Echo of Mitral Stenosis Severity and Important Echo







 • Mitral")









")
 showed that MV area could be")








 (grade 1 – 4) • Leaflet thickening •")


 Mitral Balloon Valvotomy and Outcome 100 MV")

 Limitations • Subjective (High interobserver variability) • Inability")
- Slides: 40
Echo of Mitral Stenosis Severity and Important Echo Features Steven A. Goldstein MD FACC Director, Noninvasive Cardiology Medstar Heart Institute Washington Hospital Center Sunday, February 22, 2015
DISCLOSURE I have N O relevant financial relationships
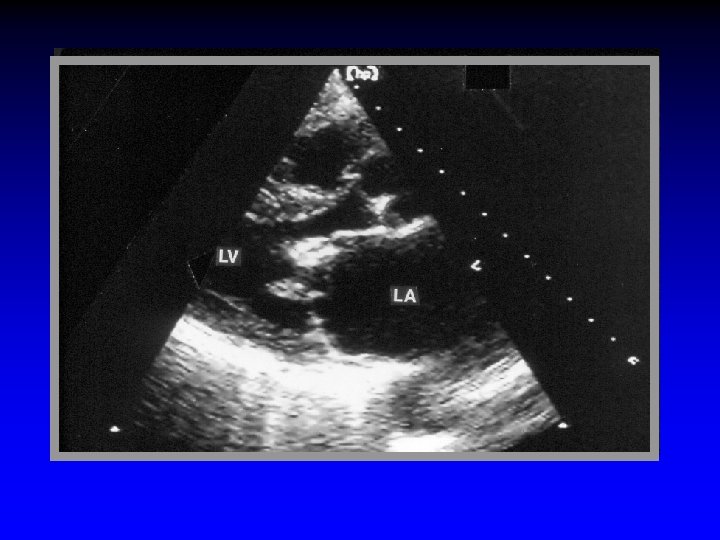
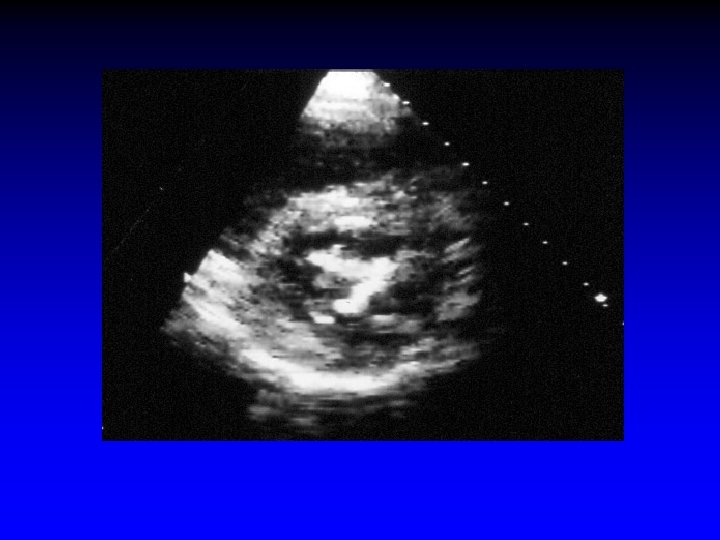
Mitral Stenosis Morphology • Leaflet thickening and calcification • Commissural fusion • Commissural and leaflet calcification • Chordal thickening, shortening & fusion
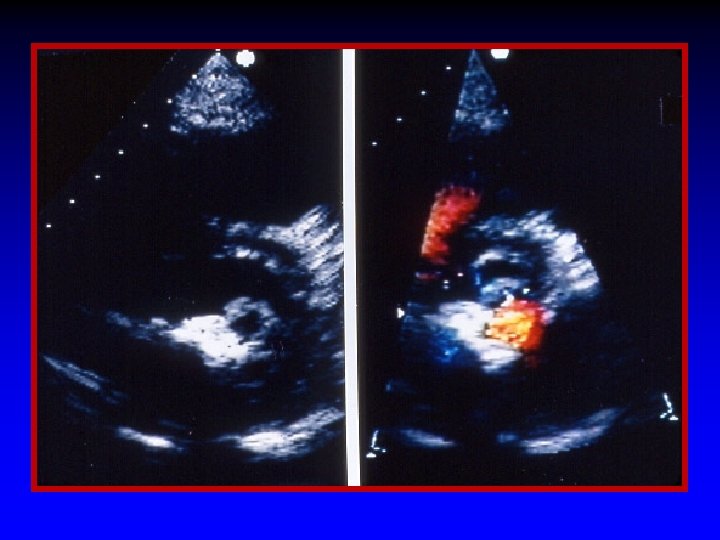
Pre-PTMV Post-PTMV
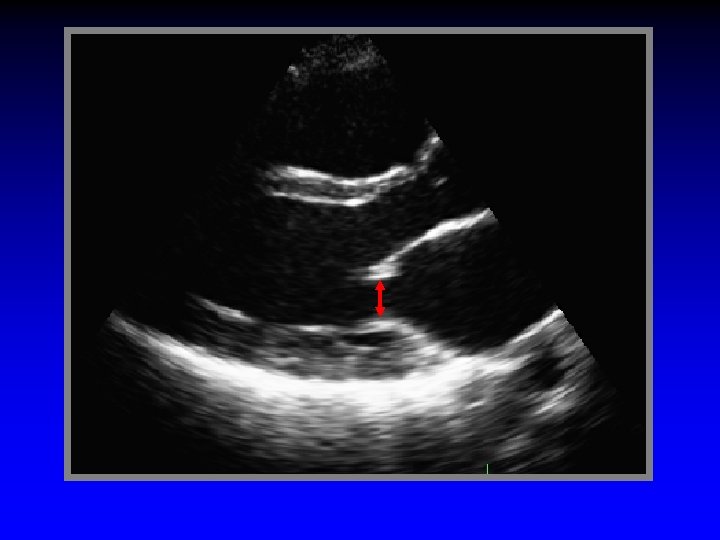
Scan off-axis to evaluate subvalve apparatus
Severity of Mitral Stenosis Echo-Doppler is method of choice
Mitral Stenosis Quantitation by Echo-Doppler • Transvalvular gradients (Peak, mean , end-diastolic) • Mitral valve area § § Planimetry Pressure half-time method Continuity equation PISA method • Pulmonary artery pressure
Gradients
Mitral Stenosis Doppler-Derived Gradients • Unlike AS, technically easy in MS • Reliable gradient almost always obtained with transducer at apex • In rare instance of extremely difficult apical window, TEE can be used
Mean PG 23. 9 mm Hg VTI 94 cm Vmax 320 cm/s Mean gradient = 24 mm Hg
18 mm Hg 13 mm Hg In atrial fib average ≥ 5 consecutive beats
Mitral Stenosis Pitfalls of Doppler Evaluation Pressure Gradient • Intercept angle b/w MS jet and echo-beam • Beat-to-beat variability in atrial fibrillation • Dependence on transvalve flow rate (depends on current HR, CO, MR) Always report HR ! (variable)
MV Area
MV Area by Planimetry Advantages: Ease of use Pathologic correlation Unaffected by MR and AR Limitations: May not image true orifice Gain and angulation Calcification Prior commissurotomy
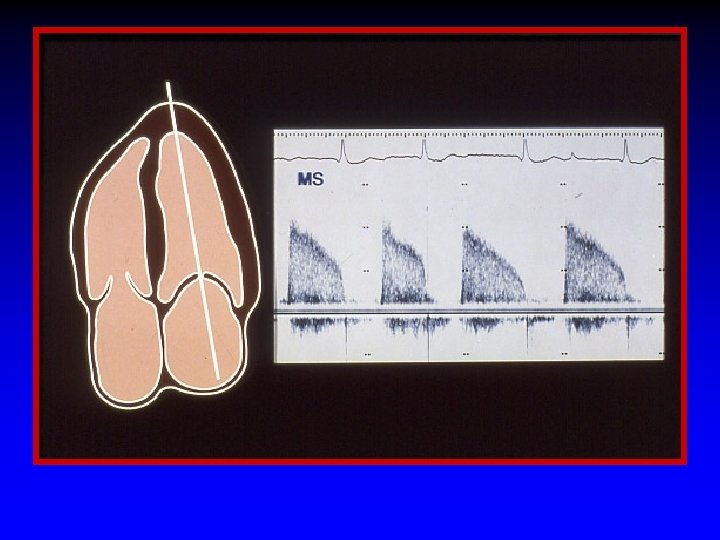
Pressure Halftime
Atrioventricular Pressure Half-Time Measurement of Mitral Orifice Area Libanoff and Rodbard Circ 38: 144(1968)
Mitral Valve Area Doppler Pressure Halftime Hatle (1979) showed that MV area could be estimated as. . 220 Doppler-derived mitral pressure halftime
MV Area Continuity Equation
Mitral Valve Area Continuity Equation MV Area = CSA LVOT x VTILVOT VTI MS JET
MV Area PISA
r = 1. 2 cm Va = 30. 8 cm/s
Mitral Valve Area: PISA Method Standard PISA Equation Assumption Orifice is planar Mitral Stenosis Correction Orifice is NOT planar Orifice is Funnel-shaped PISA Flow Rate Orifice Area (cm 2) = (cm 3/sec) Vmax (cm/sec) x Angle 0/180º Average 0 = 118 ± 15º Circulation 1993; 88: 1157 -65
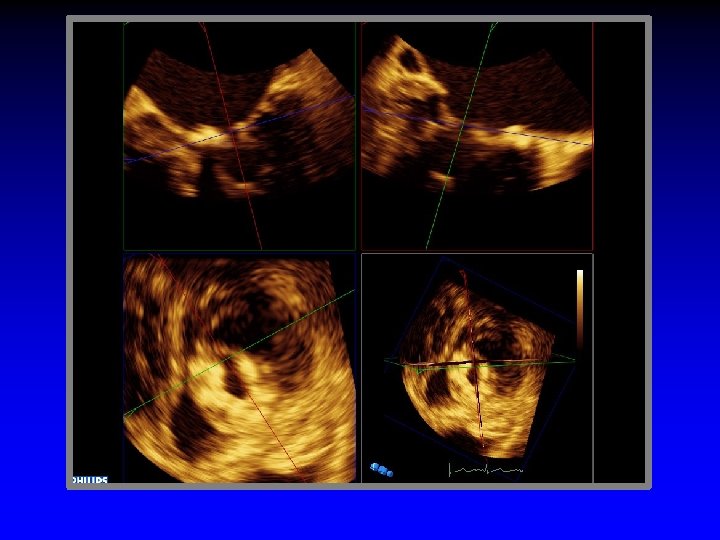
3 D-Echo likely the new “Gold Standard” Post-PTMV Pre-PTMV
A 1 = 0. 80 cm 2 TTE MV area = 0. 80 cm 2
“Splittability” Score
Mitral Stenosis “Splittability” Score (MGH Score) (grade 1 – 4) • Leaflet thickening • Leaflet mobility • Leaflet calcification • Subvalvular fusion Score < 8 = excellent candidate for PBMV
Mitral Stenosis "Splittability Score" I. Leaflet mobility II. Leaflet thickening III. Leaflet calcification IV. Subvalve thickening & fusion • Appearance of commissures
Mitral Valvuloplasty The mechanism of successful PBMV is opening of commissures RV RV
Freedom from Death, MVR, repeat PBMV (%) Mitral Balloon Valvotomy and Outcome 100 MV score 8 80 80 MV score >8 60 60 40 40 20 20 0 Ca++absent 0 0. 5 1 1. 5 2 2. 5 Years from Procedure 3 0 0 Ca++present 0. 5 1 1. 5 2 2. 5 Years from Procedure Cannan, Nishimura, et al JACC 29: 175(1997) 3
Mitral Valvuloplasty Commissural Calcium RV RV
Mitral Stenosis “Splittability” Score (MGH Score) Limitations • Subjective (High interobserver variability) • Inability to describe localized changes • Some pts with score > 10 successful PBMV • Some pts with score < 8 have complications