ECTOPIC PREGNANCY By M KamphindaBanda University of Malawi

ECTOPIC PREGNANCY By M. Kamphinda-Banda University of Malawi Kamuzu College of Nursing Medical Surgical Nursing 12 TH MAY 2011

Define Ectopic pregnancy Explain the aetiology of ectopic pregnancy Explain the risk factors

Explain the pathophysiology of ectopic pregnancy Explain the clinical manifestations of Ectopic pregnancy Describe the management of ectopic pregnancy

DEFINITION It is a condition where by a fertilised ovum is implanted on any tissue other than lining of the uterine cavity e. g. fallopian tube Also known as extra uterine pregnancy

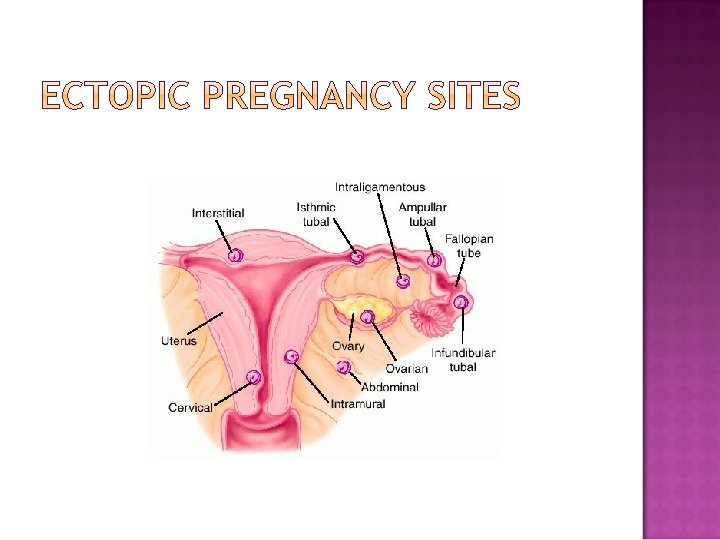
Abdominal cavity Cervix The ovary Ampullar Isthmus Infundibular

The cause is unknown.

More common in low social economic status women & the incidence has increased because of PID, the increase use of intra uterine devices, progesterone only oral contraceptive It is also common in older women (35 -44 yrs) who have had previous pregnancies than in teenagers due to degeneration of the lumen of the fallopian tubes.

Multiple factors contribute to the relative risk of ectopic pregnancy. In theory, anything that hampers the migration of the embryo to the endometrial cavity could predispose women to ectopic gestation.

The most logical explanation for the increasing frequency of ectopic pregnancy is previous pelvic infection; however, most pts presenting with an ectopic pregnancy have no identifiable risk factor.

Pelvic inflammatory diseases due to ascending infection e. g. cervicitis, salpingitis wc can be caused by Chlamydia, Neisseria gonorrhoea. Congenital abnormalities of the tubes.

Previous history of Ectopic pregnancy Use of IUCD causes tubal damage due to salpingitis. IUCD can be the source of infection.

History of prior ectopic pregnancy After one E/P, a pt incurs a 7 - to 13 -fold increase in the likelihood of another E/P Overall, a pt with prior E/P has a 50 -80% chance of having a subsequent intrauterine gestation, & a 1025% chance of a future tubal pregnancy.

History of tubal surgery & conception after tubal ligation Prior tubal surgery increases the risk of developing ectopic pregnancy. The increase depends on the degree of damage & the extent of anatomic alteration. E. g. salpingostomy, , fimbrioplasty, tubal reanastomosis.

Use of progestin- only contraceptive they interfere with tubal peristalsis. Previous pelvic or abdominal surgery. Multiple previous induced abortions.

Mechanical or functional factors prevent or interfere with the passage of the fertilized egg to the uterine cavity. e. g. pelvic infection The fertilized egg then implants itself inside the tube.

If implantation occurs into a site of the tube that offers a sufficient area for placentation, the process is very similar to that of an intrauterine pregnancy, because the conceptus penetrates the tubal mucosa & becomes embedded in the tissues of the tubal wall.

The trophoblast penetrates the full thickness of the muscular layer of the tube to reach the subserosa & the tubal ovarian circulation

As the fertilised ovum increases in size the tube becomes more & more distended, until finally 4 to 6 weeks after conception, rupture takes place & the ovum is discharged into the abdominal cavity.

This event is usually accompanied by fetal death Occasionally, following the rupture the fetus retains sufficient attachment to its bld supply to maintain viability & secondary abdominal preg can proceed to term

If the ectopic pregnancy miscarries, the uterine decidua may slough off as a cast, or more commonly as fragments mixed with small blood clots.

Subjective data History is very important History of amenorrhoea of about 6 -8 wks but may be longer if implantation occurs in the interstitial portion of the tube, or in abdominal pregnancy History of persistent mild lower abdominal pains

Subjective data History of vague localised pain on the affected side due to tubal distension History of sharp colicky pain & a sudden excruciating pain when tube has ruptured History of backache History of dizziness, nausea &vomiting

Objective Data Physical examination On palpation: -There is a unilateral lower quadrant tenderness Generalised abdominal pain when rupture has occurred. This is due to spilling of blood into the peritoneum Tender boggy mass in cul-de-sac may indicate pelvic haematocele.

Objective Data Vaginal bleeding, slight, dark brown Intermittent / continuous, due to falling hormones due to fetal death Adnexal tenderness Abdominal tenderness Adnexal mass

Patient rapidly goes into shock with decreased BP, rapid weak pulse rate, pallor, sweating, low body temperature and cold extremities If there’s hemoperitonitis, temperature will be high 38°C or more

Utrasonography: - May show extra uterine gestational sac Laparoscopy: - Confirms tubal pregnancy through visualisation of distended tube or site of implantation Dilatation and curettage: - May confirm ectopic pregnancy through pelvic examination under anaesthesia or rule out if placental tissue is obtained from endometrium

Culdoscentesis – the passing of a wide bore needle through the posterior fornix. Old blood is very suggestive, but the absence of blood does not exclude an ectopic pregnancy.

Human chorionic gonadotrophin & transvaginal ultrasound The Hcg & USS findings must be interpreted together. One of the most important parameters is the discriminatory Hcg level above which the gestational sac of an intrauterine pregnancy shld be detected by ultra sound (usually 1000 i. /L)

Threatened abortion incomplete abortion Corpus luteum cyst Salpingitis UTI Acute appendicitis

PROGNOSIS Mortality is increased with tubal rupture but patient recovers rapidly when surgery is performed early Recurrence of another E/P is 5 -6 times greater than for a woman who has never had an ectopic pregnancy.

Unruptured tube Lower abdominal pains & tenderness that may be generalised or unilateral Signs of pregnancy like amenorrhoea, nausea, vomiting & breast tenderness Pelvic mass may be palpable.

Ruptured tube Severe abdominal pain that is sudden & stabbing. Dizziness Fainting Referred supraclavicular pain Vaginal bleeding (not always present) Pallor Cervical pain during vaginal examination

Progressive supine hypertension Tachycardia & tachypnea Decreased hematocrit value Shock

EMMERGENCY SURGERY: In cases where the preg is located on cervix, ovary, or in the interstitial or the cornual portion of the tube is often associated with increased risk of hemorrhage, often resulting in hysterectomy or oophorectomy. Salpingectomy or salpingoophorectomy depending on findings

Decreased cardiac output, shock related to haemorrhage evidenced by reduced B/P, etc Goal: To maintain normal cardiac output Actions: Place pt in supine position with the head and chest on the same level while the legs are elevated at a 45 angle.

The position promotes blood supply to vital organs the heart, brain & kidneys thereby minimizing the signs of shock Provide extra linen to the pt prevent hypothermia. BUT avoid providing a heater which will cause sudden dilatation of superficial blood vessels thereby leading to decreased bld supply to the vital organs.

Explain the condition & its management to pt in a simple language & calm manner & allow her to ask questions in order to allay anxiety

Collect blood samples for Hb level, grouping & cross-matching & cross the form in order to be processed urgently. These will assist in knowing how much she needs to be transfused & also to avoid blood reactions during transfusion.

Commence haemacel, a plasma expander 1 litre in 1 hour which will assist in raising the circulatory volume

IF HAEMACEL IS NOT AVAILABLE THEN Commence IV infusion of either R/L or N/ S 1 litre to run in an hour which will maintain the intravascular osmotic pressure thereby correcting the state of shock.

Arrange for 2 pints of blood with the laboratory staff since pt is bleeding internally & may need transfusion Provide extra linen to patient to relieve the problem of hypothermia. BUT avoid providing a heater which will cause sudden dilatation of superficial blood vessels thereby leading to decreased blood supply to the vital organs.

Monitor Temperature, Pulse rate, Respirations, Blood pressure, level of consciousness & the mucous membranes ¼ hourly until patient goes to theatre The monitoring will evaluate effectiveness of the nursing interventions given i. e. reduced restlessness, a rise in Blood pressure & temperature, a drop in pulse rate & respirations indicate that she is recovering from shock.

Monitor level of consciousness & record using glassgow coma scale Monitor intake & output, record on chart Assess vaginal blood loss for colour, odour & consistency

Altered comfort, abdominal pain, related to intrauterine contraction & tubal distension Goal: Pt will verbalise relief from pain Actions: Explain to pt about the findings & plan of care

Put pt on complete bed rest in the comfortable position to lessen pain Do not give analgesics because they mask symptoms

Altered renal perfusion, oliguria related to haemorrhage Goal: To maintain normal tissue perfusion Actions: Catheterize pts urinary bladder with foleys catheter, using aseptic technique, to prevent trauma to the bladder during the operation & infection respectively.

Strictly monitor intake & output ½ hourly in order to assess kidney function & to prevent over or under hydration that may complicate the condition Note amount & colour of urine then record on chart Catheter care to prevent infection

High risk for infection related to pelvic Bleeding Goal: Pt will not develop infection throughout hospitalisation period Action: Maintain sterility in carrying out procedures to prevent infection e. g. catheter care

Provide sterile sanitary pads & monitor vaginal loss Clean the patient of any vomitus whenever necessary
 related to lack of knowledge on the disease process &")
Ineffective coping mechanism (anxiety) related to lack of knowledge on the disease process & the pending surgery. Goal: Pt will demonstrate understanding of her problem

Action: Explain the disease process & its mgt including the impending emergency surgery to the pt in a simple language & calm manner & allow her to ask questions in order to allay anxiety.

Obtain an informed consent after explaining the procedure to the pt as a legal agreement for the operation Inform her that she should neither drink nor eat to avoid aspiration since she is going to theatre.

Remove dentures to prevent choking in theatre Administer prophylactic antibiotic stat i. e. Chloramphenicol gm intravenously or Benzyl penicillin 3 mega units or Ampicillin 500 mg intravenously

Inform theatre team to prepare for the procedure Shave pt if necessary and or according to protocol Stay with pt, reassure, support & encourage the pt

Confirm with the laboratory for availability of blood. Attend to partner if available Take care of pts property & escort patient to theatre

POST OPERATIVE CARE It is the same as in any surgery Specific Position pt in a way that airway is maintained Monitor V/S every 15 minutes for the first two hours, then every ½ hrly, 2 hrly then 4 hrly

POST OPERATIVE CARE The condition of the abdominal dressing should be observed at regular intervals and vulval pads inspected for blood loss. Maintain infusion & monitor intake & output

POST OPERATIVE CARE Transfusion: may have auto transfusion make necessary arrangements and check Hb after 48 hours Give prescribed analgesics, Pethidine 100 mg intramuscularly

POST OPERATIVE CARE Administer antibiotics if signs of infection appear e. g. increased temperature Gentamycin 240 mgs im od x 7/7 Flagyl 500 mgs IV three times a day x 48 hours then orally x 5/7 Chloramphenicol 1 gm intravenously IV every 6 hours x 48 hours then orally for 5 days

POST OPERATIVE CARE Remove catheter after 48 hours or earlier if indicated Give oral fluids when bowel sounds are present, soft diet then regular diet with high vitamins, protein to correct anaemia & facilitate wound healing

POST OPERATIVE CARE Encourage deep breathing exercises to prevent chest complications from arising Leg exercises will improve the circulation & prevent deep vein thrombosis from occurring.

POST OPERATIVE CARE Support couples grief through listening & offering explanations about their conditions Help couple to verbalise their feelings when they find it difficult to do so, you may even consult the clergy.

POST OPERATIVE CARE Early ambulation to prevent DVT & chest complications I. E. C, when crisis is over explain cause of the condition, treatment counsel on F/P Also explain the impact on future pregnancies include partner in the discussion

POST OPERATIVE CARE Pt & partner may not express loss of pregnancy verbally, be available to observe and listen, provide psychological & emotional support, you can consult the clergy Remove alternate sutures on day 7, the rest on day 8 Discharge pt if no problems Follow up visit at Gynaecological Clinic after 2 weeks
- Slides: 66