ECTOPIC PREGNANCY Rukset Attar MD Ph D Obstetrics

ECTOPIC PREGNANCY Rukset Attar, MD, Ph. D Obstetrics and Gynecology Department

n n n is a complication of pregnancy in which the pregnancy implants outside the uterine cavity 1. 4 -2 % With rare exceptions, ectopic pregnancies are not viable. About 1% of pregnancies are in an ectopic location with implantation not occurring inside of the womb, and of these 98% occur in the Fallopian tubes The classic symptoms of ectopic pregnancy include: n abdominal pain, n the absence of menstrual periods (amenorrhea), n vaginal bleeding.

n The pain is caused by n n n prostaglandins released at the implantation site, and free blood in the peritoneal cavity, which is a local irritant. If left untreated, about half of ectopic pregnancies will resolve without treatment

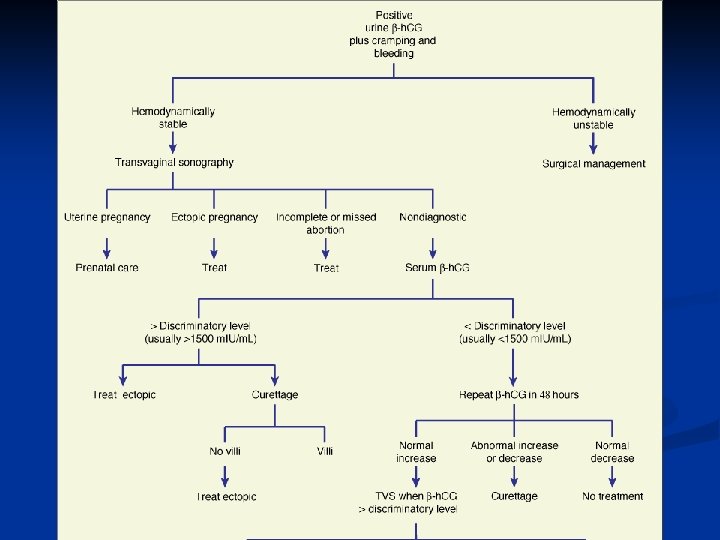
n An intrauterine sac should be visible by transvaginal ultrasound when the β-h. CG is approximately 1000 m. IU/m. L, and by transabdominal ultrasound approximately 1 week later, when the β-h. CG is 1800– 3600 m. IU/m. L.

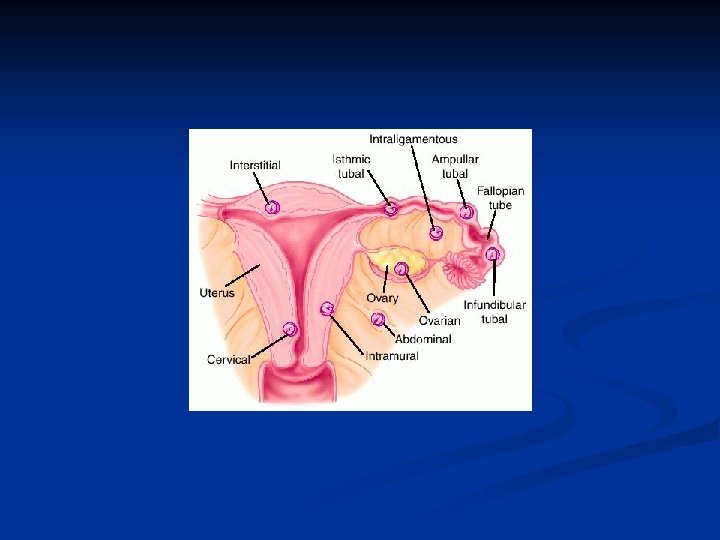
Classification n Tubal pregnancy n Pregnancies can grow in the fimbrial end (5% of all ectopics), n the ampullary section (80%), n the isthmus (12%), n and the cornual and interstitial part of the tube (2%). Isthmic pregnancies rupture earliest, at 6 to 8 weeks’- due to the small diameter of this portion of the tube. Ampullary pregnancies rupture later, generally at 8– 12 weeks. Interstitial pregnancies are the last to rupture, usually at 12– 16 weeks, as the myometrium allows more room to grow than the tubal wall n n

n Nontubal ectopic pregnancy n Two percent of ectopic pregnancies occur in the ovary, cervix, or are intraabdominal n Heterotopic pregnancy n The survival rate of the uterine fetus of an ectopic pregnancy is around 70%

n Persistent ectopic pregnancy n refers to the continuation of trophoplastic growth after a surgical intervention to remove an ectopic pregnancy. n After a conservative procedure such as a salpingotomy some trophoblastic tissue perhaps deeply embedded may escape removal and continues to growth, generating a new rise in h. CG levels.

n n n The most effective way to identify persistent ectopic pregnancies is to monitor serum b-h. CG levels during the postoperative period. Recommendations have varied from every 3 days to 2 weeks Women in whom the serum b-h. CG concentration falls less than 50% are more than 3 times as likely to have a persistent ectopic pregnancy serum b-h. CG on postoperative day 1 and every 3– 7 days thereafter, depending on the rate of decline, until levels are undetectable. For those who exhibit evidence of persistent ectopic pregnancy (rising or slowly falling postoperative b-h. CG concentrations), the single-dose methotrexate treatment regimen (50 mg/m 2 i. m. ) is highly effective.

Causes n n one third to one half of ectopic pregnancies, no risk factors can be identified. Risk factors include: n pelvic inflammatory disease, n infertility, n use of an intrauterine device (IUD), n those who have been exposed to DES, n tubal surgery, n smoking, n previous ectopic pregnancy, and n tubal ligation

Symptoms n Early signs include: n Pain n Vaginal bleeding

Diagnosis n n n n An ectopic pregnancy should be considered in any woman with abdominal pain or vaginal bleeding who has a positive pregnancy test ultrasound β-h. CG Serum progesteron levels laparoscopy or laparotomy Culdocentesis Cullen's sign

Treatment n n n Expectant management Medical n methotrexate Surgical n laparoscopy or laparotomy n salpingostomy n salpingectomy

n Expectant management n Tubal ectopic pregnancies only Decreasing serial -h. CG levels Diameter of the ectopic mass not >3. 5 cm No evidence of intra-abdominal bleeding or rupture by transvaginal sonography n n n

Medical treatment n h. CG < 5, 000 n No cardiac activity n Mass < 4 cm n

n n n Absolute Requirements Hemodynamic stability No evidence of acute intra-abdominal bleeding Reliable commitment to comply with required follow-up care No contraindications to methotrexate treatment

n n n n n Contraindications to Methotrexate Treatment Breastfeeding Immunodeficiency states Hematologic abnormalities (severe anemia, leukopenia, thrombocytopenia) Known sensitivity to methotrexate Active pulmonary disease Active peptic ulcer disease Alcoholism Clinically important hepatic or renal dysfunction
 Serum concentration less than")
n n n Preferred Characteristics Absent or mild symptoms (pain) Serum concentration less than 5, 000 IU/L Absent embryonic heart activity Ectopic mass measuring less than 4 cm in diameter
 Serum creatinine")
n n n Pre-treatment evaluation: Complete blood count Blood type and Rh(D) Serum creatinine Liver function tests Transvaginal ultrasonography

n patients should be advised to n n discontinue any folic acid supplements they may be taking to avoid n n n sun exposure (to decrease risk of methotrexate dermatitis), use of non-steroidal antiinfl ammatory drugs (interaction with methotrexate may cause bone mar-row suppression or gastrointestinal toxicity), and intercourse or strenuous physical activity (to decrease the risk of tubal rupture).

n “single-dose” treatment regimen n methotrexate is administered in a single dose (50 mg/m 2, day 1) n if the serum b-h. CG declines 15% or more between days 4 and 7, treatment is deemed successful and b-h. CG concentrations are monitored weekly thereafter until undetectable. n In the majority of women (85%), serum b-h. CG concentrations rise somewhat between days 1 and 4 - normal

n n n Any subsequent further increase in b-h. CG levels, or a decrease of less than 15% between days 4 and 7, is indication for a second dose (on day 7), using the same criteria for judging response (on day 11). If required, a third dose can be administered on day 11 and the response evaluated by measuring b-h. CG again on day 14. Although a fourth dose can be administered (on day 14), surgical treatment generally is recommended after 2 weeks of failed medical treatment.

n 2 -dose treatment regimen n Methotrexate is administered on days 1 and 4 (50 mg/m 2) If the serum b-h. CG declines 15% or more between days 4 and 7, levels are monitored weekly until levels become undetectable If b-h. CG concentrations decreases by less than 15% between days 4 and 7, a third dose of methotrexate is administered (on day 7) and the same criterion is applied in judging the response to treatment on day 11. If necessary, a fourth dose is administered (on day 11) and the serum b-h. CG concentration is assessed again on day 14. n n n
 and leukovorin")
n n n Multi-dose treatment regimen Methotrexate (1 mg/kg i. m. ) and leukovorin (0. 1 mg/kg i. m. ) are administered on alternate days, up to a maximum of four doses, until the serum b -h. CG level declines by 15% from the previous value. Thereafter, b-h. CG concentrations are monitored on a weekly basis until levels become undetectable.

Indications for surgical treatment n n n n Hemodynamic instability Rupture of an ectopic mass Coexisting viable intrauterine pregnancy Unwillingness or inability to comply with required followup after medical treatment Lack of ready access to a hospital for management of tubal rupture Desire for permanent sterilization Contraindications to medical treatment Failed medical treatment
- Slides: 26