Educational Workshops 2013 Bone and Joint Infections Survival

Educational Workshops 2013 Bone and Joint Infections Survival of the fittest Julie Samuel Consultant Microbiologist Newcastle upon Tyne Hospitals NHS Foundation Trust

• 54 yr old Asian male diagnosed with Aplastic anaemia in June 2010. • His chemotherapy regime included ATG, ciclosporin , steroids and CAMPATH. He was also on regular blood and platelet transfusions. – CAMPATH- humanised monoclonal antibody against CD 52 leading to profound T and B lymphocyte depletion. – ATG (anti thymocyte globulin) - antibodies against CD 3, CD 8 and CD 4. Mainly indicated in T cell mediated rejection. • Having made no response to ATG he had prolonged admission in July the same year with neutropenic sepsis. • Treated empirically with various abx including ciprofloxacin, piperacillin/tazobactam , meropenem and daptomycin. – (standard neutropenic regime includes Taz + gent +/- dapto/teic) • No empirical antifungals given • Few days into admission: acute left knee swelling, Pain , difficulty weight bearing

Any other relevant questions associated with the knee? • • History of inflammatory arthritis Native or prosthetic joint Trauma Any past history of steroid injections into the joint in the community?

Differential diagnoses • Haematoma secondary to thrombocytopenia • Septic arthritis - native/prosthetic • Inflammatory arthritis - osteoarthritis or rheumatoid arthritis • Crystal arthropathy • Patient had past history of osteoarthritis but no history of prosthetic joints or steroid injections

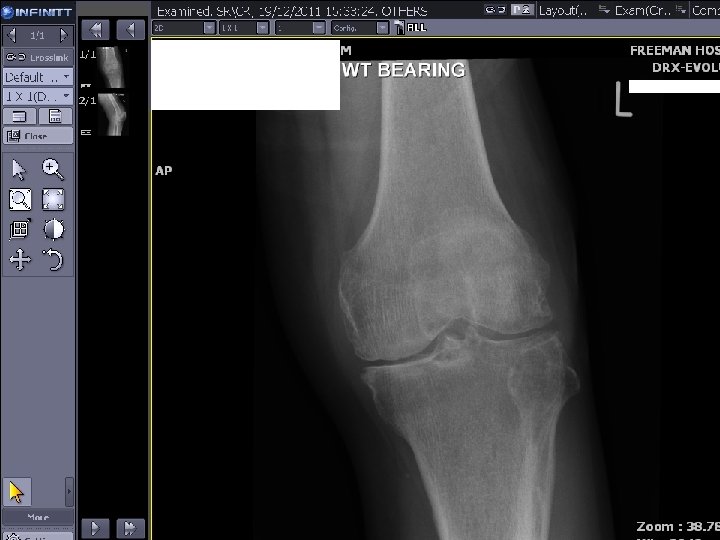
Investigations Full blood count Blood culture hickman line and peripheral – no growth hickman line tip- Coagulase Negative Staphylococci Orthopaedic referral Plain Xray Ultrasonography MRI Aspirate


14/07/10 suprapatellar knee effusion. Moderate medial compartment and patellofemoral OA with joint space loss, osteophyte formation and loose bodies noted in the knee joint.

USG- bony cortical erosion degenerative change joint space reduction left suprapatellar bursa, bakers cyst with intracystic haemorrhage • Diagnostic synovial fluid aspirate - negative for crystals • Gram stain- moderate polymorphs , budding yeast cells with hyphae • Culture

C tropicalis isolated

Candida isolated
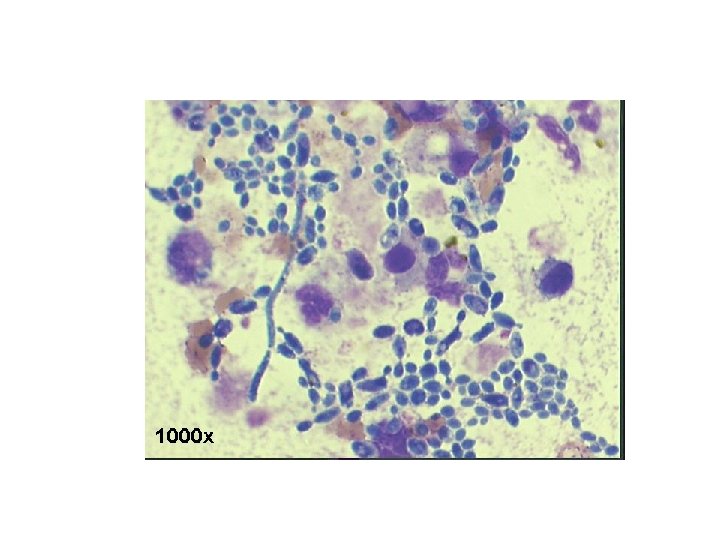

• Candida tropicalis was isolated using Sabouraud dextrose agar and chromogenic media. • Identification was confirmed using morphological characteristics and AUXACOLOR. • MICs were performed using RPMI agar and sensititre plates.

Colonies on Sabourand dextrose or yeast potato dextrose agar - cream-colored , off white to grey, dull, smooth, soft and creamy or wrinkled or rough

Diagnosis True hyphae and pseudohyphae, blastospores in clusters at intervals along the hyphae. Single internodal blastospores sometimes found

Candida tropicalis • 4% of yeasts obtained from seawater, sea sediments, mud flats, marine fish intestine, mangrove plants and marine algae, as well as shrimp, indicating its wide distribution in tropical and subtropical marine environments • Commonly in ITU and neutropenics (30%) • Isolates are generally susceptible to all commonly used antifungal agents, but a trailing endpoint and emergence of azole resistance is problematic. Rare instances of echinocandin and amphotericin B resistance have been described.

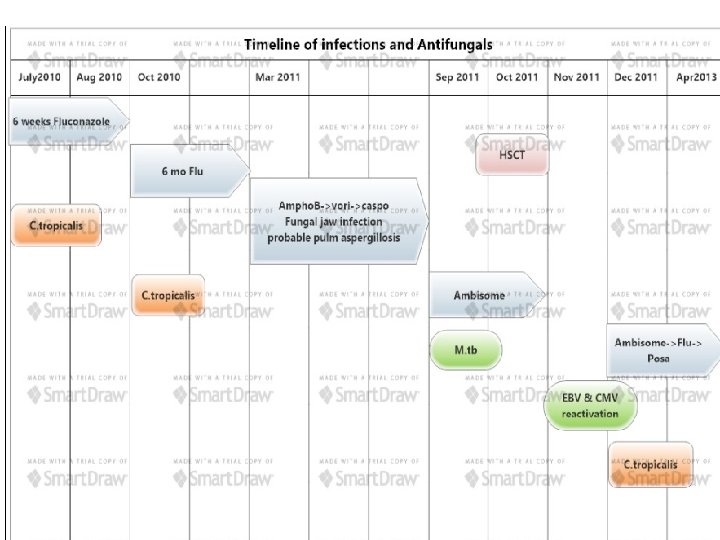
• Orthopaedic referral- they did not consider washing out the joint due to thrombocytopenia. • Discharged on 6 wks fluconazole (2 wks IV followed by oral) 3 months later: similar complaints

What further investigations and would you manage it differently? • Diagnostic aspirate - C tropicalis from enrichment only. • A higher dose of fluconazole (200 followed by 400 bd) for a longer duration (6 months) • The knee was not washed out due to concerns with low platelets. • Xray planned 2 months post treatment • MRI


3 months post fluconazole 1/12/10 Osteoarthritis in all three compartments. There is a joint effusion. Although this could be due to infection, the appearance is non specific and there is no evidence of erosion or other features of infection 2

MRI • 4 months post treatment confirmed the OA degenerative medial meniscus intact cruciate and collaterals parrot beak vertical tear at the midbody of lateral meniscus

• On multiple antifungals for other indications after completion of fluconazole. • Initially treated with ambisome for presumed fungal jaw infection, • Followed by voriconazole and caspofungin for probable pulmonary aspergillosis based on HRCT. • He was always on some antifungals which may have suppressed the fungal arthritis and kept the knee quiescent. • Sep 2011 - He was consented for sibling ALLO transplant pulmonary tuberculosis (M tb complex) diagnosed on CT and culture and he was commenced on standard anti tuberculosis treatment. At this point he was switched to ambisome and meropenem. • • Two weeks after commencing ATT he was transplanted ( chemotherapy included , fludarbine, cyclophosphamide and CAMPATH) This decision to transplant him was based on the rapid progression of his disease.
 Pulmonary Tb Meropenem + ambisome +")
Sep 2011 (14 months post 1 st admission) Pulmonary Tb Meropenem + ambisome + ATT for treatment of neutropenic sepsis and Tb. Ambisome was restarted as part of neutropenic sepsis protocol and with previous h/o pulmonary aspergillosis.

• 2 weeks post ATT- conditioning chemotherapy followed by stem cell transplant in Oct 2011 • Successful engraftment within 21 days

Other concurrent problems CMV and EBV reactivation treated with valganciclovir and rituximab Lamivudine to prevent Hep B reactivation Enterococcus faecium line infection Stenotrophomonas in BAL

28 days post transplant- Ambisome changed to prophylactic dose and stopped after 1 week 1 month off antifungals - another flare up

19/12/11 Joint space narrowing of medial and lateral compartments of knee and patellofemoral joint with large osteophytes in keeping with moderately severe osteoarthritis. An effusion is present. History of septic arthritis noted. No lytic bone lesion present.

• • Knee washed out Aspirate – C. tropicalis Similar MIC values as previous isolates Low dose ambisome changed to fluconazole then switched to posaconazole • ATT stopped after 6 months due to concerns with drug interactions and toxicity. • Echo- no e/o endocarditis • No e/o disseminated candidal infection.
: 0. 5 Itraconazole")
Antifungal MIC July 2010 Oct 2010 Dec 2011 Fluconazole MIC (mg/L): 0. 5 Itraconazole MIC (mg/L): 0. 125 Amphotericin MIC (mg/L): 0. 25 Flucytosine MIC (mg/L): <0. 03 Voriconazole MIC (mg/L): 0. 032 Caspofungin MIC (mg/L): 0. 032 Posaconazole MIC (mg/L): 0. 12 Fluconazole MIC (mg/L): 1. 0 Itraconazole MIC (mg/L): 0. 25 Amphotericin MIC (mg/L): 0. 25 Flucytosine MIC (mg/L): <0. 03 Voriconazole MIC (mg/L): 0. 032 Caspofungin MIC (mg/L): 0. 064 Posaconazole MIC (mg/L): 0. 125 Fluconazole MIC (mg/L): 0. 5 Itraconazole MIC (mg/L): 0. 064 Amphotericin MIC (mg/L): 0. 25 Flucytosine MIC (mg/L): <0. 03 Voriconazole MIC (mg/L): 0. 016 Caspofungin MIC (mg/L): 0. 064 Posaconazole MIC (mg/L): 0. 064

May 2012 • Severe knee pain • MRI - Prominent medial compartment osteoarthritis and effusion
 • Awaiting orthopaedic plan.")
April 2013 • Still on posaconazole (nearly 14 months) • Awaiting orthopaedic plan.

Summary Severely immunosuppressed host Source of candida could probably be attributed to the Hickman line! Persistent joint infection with Candida tropicalis despite antifungal treatment. Conservative management with antifungals Suboptimal surgical management due to severe comorbidities

Key management issues Duration and type of antifungals? Monotherapy or combination treatment? Significant drug interactions- ATT, ciclosporin Risks v/s benefits of early washout Definitive orthopaedic plan?

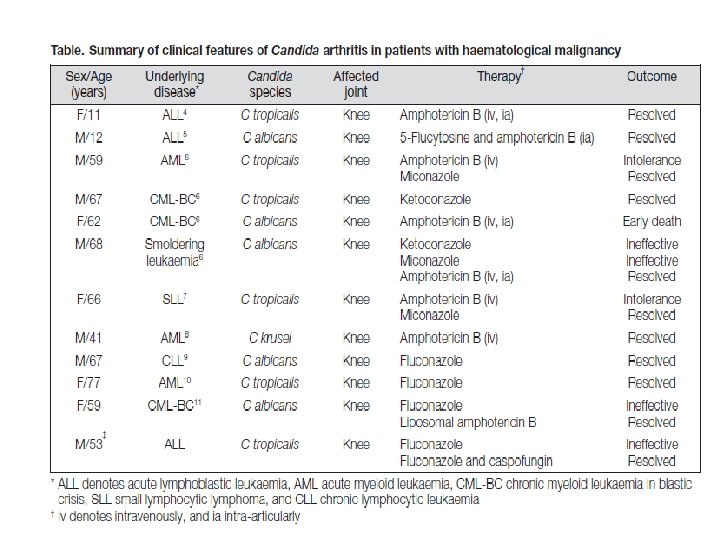
Candida arthritis • Septic arthritis due to Candida species: – hematogenous dissemination – direct inoculation due to trauma, surgery, or intra-articular injections. For hematogenous-related candidal arthritis, C. albicans is responsible for about 70% of cases, while the most frequent non-albicans species are C. tropicalis, C. parapsilosis, and C. krusei. For candidal arthritis related to direct inoculation, the species described, in order of approximate frequency, include C. albicans, C. parapsilosis, C. tropicalis, C. glabrata, and C. zeylanoides. C. parapsilosis is especially linked to arthritis in the setting of a prosthetic joint.

Candida Arthritis Candidal arthritis typically presents with: pain or tenderness of the involved joint. In infants these symptoms are suggested by abnormal positioning of the affected limb. Fever is often absent, and the ability to observe joint warmth or swelling depends on the joint: more superficial joints (e. g. , ankle or knee) will be warm and swollen. Candidal arthritis usually affects large joints, most often the knee. Hip, ankle and shoulder are the next most commonly affected. Arthritis may be the first clinical manifestation of neonatal candidiasis. While presentation may be delayed for some days or weeks following the episode of candidemia in adults, candidal arthritis in the neonate usually presents simultaneously with the acute phase of the disease. Candida joint infection in infants usually presents with concomitant metaphyseal osteomyelitis.

Synovial fluid levels • IV Amphoterecin B - 20 -100% of serum • Fluconazole – 90 -100% of serum

IDSA guidelines 2009 Recommendations • For osteomyelitis, the Expert Panel recommends fluconazole at a dosage of 400 mg (6 mg/kg) daily for 6 -12 months or LFAm. B at a dosage of 3 -5 mg/kg daily for at least 2 weeks, followed by fluconazole at a dosage of 400 mg daily for 6 -12 months (B-III). Alternatives include an echinocandin or Am. B-d at a dosage of 0. 5 -1 mg/kg daily for at least 2 weeks, followed by fluconazole at a dosage of 400 mg daily for 6 -12 months (B-III). Surgical debridement in selected cases is advised (B-III). • For septic arthritis, the Expert Panel recommends treatment for at least 6 weeks with fluconazole at a dosage of 400 mg (6 mg/kg) daily or LFAm. B at a dosage of 3 -5 mg/kg daily for at least 2 weeks, followed by fluconazole at a dosage of 400 mg daily (B-III). Alternatives include an echinocandin or Am. B-d at a dosage of 0. 5 -1 mg/kg daily for at least 2 weeks, followed by fluconazole at a dosage of 400 mg daily for the remainder of therapy (B-III). Surgical debridement is indicated in all cases (A-III). • For infection involving a prosthetic device, device removal is recommended for most cases (A-III). Therapy for at least 6 weeks with the above dosages of fluconazole, LFAm. B, an echinocandin, or Am. B-d is recommended (B-III). If the device cannot be removed, chronic suppression with fluconazole is recommended (B-III).
- Slides: 39