Echocardiographic Evaluation of LV Diastolic Function Rasoul Azarfarin



 RELAXATION ENERGY DEPENDENT")






")





 http: //www. echobasics. de/diastole-en. html")
 • E/e’ ratio (combo of transmitral flow velocity and annular")

 in Color M-Mod Echo http: //www. echobasics. de/diastole-en. html")
 Wang et al Global Diastolic SR for LV Relaxation Circ.")




- Slides: 31
Echocardiographic Evaluation of LV Diastolic Function Rasoul Azarfarin MD, FACC Professor of Anesthesiology
Case scenario • A 70 yrs old female presenting with severe dyspnea at rest. • History of HTN (BP=180/95 mm. Hg) • Echo: LVEF=50% mod LVH
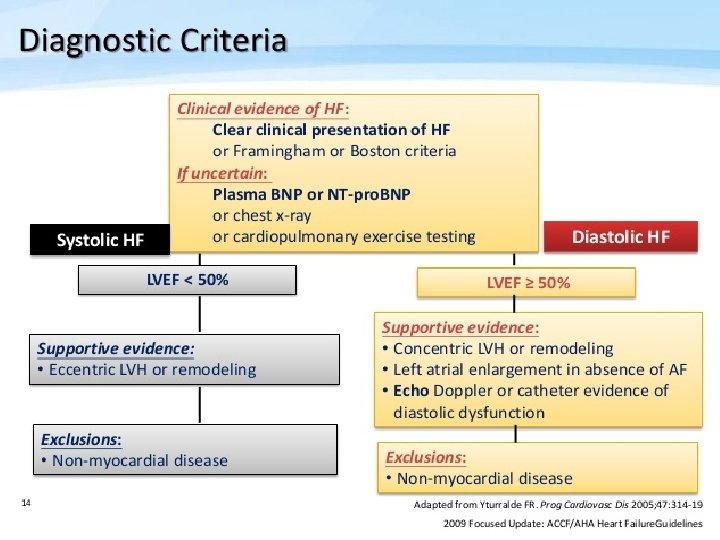
TERMINOLOGY Diastolic dysfunction Alteration in active or passive relaxation of the LV Diastolic heart failure Signs/symptoms of heart failure & normal ventricular function/size and findings of abnormal diastolic function Systolic heart failure Signs/symptoms of heart failure & abnormal ventricular function/size.
ISOVOLUMIC (EARLY) RELAXATION ENERGY DEPENDENT
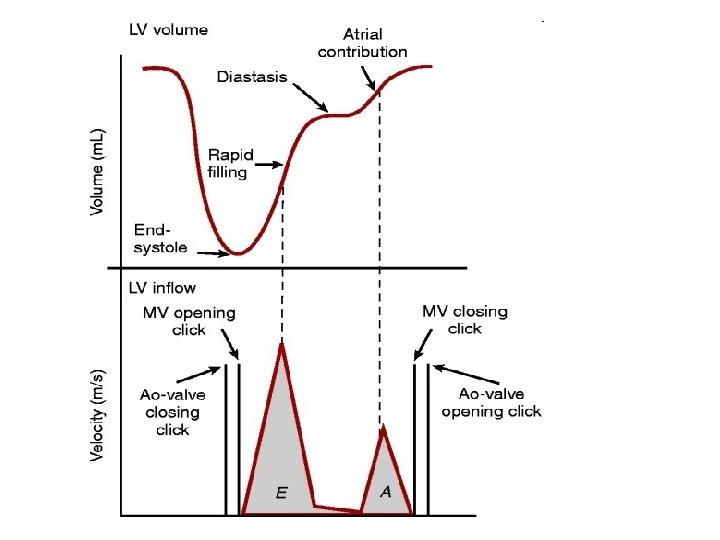
Phases of diastole
Pressure-Volume Loop
Elevated Left Ventricular Diastolic Pressure Causes Pulmonary Congestion
LV anatomic changes alters distensibility in chronic non-ischemic disorders Myocardial cell Hypertrophy occurs and corresponds to wall thickness as per Echocardiogram Active fibrotic process occurs with increase in the amount of collagen and shift to less pliable collagen
LV Diastolic Distensibility Stiffness- Compliance- Distensibility are best quantified by the LV pressure / volume relationship
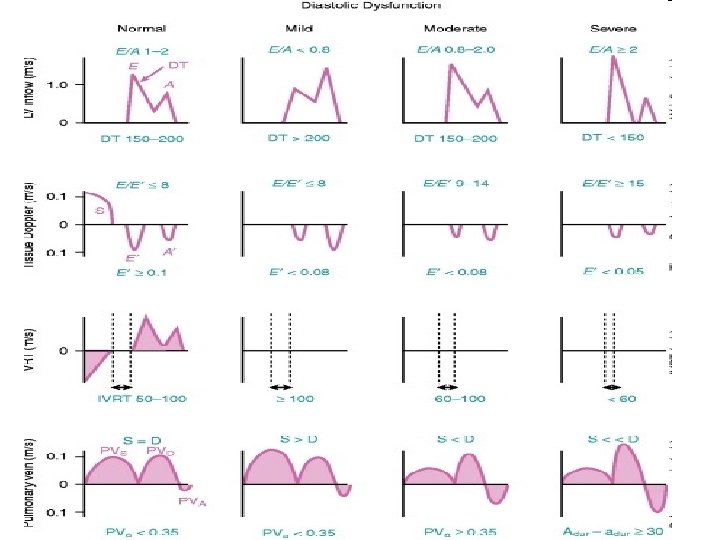
Assessment of Diastolic Function Echocardiogram Normal Heart size and normal contraction pattern E/A flow velocity ratio : in DD E declines and A increases (normal: 1. 2 - 2 & Abnormal <1) ; also Abnormal pulmonary venous flow velocity E A Cardiac Catheterization Normal heart size and contraction pattern LV end diastolic pressure (normal =12 mm. Hg) Greater specificity when 16 mm. Hg used as upper normal.
COMMON CAUSES OF DIASTOLIC DYSFUNCTION Ischemia (potentially reversible delay in or incomplete early relaxation) Acute Hypertension (potentially reversible delay in or incomplete early relaxation) Infarction (increased passive stiffness) Chronic Hypertension with Hypertrophy (increased passive stiffness) Aortic Stenosis & IHSS (increased passive stiffness) Idiopathic Hypertrophic Cardiomyopathy (increased passive stiffness) Diabetes and Obesity (increased passive stiffness)
Triggers To Pulmonary Congestion In Patients With Diastolic Dysfunction Volume overload Increased salt & water intake Chronic renal disease Iatrogenic (procedure or surgery related) Severe chronic anemia Tachycardia Atrial Fibrillation with and without rapid VR Hypertension (>200 mm. Hg) Ischemia
Exercise Response In Diastolic Dysfunction
Acute Treatment Of Diastolic Heart Failure Reduce intravascular volume carefully Morphine, diuretic, NTG Control Systolic BP in obvious hypertensive state Morphine, diuretic, NTG, ACE inhibitors, betablocker Treat any ischemia NTG, anti-thrombotic Rx, if indicated Control ventricular heart rate Beta blocker, Ca++ channel blocker
Transmitral Doppler Inflow http: //www. echobasics. de/diastole-en. html
IVRT
Tissue Doppler Imaging (e’) http: //www. echobasics. de/diastole-en. html
Tissue Doppler Imaging (e’) • E/e’ ratio (combo of transmitral flow velocity and annular velocity) is best parameter for predicting mean LVEDP (<8 nl, >15 abnl); but cannot be used in isolation!
Pulmonary Venous Doppler Flow http: //www. echobasics. de/diastole-en. html
Mitral Inflow Propagation Velocity (Vp) in Color M-Mod Echo http: //www. echobasics. de/diastole-en. html
Global Strain Rate (SRivr) Wang et al Global Diastolic SR for LV Relaxation Circ. 2007; 115: 1376 -1383.
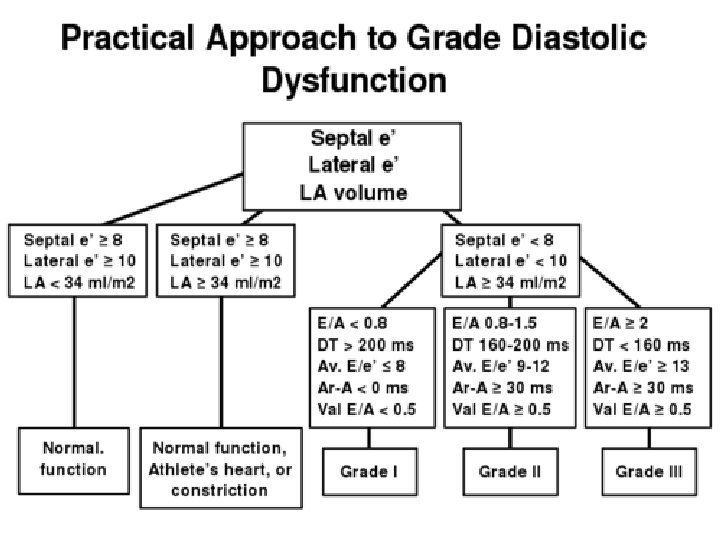
LA Volume • Barometer of the chronicity of diastolic dysfunction. • LA volume correlates with risk of cardiovascular events including MI, CVA, A fib and CHF. • More stable than LV filling pressures. Douglas PS. The left atrium: a biomarker of chronic diastolic dysfunction and cardiovascular disease risk. JACC 2002; 42: 1206 -7.
Approach to the Patient BIDMC Echo Lab Decel Time 140 -250 ms E/e’: <8 normal E/e’>15 (LVEDP>18 mm. Hg)
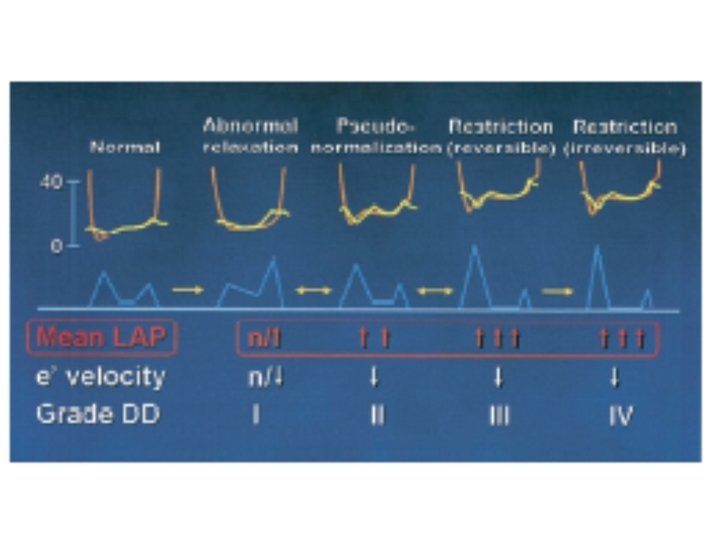
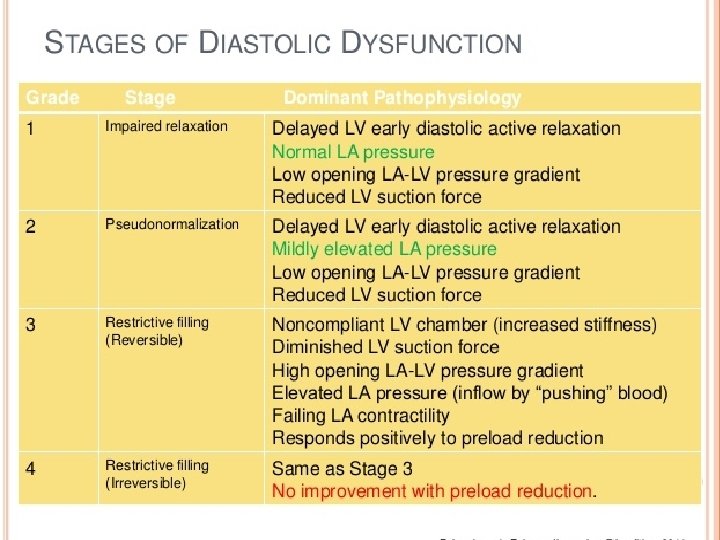
Summary • Diastole is a complex, energy dependent process. • Echo indices of diastolic fn include: – – Transmitral Doppler inflow Tissue Doppler velocities Pulmonary venous Doppler flow Color M-mode propagation velocity • Diastolic dysfunction is a measurable, step-wise progression from normal to irreversible.
References • • Otto CM. Textbook of clinical echocardiography, 4 th Edition. Douglas PS. The left atrium: a biomarker of chronic diastolic dysfunction and relation to cardiovascular risk burden. JACC 2002; 40: 1206 -7. http: //www. echobasics. de/diastole-en. html Lester SJ, Tajik AJ, Nishimura RA, et al. Unlocking the mysteries of diastolic function. JACC 2008; 51: 679 -89. Nagueh SF, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am S Echo 2009; 22: 107 -33 Nishimura RA, Tajik AJ. Evaluation of diastolic filling of left ventricle in health and disease: Doppler echocardiography is the clinician’s Rosetta Stone. JACC 1997; 30: 8 -18. Ommen SR, Nishimura RA, Appleton CP, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: a comparative simultaneous Dopplercatheterization study. Circ. 2000; 102: 1788 -94. Wang J, Khoury DS, Thohan V, Torre-Amione G, Nagueh SF. Global diastolic strain rate for the assessment of left ventricular relaxation and filling pressures. Circ. 2007; 115: 1376 -83.