ECG leffort positifngatif oublier Dr Guy Tremblay CHU

ECG à l’effort. . positif-négatif à oublier Dr Guy Tremblay CHU de Québec – Université Laval

Déclaration d’intérêts potentiels • Conférencier pour EMC: • Centre de Santé Publique 03, FMOQ, FMSQ • Universités Laval, Mc. Gill • Sea Course • Amgen, Sanofi • Consultant médical: La Capitale, L’Union-Vie, SSQ • Cardiologue clinicien : CHU-Québec (HSS ) CIUSSQ ( Jeffery-Hale) Pas de conflit d’intérêt pour cet présentation …

ECG d’effort. . positif / négatif à oublier … Après cette présentation, les participants pourront… § expliquer l’histoire naturelle de MCAS § distinguer sensibilité et spécificité d’un test § reconnaître impact de la prévalence d’une maladie sur VPPositive et VPNégative § utiliser l’épreuve d’effort en sélection pour screening , diagnostic et PRONOSTIC. 3

Théoreme de Bayes La Valeur Prédictive Positive et la Valeur Prédictive Négative d’un test dépend plus de la prévalence de la maladie que de la sensibilité et spécificité du test … Révérend Thomas Bayes, 1702 -1761
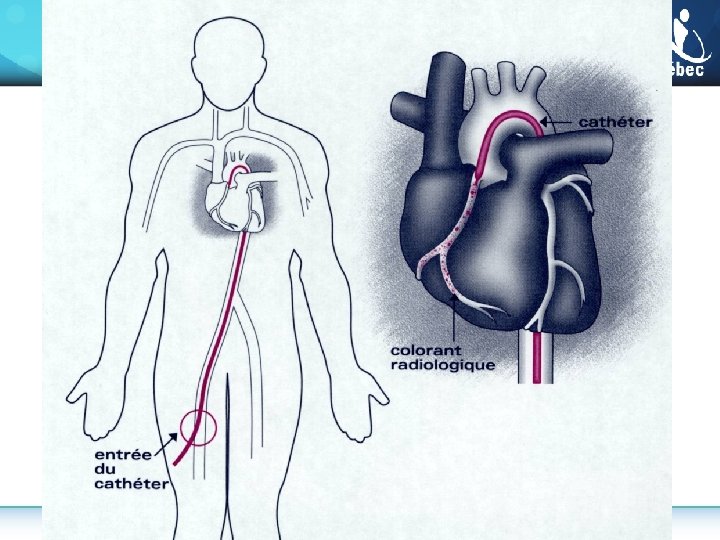

CT Angio

SCA ie infarctus , angine instable, mort subite MCOC ie angine stable, post-infarctus , post angioplastie et post PAC

Classification clinique des douleurs thoraciques Ø Angor typique 1. 2. 3. Douleur/malaise rétro-sternale provoquée par l’exercice ou les émotions soulagée par le repos ou la TNT, en <10 min Ø Angor atypique § rencontre deux des trois caractéristiques Ø Douleur thoracique d’étiologie indéterminée § rencontre ≤ 1 des caractéristiques de l’angine typique

Pretest likelihood of CAD as detected by invasive angiography in symptomatic patients according to age and sex (Combined Diamond Forrester and CASS Data). A low pretest risk of CAD is considered < 10% (green) and a high pretest risk is considered > 90% (red). All others are at intermediate risk (yellow). Chest Pain Criteria: 1. Sub-sternal chest discomfort with characteristic quality and duration 2. Provoked by exertion or emotional stress 3. Relieved promptly by rest or nitroglycerin Non-anginal Chest Pain Atypical Angina Typical Angina 1 of 3 Criteria 2 of 3 Criteria 3 of 3 Criteria Age Male Female 30 – 39 4% 2% 34% 12% 76% 26% 40 - 49 13% 3% 51% 22% 87% 55% 50 - 59 20% 7% 65% 33% 93% 73% 60 – 69 27% 14% 72% 51% 94% 86% Adapted from Diamond et al NEJM 1979; 300: 1350 -58 and Weiner et al NEJM 1979; 301: 230 -5

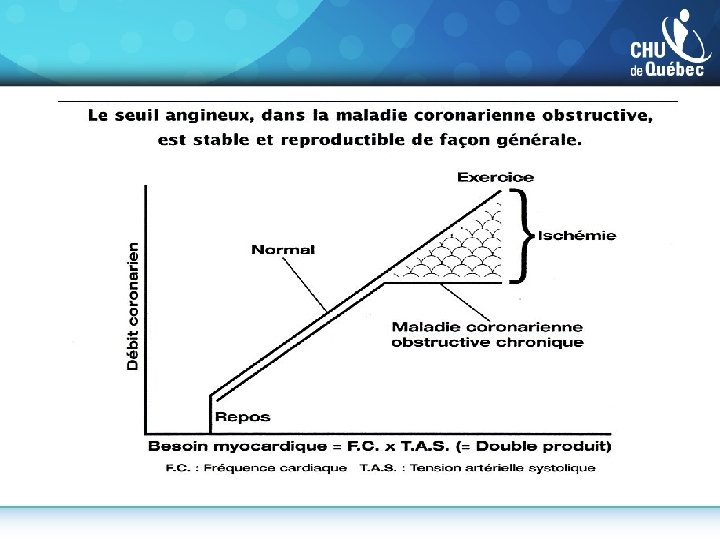
Double Produit FC: Fréquence Cardiaque x TAS: Tension artérielle systolique METS

ECG d’effort …positif/négatif à oublier § § § § Homme 38 ans, non fumeur. . . actif: tennis, ski TA 128/76 Glycémie 5, 2 Hb. A 1 c 0, 46 LDL 2, 8 HDL 2, 2 Longévité famille, profil et urine normaux, etc. Vie $5 millions, homme-clé, 25% Exigences: ECG effort …

ECG d’effort …positif/négatif à oublier § § § § Homme 38 ans, non fumeur. . . actif: tennis, ski TA 128/76 Glycémie 5, 2 Hb. A 1 c 0, 46 LDL 2, 8 HDL 2, 2 Longévité famille, profil et urine normaux, etc. Vie $5 millions, homme-clé, 25% ECG effort : ST , sous décalé 1, 5 mm , 15 minutes , aucun symptôme

ECG d’effort. . . positif/négatif à oublier § § § Femme 52 ans , non fumeuse. . Suivi cardio x 3 ans : angine stable 2/4 Glycémie 5, 2 Hb. A 1 c 0, 46 LDL 1, 8 HDL 1, 6 Ta 128/76 Rx : ASA 80 mg-EC, Rovustatin 10 mg , Périndopril 8 mg, TNT-spray ( jamais ) § ECG repos Normal § Vie $ 1 million , femme-clé , 25% § Exigences ; ECG effort

ECG d’effort. . . positif/négatif à oublier § § § § § Femme 52 ans , non fumeuse. . Suivi cardio x 3 ans : angine stable 2/4 Glycémie 5, 2 Hb. A 1 c 0, 46 LDL 1, 8 HDL 1, 6 Ta 128/76 Rx : ASA 80 mg-EC, Rovustatin 10 mg , Périndopril 8 mg, TNT-spray ( jamais ) ECG repos Normal Vie $ 1 million , femme-clé , 25% Exigences ; ECG effort ECG d’effort : 6 minutes , cliniquement et électriquement négatif

Théoreme de Bayes
 Severe")
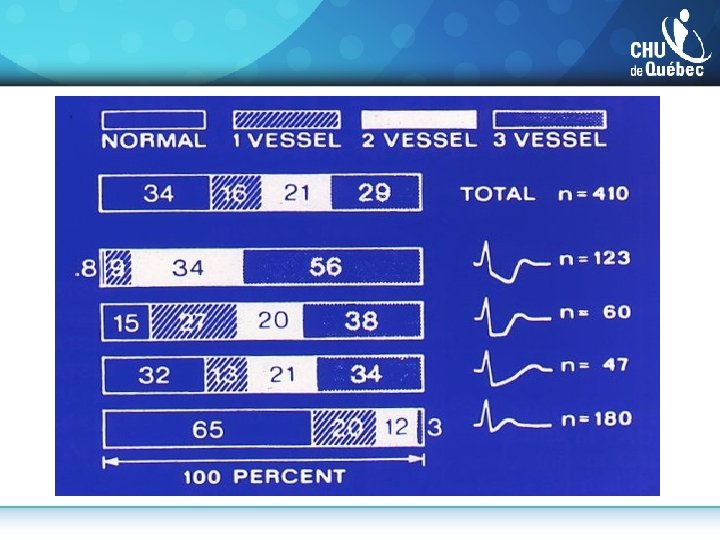
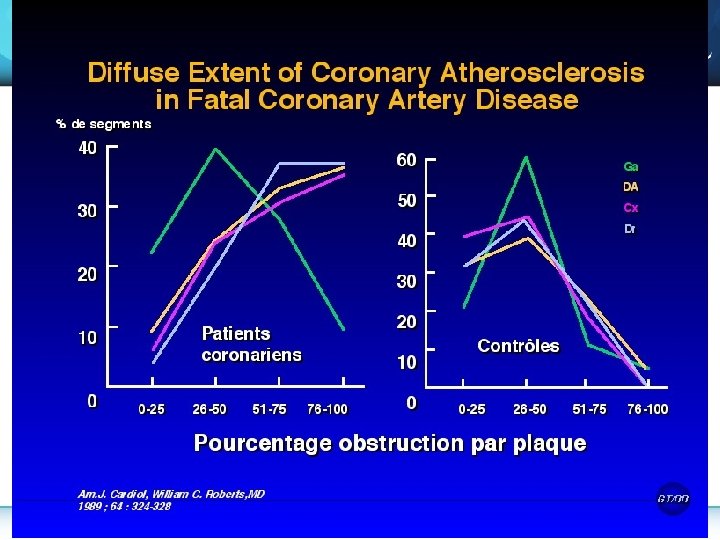
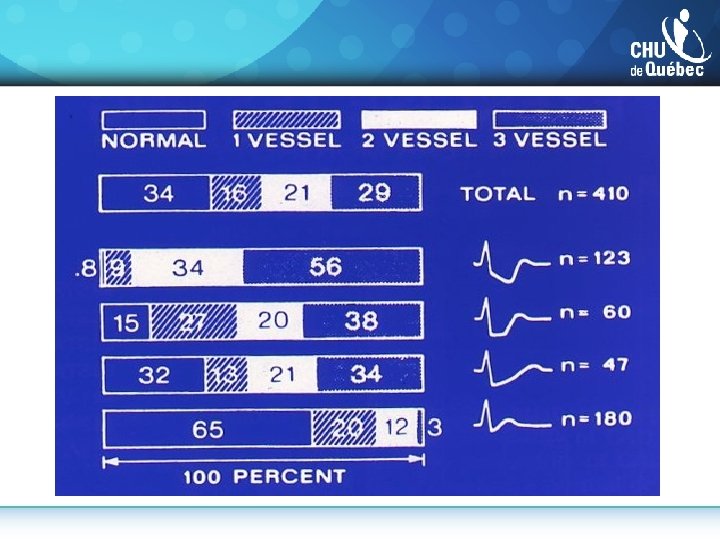
Lesion Severity: An Imperfect Predictor of Survival Angiographically insignificant disease ( 50% stenosis) Severe CAD ( 70% stenosis in all three coronary arteries) From the Coronary Artery Surgery Study (CASS) as reported by Little et al. Clin Cardiol 1991.

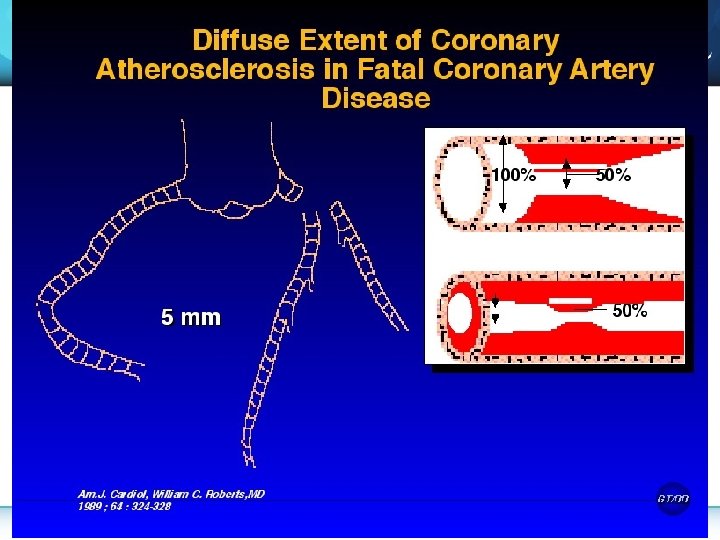
Angiography Underestimates Diffuse Disease Nissen et al. Textbook of Cardiovascular Medicine, 1998. Topol et al. Circulation 1995.

Most Acute MI’s Are Associated With Less Severe Stenoses % Patients Severity of Coronary Artery Stenosis Before Acute MI (n=195) <50 50 -70 % Diameter Stenosis Data from 4 studies. Smith. Circulation. 1996; 93: 2205 -2211. >70

IVUS coronarien Rotating transducer Anatomie coronarienne normale Images courtesy of Cleveland Clinic Intravascular Ultrasound Core Laboratory IVUS=intravascular ultrasound These slides are intended for education only and have been provided on request by Astra. Zeneca Scientific Affairs. A

Hypothèse de Glagov sur le remodelage coronarien Progression L’extension compensatrice maintient le diamètre de la lumière Vaisseau normal Coronaropathie bénigne Coronaropathie modérée Régression D’après Glagov et coll. N Engl J Med, 1987; 316: 1371 -75. Arrêt de l’extension : rétrécissement de la lumière Coronaropathie grave

Dialogues in Cardiovascular Medicine – Vol 19, No. 1, 2014

La plaque vulnérable…

Population en santé Manifestation initiale • • • Transition SCA mort subite angine instable MCOC infarctus aigu défaillance MCOC angine macro-vasculaire angine micro-vasculaire Défaillance post-infarctus post PAC post-angioplastie Décès • SCA Mort subite • • Défaillance cardiaque chronique Mort subite Décès autres causes vasculaire non-vasculaire

ECG à l'effort et diagnostic MCAS • Sensibilité du test = ? ? • Spécificité du test = ? ? • Cependant avec études évitant biais § Sensibilité = 55 à 70 % environ § Spécificité = 75 à 90 % environ

La coronarographie ne permet pas de visualiser le remodelage coronarien 3, 1 mm

Estimates of Sensitivity and Specificity for Non-Invasive Cardiac Tests for the Diagnosis of Coronary Artery Disease Technology Sensitivity Specificity Exercise Treadmill 0. 68 (0. 23 -1. 0) 0. 77 (0. 17 -1. 0) Attenuation Corrected SPECT 0. 86 (0. 81 -0. 91) 0. 82 (0. 75 -0. 89) Gated SPECT 0. 84 (0. 79 -0. 88) 0. 78 (0. 71 -0. 85) Traditional SPECT 0. 86 (0. 84 -0. 88) 0. 71 (0. 67 -0. 76) Contrast Stress Echocardiography (wall motion) 0. 84 (0. 79 -0. 90) 0. 80 (0. 73 -0. 87) Exercise or Pharmacologic Stress Echocardiography 0. 79 (0. 77 -0. 82) 0. 84 (0 -. 82 -0. 86) Cardiac Computed Tomographic Angiography 0. 96 (0. 94 -0. 98) 0. 82 (0. 73 -0. 90) Positron Emission Tomography 0. 90 (0. 88 -0. 92) 0. 88 (0. 85 -0. 91) Cardiac MRI (perfusion) 0. 91 (0. 88 -0. 94) 0. 81 (0. 75 -0. 87) Adapted from Gianrossi et al Circulation 1989; 80: 87 -98, Medical Advisory Secretariat 2010; 10: 1 -40, and Mc. Ardle et al J Am Coll Cardiol 2012; 60: 1828 -37

Prediction of Survival by Exercise Duration Non-Surgical Patients CAD Patients 100 90 90 80 80 % Survival 100 Stage IV Stage III Stage II 70 70 60 60 50 50 Mc. Neer, Circulation 1978; 57: 64 12 24 36 48 Stage I 12 Time (months) 24 36 48

Nomogramme de Mark & Pryor Sous-décalage du segment ST au cours du test Indice d’ischémie Présence d’angine au cours du test Pronostic Taux de survie de 5 ans Taux moyen de mortalité annuelle Durée du test MET Min 0 Non 1 Présente mais peu sévère 2 Interruption en raison d’angine sévère 2 4 5 3 TAUX DE SURVIE 1 Index angineux 0 1 2 Pas de douleur Douleur angineuse Épreuve d’effort cessé à cause de la douleur ge 50 ans 55 ans 60 ans 65 ans Survie 5 ans (%) Hommes Femmes 97 95 91 87 98 97 96 93 74

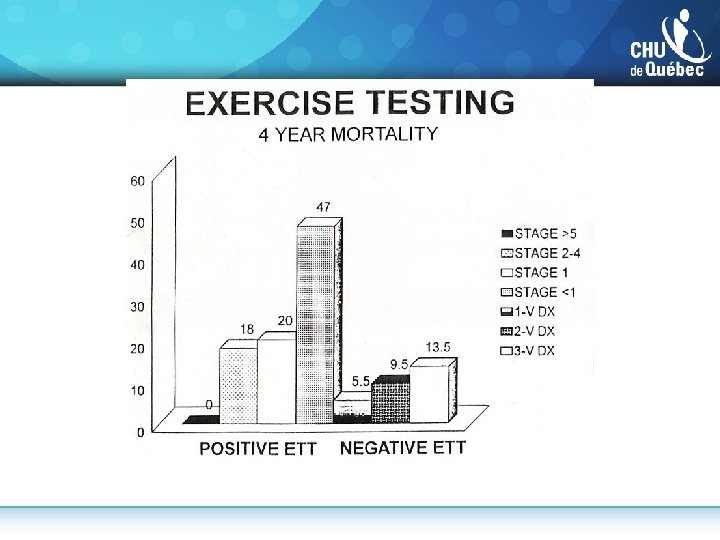
Incremental Risk Stratification for Cardiac Events in Patients Without Known CAD 10. 0* 8. 9* 9. 1 Event rate (%) 7. 8* Scan Results Normal Mildly abnormal Severely abnormal 6. 4 3. 6 1. 8 0. 4 0. 3 n= 762 113 Low (0. 9%) 51 * p < 0. 05 834 185 168 28 22 40 Intermediate High (2. 5%) (7. 7%) Duke Treadmill Score (DTS) Hachamovitch, Circulation 1996; 93: 908

Use of non-invasive testing for diagnostic and prognostic purposes in patients with classical anginal chest pain symptoms suggestive of SIHD. Stable Chest Pain Syndrome (1 – 3/3 anginal symptoms) Cardiovascular history, physical, laboratory tests, 12 lead EKG 2 or 3/3 Chest pain criteria 1/3 Chest pain criteria Male ≥ 40 yo Female ≥ 60 yo or single severe or multiple risk factors Non-invasive testing for diagnostic and/or prognostic purposes (tailored to patient characteristics, access and local expertise) Significant non-CV comorbidities and quality of life issues are present Male < 40 yo Female < 60 yo No risk factors Assess for other causes as appropriate Conservative diagnostic and treatment strategy

2014 CCS Guidelines on the Diagnosis and Management of Stable Ischemia Heart Disease Guidance for selection of an initial non-invasive test for diagnosing suspected CAD in routine practice settings. Able to exercise adequately and no contraindications (see legend) YES NO ECG abnormal (eg. ST depression ≥ 1 mm, LVH, digoxin, ventricular pre-excitation ECG normal No LBBB or ventricular paced rhythm Exercise stress test Exercise echocardiography Exercise myocardial perfusion imaging LBBB or ventricular paced rhythm Vasodilator myocardial perfusion imaging ECG normal or abnormal No LBBB or ventricular paced rhythm Dobutamine or vasodilator echocardiography Mancini GBJ, Gosselin G, et al. , Can J Cardiol 2014 Copyright © 2014, Canadian Cardiovascular Society LBBB or ventricular paced rhythm Vasodilator myocardial perfusion imaging Cardiac computed tomographic angiography

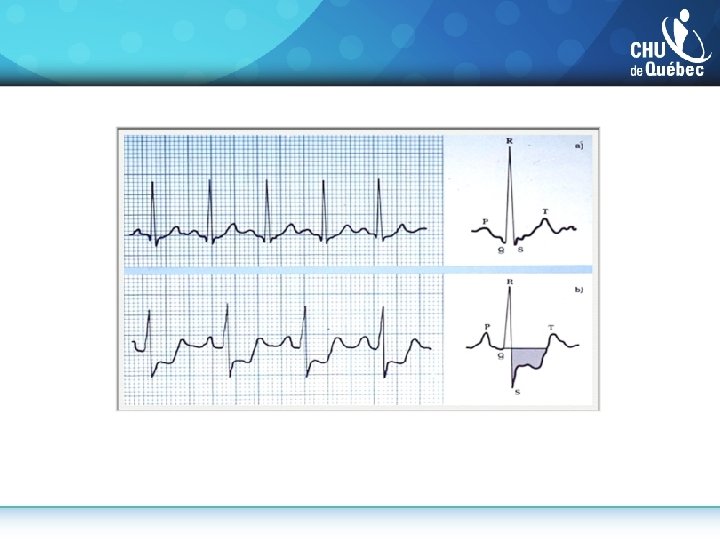
High Risk Features of Noninvasive Test Results Associated with > 3% Annual Rate of Death or MI Exercise Treadmill • ≥ 2 mm of ST-segment depression at low (< 5 metabolic equivalents, METS) workload or persisting into recovery • Exercise-induced ST-segment elevation • Exercise-induced VT/VF • Failure to increase systolic blood pressure to > 120 mm Myocardial Perfusion Imaging • Severe resting LV dysfunction (LVEF < 35%) not readily explained by non-coronary causes • Resting perfusion abnormalities ≥ 10% of the myocardium in patients without prior history or evidence of MI • Severe stress-induced LV dysfunction (peak exercise LVEF <45% or drop in LVEF with stress ≥ 10%) • Stress-induced perfusion abnormalities encumbering ≥ 10% myocardium or stress segmental scores indicating multiple vascular territories with abnormalities • Stress-induced LV dilation • Increased lung uptake Stress Echocardiography • Inducible wall motion abnormality involving >2 segments or 2 coronary beds • Wall motion abnormality developing at low dose of dobutamine (< 10 micrograms/kg/min) or at a low heart rate (<120 beats/min) Coronary Computed Tomographic Angiography • Multivessel obstructive CAD or left main stenosis on CCTA Adapted from Fihn et al Circ 2012; 126: e 354 -e 471

Théorème de Bayes

Théorème de Bayes

Théorème de Bayes

Théorème de Bayes

Prévalence < 4% ECG d’effort et prévalence 4% Sensibilité 70% Spécificité 80% + - 40 m 28 12 960 s 192 768 28/220 VPP = 13% 12/780 VPN = 98%

Prévalence 73% Sensibilité 70% ECG d’effort et prévalence 73% Spécificité 80% + - 730 m 510 220 270 s 54 216 510/564 VPP = 90% 216/436 VPN = 50%

Théorème de Bayes
 study Ø 70% stenosis +")
Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) study Ø 70% stenosis + evidence of myocardial ischemia; Øor >80% stenosis and classic angina. Ø 35000 screened 6. 4% enrolled ØExclusion: LMC, EF<30% (35% if 3 VD), marked ischemia ØBoth arms: intensive control of lipids, blood pressure, and blood glucose and counseling on lifestyle factors, such as nutrition, exercise, and smoking Dr Per Anton Sirnes. (NO) CCP 54 54
 CCP 55 55")
COURAGE NEJM. 2007; 356: 1503 -1516 Dr Per Anton Sirnes. (NO) CCP 55 55

Comprehensive CV risk Management : BARI- 2 D JACC Vol 66, no 7, 2015 -august 19

Comprehensive CVD Risk Management : BARI 2 D JACC Vol 66, no 7 , 2015 -august 19

Comprehensive CVD Risk Management : BARI 2 D JACC Vol 66, no 7 , 2015 -august 19

2014 CCS Guidelines on the Diagnosis and Management of Stable Ischemia Heart Disease Absolute Annualized Event Rate “Warranty Period” of Normal CT extends to 7 years N>10, 000 5 yr f/u N=2, 538 N=1, 304 6. 5 yr f/u 4. 3 yr f/u Mancini GBJ, Gosselin G, et al. , Can J Cardiol 2014 Copyright © 2014, Canadian Cardiovascular Society Source: Ostrom et al. J Am Coll Cardiol 2008; Andreini et al. JACC Imaging 2012; Hadamitzky et al. Eur Heart J 2013; N=1, 584 5. 6 yr f/u
- Slides: 59