmatic bronchitis - Chronic atrial fibrillation on Coumadin - CAD s/p CABG 2005 【FHx】 Unknown, He was adapted 【Social Hx】 He was born and raised in Oahu. Single. Tobacco:Never smoked Et. OH:occ 1 glass of beer/week

【Meds】 - Lasix 40 mg 1 tab daily - Atorvastatin 40 mg 1 tab daily - Losartan 25 mg 1 tab daily - Aspirin 81 mg 1 tab daily - Carvedilol 3. 125 mg 1 tab BID - Advair 1 puff BID - Proair 2 puffs prn - Spiriva 1 cap daily 【Alleries】 Lisinopril (rash) He did not want to take Coumadin anymore for frequent monitoring. We were planning to start Apixaban… He was concerned about new medication because of his age…
, does the efficacy and safety")
My question is… In patient with atrial fibrillation (AF), does the efficacy and safety of apixaban compared with warfarin differ by patient age?
")
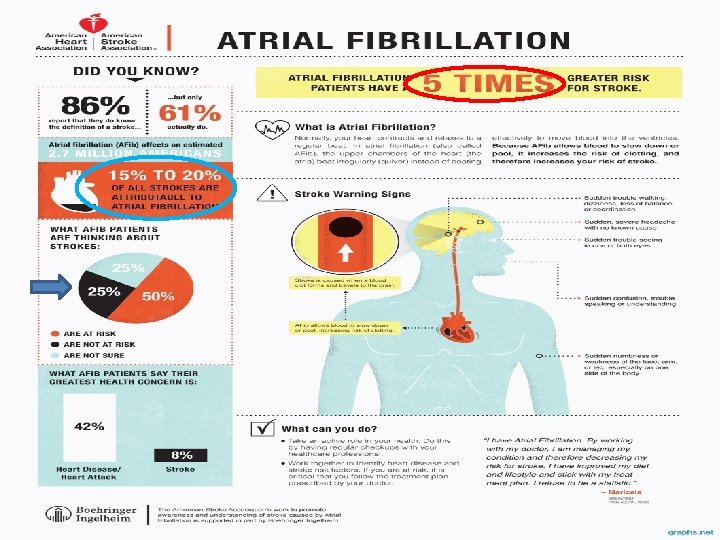
What is Atrial fibrillation? • Atrial Fibrillation (also known as AFib or AF ) is the most common arrhythmia. • It affects more than 2. 5 million American adults and 4. 5 million people living in the European Union. • It accounts for approximately one-third of hospitalizations for cardiac rhythm disturbances.

Afib Management
 is an anticoagulant for the treatment")
What is apixaban? • Apixaban (BMS-56224701, tradename Eliquis) is an anticoagulant for the treatment of venous thromboembolic events. • It is a direct factor Xa inhibitor.

How does apixaban work?

They did not discuss the efficacy and safety compared with warfarin by patient age. In patients with atrial fibrillation, apixaban was superior to warfarin in preventing stroke or systemic embolism, caused less bleeding, and resulted in lower mortality.

Objective • The risk of stroke in patients with atrial fibrillation increases with age. • In the ARISTOLE trial, apixaban when compared with warfarin reduced the rate of stroke, death, bleeding. • To evaluate these outcomes in relation to patient age

Methods Design: Prespecified subgroup analysis of a randomized controlled trial Blinding: blinded (patients, clinicians, outcome assessors, data collectors, data analysis) Follow-up period: Median 1. 8 years Setting: 1034 centers in 39 countries (Between Dec/19/2006 and Apr/2/2010)
 who had atrial fibrillation")
Methods Patients: 18, 201 patients (65% men(median age 70 y) who had atrial fibrillation or atrial flutter - 30% <65 y - 39% 65 to <75 y - 31% ≧ 75 y

Pt Population Inclusion Exclusion • at least ≧ 1 CHADS 2 risk factor for stroke or systemic embolism • cardiac failure • HTN • age>75 y • DM • previous stroke or transient ischemic attack • Previous intracranial hemorrhage • Any stroke →within 7 days before random assignment • Dual antiplatelet therapy with ASA and clopidogrel at study entry
), or warfarin adjusted to")
Intervention • Apixaban, 5 mg BID, (+ warfarin placebo (n=9120)), or warfarin adjusted to achieve a target international normalized ratio of 2. 0 to 3. 0, plus apixaban placebo (n=9081). • Apixaban dose was reduced to 2. 5 mg BID in patients with ≧ 2 of age ≧ 80 y, body weight ≦ 60 kg, and serum creatinine level ≧ 133μmol/L(≧ 1. 5 mg/d. L)

End points • Primary efficacy outcome - stroke - systemic embolism • Secondary efficacy outcome - all cause mortality
major")
End points • Primary safety outcome - international society on thrombosis and haemostasis (ISTH)major bleeding • Secondary safety outcome - intracranial and total bleeding

Patient characteristics

Patient characteristics

Patient characteristics

Stroke Prevention in Atrial Fibrillation: Latest Clinical Trials and Guidelines. Luciana Armaganijan et al. Pharmaceuticals 2012, 5, 384 -397

The HAS-BLED score offers useful predictive capacity for bleeding. One point is assigned to each of the following markers: hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile INR, elderly and concomitant use of drugs/alcohol. Stroke Prevention in Atrial Fibrillation: Latest Clinical Trials and Guidelines. Luciana Armaganijan et al. Pharmaceuticals 2012, 5, 384 -397

Patient characteristics • A reduced dose of apixaban 2. 5 mg twice a day or placebo was administered (19 pts<65 y, 22 pts 65 -74 y, 790 pts≧ 75 y(13. 9% ≧ 75 y)). • Most of these patients were ≧ 80 y (n=766, 31% of ≧ 80 y). • In patients receiving warfarin, the median TTR (time within therapeutic range for warfarin)was lower in the younger compared with the older (64. 8% for <65 y, 67. 2% for ≧ 75, p<0. 0001). • The numerical difference was small (<3%).

Patient characteristics • Excluding patients who died, more elderly patients discontinued study drug before the end of the study (1067 of 5290 (20%) for <65 y, 1483 of 6792 (21. 8%) for 65 -74 y, 1496 of 5361 (27. 9%) for ≧ 75 y, p<0. 0001)

Outcomes according to age Stroke/systemic embolism ISTH major bleeding All-cause mortality Intracranial bleeding

Efficacy and safety of apixaban vs. warfarin according age

Efficacy and safety of apixaban vs. warfarin according age
 NNT (CI) RRI 16% (-23 to 72) Not significant RRR 28%")
RRI/RRR (95% CI) NNT (CI) RRI 16% (-23 to 72) Not significant RRR 28% (4 to 46) 114 (69 to 797) RRR 29% (5 to 47) 91 (56 to 530) RRI 6. 8% (-16 to 34) Not significant RRR 22% (6 to 35) 69 (44 to 274) RRR 8. 5% (-7 to 22) Not significant RRR 22% (-11 to 45%) Not significant RRR 29% (11 to 43) 75 (49 to 196) RRR 35% (20 to 47) 36 (27 to 62) Very low in both groups

Patients ≧ 80 y • The results were consistent also in patients ≧ 80 y (n=2436). - Stroke or systemic embolism (1. 9%/y with WF vs 1. 53%/y with apixaban, HR 0. 81, 95 % CI 0. 51 -1. 29 ) - Major bleeding (5. 41%/y with WF vs 3. 55%/y with apixaban, HR 0. 66, 95 % CI 0. 48 -0. 90 ) - Intracranial hemorrahe (1. 32%/y with WF vs 0. 47%/y with apixaban, HR 0. 36, 95 % CI 0. 17 -0. 77 )

Patients ≧ 80 y • After testing for an interaction between categorical age and treatment, similar results were found w/o any significant interactions, except for an interaction of borderline significance on net clinical benefit (p=0. 042)

Treatment effect in subgroup of patients ≧ 75 years of age

Treatment effect in subgroup of patients ≧ 75 years of age No significant interactions were found among treatment and dose, neither when studying patients ≧age 75, nor when studying the full cohort of subjects who received the reduced dose of apixaban.

Clinical Appraisal Using EBM method

Are the result valid? • Randomized, double-blind • Patients: 18, 201 patients • Setting: 1034 centers in 39 countries • The rates of stroke, all-cause mortality, and major bleeding were higher in the older age groups (p<0. 001 for all).

What are the results? • In this study, apixaban was shown to be superior to warfarin with respect to stroke prevention, bleeding complications, and mortality, with consistency across all age groups. • The superiority of apixaban vs. warfarin was shown to be consistent even in patient ≧ 80 y. • Taken together with the lack of need for coagulation monitoring and the few drug interactions, apixaban appears to be an attractive alternative for the elderly patients with atrial fibrillation.

Discussion • Bleeding risk increased with age for both rivaroxaban and warfarin in ROCKET-AF, but risks were similar for each treatment across age strata • In RF-LY, patients ≧ 75 y have similar rates of extracranial bleeding with dabigatran, 100 mg BID and a trend toward higher risk for major bleeding with dabigatran 150 mg BID, compared with warfarin. Intracranial bleeding was reduced with both doses of dabigatran in all age groups.

Limitations • Subgroup analysis, although pre-specified, of a trial that comprised all age groups. • The relatively low number of very old people (2436 patients ≧ 80 y) • Selection bias towards more healthy patients being included in the study, especially among the elderly. → 49% of patients ≧ 75 y had CHADS 2 score ≧ 3, mortality/y was 5. 7%, showing a high risk group of patients.

Will the result help me in caring for my patient? • Can the results be applied to my patient care? → Yes • Were all clinically important outcomes considered? → Yes • Are the likely treatment benefits worth potential harms and costs? → Yes

Conclusion • In patients with atrial fibrillation, apixaban reduced stroke or systemic embolism, all-cause mortality, and major bleeding compared with warfarin, regardless of patient age. • In light of these data, apixaban was demonstrated to be very attractive for stroke prevention in atrial fibrillation across the spectrum of age, and particularly for the elderly.

Questions?
- Slides: 44