ECG Lecture Scott Ewing D O March 23


 secondary to renal failure Findings consistent")







 prominent U waves with Q-T(U) prolongation He")


- Slides: 18
ECG Lecture Scott Ewing, D. O. March 23, 2006
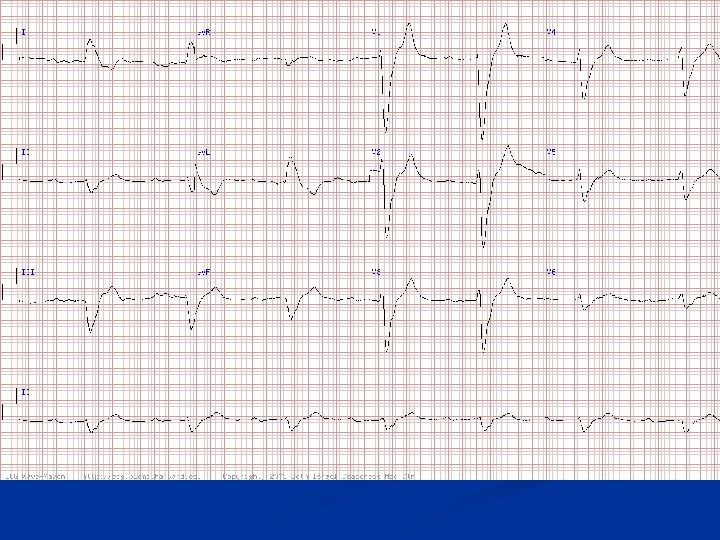
Question #1 n The patient is an elderly man who presented to the emergency ward with dizziness and new renal failure
Hyperkalemia n n Hyperkalemia (7. 6 m. Eq/L) secondary to renal failure Findings consistent with severe hyperkalemia n n Widening of the QRS complex Peaking of the T waves Prolongation of the PR interval and flattening of the P waves If left untreated, the ECG will progress to a sinusoidal pattern and eventually asystole with subsequent hemodynamic collapse and death
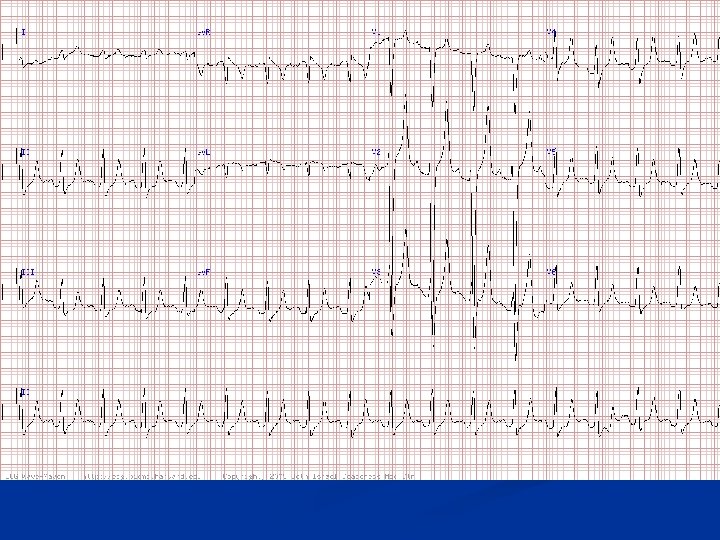
Question #2 A 65 -year-old man n What should you do before calling cardiology fellow for a "hyperacute myocardial infarction" here? n
Hyperkalemia n n n Classic hyperkalemia with tall peaked T waves, along with PR prolongation and underlying left ventricular hypertrophy (LVH) (patient has renal disease with hypertension) Note QRS prolongation also seen with moderate-severe hyperkalemia Potassium here was 9. 6 m. Eq/L Not all tall positive T waves are "hyperacute“ The latter term should be reserved for increased T wave positivity secondary to transmural ischemia Major clues include narrowness (tenting) of T waves along with other findings noted above
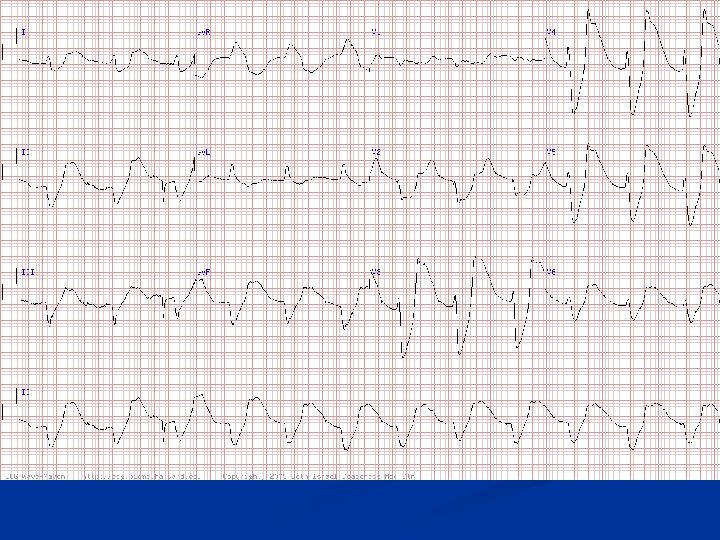
Question #3 n This ECG is most consistent with which diagnosis? A. B. C. D. E. Acute anterior myocardial infarction Accelerated idioventricular rhythm Marked hyperkalemia Marked hypercalcemia Systemic hypothermia
Hyperkalemia The K+ was 10. 5 m. Eq/L in a patient with renal failure n Note the wide QRS complexes with no evident P waves n CK was normal and ST elevations were likely due to hyperkalemia. (Note: The apparent spike after the second QRS complex is an artifact. ) n
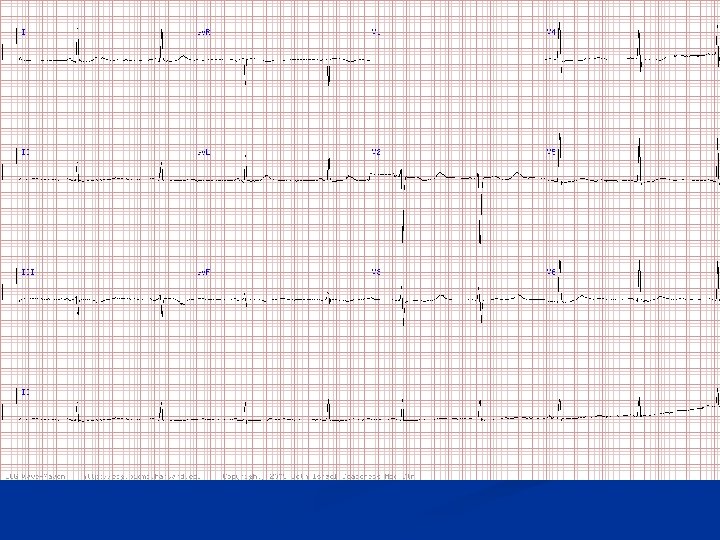
Question #4 A 38 -yr-old woman n What does the ECG show and what is the differential diagnosis? n
Hypokalemia n n n Sinus bradycardia with diffuse T wave flattening or inversions and markedly prominent U waves Best seen in leads V 2 and V 3 Most common causes n n Hypokalemia (K+ here was 2. 4 m. Eq/L) Drugs such as quinidine, phenothiazines, tricyclics Patients with hereditary long QT syndromes may show a similar finding This pattern is of great importance because it identifies patients at high risk of torsade de pointes type of polymorphic ventricular tachycardia
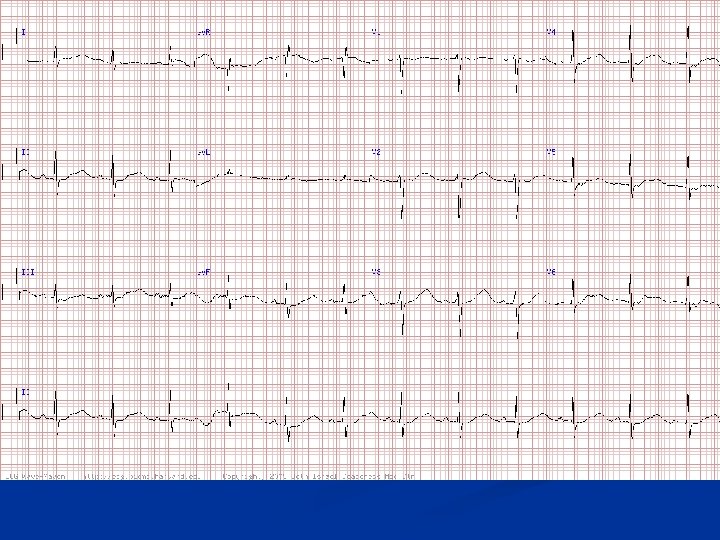
Question #5 30 -yr-old man with diarrhea, not on medication n What waveform is prominent? n What is the diagnosis? n
Hypokalemia n n There are very (!) prominent U waves with Q-T(U) prolongation He had severe hypokalemia (1. 5 m. Eq/L) due to diarrhea Calcium was normal, as was magnesium (remember pure hypocalemia prolongs ST segment primarily but doesn't give large U waves. ) Obviously, this acquired-type long-QT(U) syndrome puts subject at risk for torsade de pointes which he fortunately did not have before coming to hospital
Hyperkalemia n n ECG changes have a sequential progression of effects, which roughly correlate with the potassium level ECG findings may be observed as follows: n n n Early changes include peaked T waves, shortened QT interval, and ST segment depression Followed by bundle branch blocks causing a widening of the QRS complex, increases in the PR interval, and decreased amplitude of the P wave These changes reverse with appropriate treatment Without treatment, the P wave eventually disappears and the QRS morphology widens to resemble a sine wave. Ventricular fibrillation or asystole follows. ECG findings generally correlate with the potassium level, but potentially life-threatening arrhythmias can occur without warning at almost any level of hyperkalemia.
Hypokalemia n ECG findings may be observed as follows Flattening of the T wave, which is the earliest change n A "U wave" then develops, associated with ST-T wave flattening and sometimes slight ST depression n ST depression is more noticeable and the U wave increases in amplitude until ultimately the U wave overtakes the T wave. n At this point distinguishing between the T wave and U wave may be almost impossible ("Q-U" prolongation). n