ECG Interpretation Criteria Review Axis Deviation Left Right


 Normal Positive LAD")


 show wide P waves • •")








 Complete occlusion")










 ✦ Persistent ST segment depression")


 1. Normal conduction 2. Conducted with aberration ✦ a fascicles")


")









 PVCs ✦ same appearance in the same lead ✦ small")
 PVCs ✦ different appearance in the same lead")







- Slides: 51
ECG Interpretation Criteria Review
Axis Deviation Left Right ✦ ✦ RAD = If R wave in III > R wave in II LAD = If R wave in a. VL > I; and deep S wave in III
Axis Deviation Criteria LEAD II (or Lead a. VF or III) Normal Positive LAD Positive Negative RAD Negative Positive Intermediate axis Negative
Axis Deviation ✦ LAD = possible left anterior fasicular block ✦ RAD = possible left posterior fasicular block
Right Atrial Abnormality Criteria ✦ Tall P waves in lead II ✦ (or III, a. VF and sometimes V 1)
Left Atrial Abnormality • Lead II (and I) show wide P waves • • • (second hump due to delayed depolarization of the left atrium) (P mitrale: mitral valve disease) V 1 may show a bi-phasic P wave • • 1 box wide, 1 box deep (biphasic since right atria is anterior to the left atria)
Right Ventricular Hypertrophy Criteria 1. In V 1, R wave is greater than the S wave - or - R in V 1 greater than 7 mm 2. Right axis deviation 3. In V 1, T wave inversion (reason unknown)
Left Ventricular Hypertrophy Criteria ✦ If S wave in V 1 or V 2 + R wave in V 5 or V 6 ≥ 35 mm. . . ✦ . . . or, R wave > 11 (or 13) mm in a. VL or I. . . ✦ . . . or, R in I + S in III > 25 mm. ✦ Also ✦ LVH is more likely with a “strain pattern” or ST segment changes ✦ Left axis deviation ✦ Left atrial abnormality
Right Bundle Branch Block Criteria ✦ V 1 or V 2 = r. SR’ - “M” or rabbit ear shape ✦ V 5 or V 6 = q. RS ✦ Large R waves ✦ Right chest leads: T wave inversion (“secondary changes” since they reflect a delay in depolarization not an actual change in depolarization). ✦ Complete RBBB: QRS > 0. 12 sec. ✦ Incomplete RBBB: QRS = 0. 10 to 0. 12 sec.
Left Bundle Branch Block Criteria ✦ Wide QRS complex ✦ V 1 = QS (or r. S) and may have a “W” shape to it. ✦ ✦ V 6 = R or notched R and may show a “M” shape or rabbit ears Secondary T wave inversion ✦ Secondary if in lead with tall R waves ✦ Primary if in right precordial leads
Incomplete Bundle Branch Blocks ✦ RBBB or LBBB where QRS is between. 10 and. 12 with same QRS features
Left Anterior Fascicular Block ✦ Limb leads ✦ QRS less width less than 0. 12 sec. ✦ QRS axis = Left axis deviation (-45° or more) ✦ if S wave in a. VF is greater than R wave in lead I ✦ small Q wave in lead I, a. V , or V 6 L
Left Posterior Fascicular Block ✦ ✦ ✦ Right axis deviation (QRS axis +120° or more) S wave in lead I and a Q wave in lead III (S 1 Q 3) Rare
Bifascicular Block ✦ ✦ Two of the three fascicles are blocked. Most common is RBBB with left anterior fascicular block.
Subendocardial Ischemia Partial occlusion Transmural Infarction (MI) Complete occlusion
✦ ✦ ✦ A. Normal ECG prior to MI B. Hyperacute T wave changes - increased T wave amplitude and width; may also see ST elevation C. Marked ST elevation with hyperacute T wave changes (transmural injury) D. Pathologic Q waves, less ST elevation, terminal T wave inversion (necrosis) E. Pathologic Q waves, T wave inversion (necrosis and fibrosis) F. Pathologic Q waves, upright T waves (fibrosis)
Infarction
Anterior Infarctions ✦ ✦ Abnormal Q waves in chest leads Anterior MI can show loss of R wave progression in the chest leads
Inferior Infarctions ✦ Abnormal Q waves in leads II, III, and a. VF
Lateral ✦ ✦ Lateral - V 5 and V 6 High lateral when ST elevation and Q waves localized to leads I and a. VL
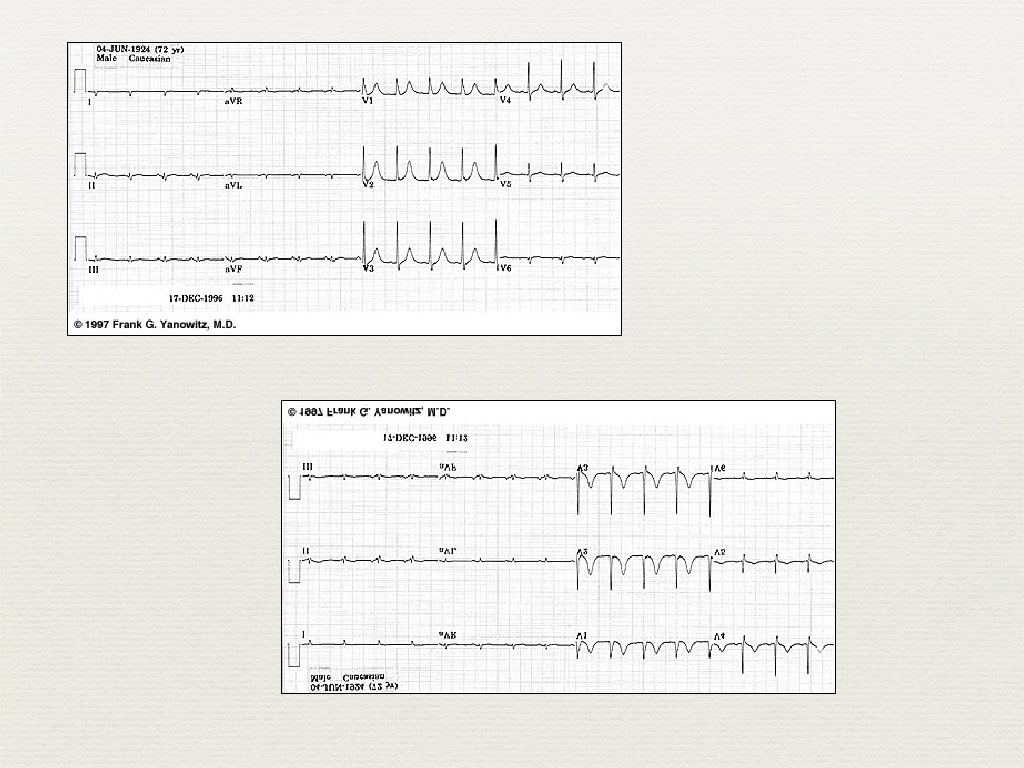
Posterior MI ✦ Tall R waves in V 1, V 2 ✦ ✦ ✦ R/S ratio > 1 in V 1, V 2 The tall, anterior R waves are mirror images of a pathological, posterior Q waves. Absences of right axis deviation (found with RVH) ✦ ST segment depression in V 1 -V 3 ✦ Often seen with inferior MI
Infarctions or BBB ✦ RBBB & LBBB ✦ ✦ T wave inversion and ST segment depression in V 1 & V 2 (RBBB) and V 5 & V 6 (LBBB) MI ✦ ✦ T wave inversion and ST segment depression in additional leads Likely loss of R wave progression
Infarctions and BBB ✦ RBBB and MI ✦ ✦ usual ECG changes in leads other than V 1 and V 2 septal MI - upright T waves in V 1 and V 2 ✦ with just RBBB the T waves should be inverted so upright T waves w/ RBBB are “abnormal” and indicated septal MI
Infarctions and LBBB ✦ ✦ ✦ Infarctions often damage the left bundle branch leading to a new or recent LBBB expect to see upright T waves in left chest leads septal MI are very difficult to assess with LBBB
Subendocardial Ischemia ✦ ST Segment depression ✦ ✦ ✦ Anterior leads (I, a. Vl and V 1 -V 6) Inferior leads (II, III, and a. Vf) may see ST segment elevation in a. Vr ✦ T wave inversion ✦ Poor R wave progression
Subendocardial Infarction ✦ No Q waves (non-Q wave infarction) ✦ Persistent ST segment depression ✦ T wave inversion
Sinus Bradycardia ✦ HR less than 60 bpm
Sinus Tachycardia ✦ HR > 100 bpm
Premature Atrial Complexes (PAC) 1. Normal conduction 2. Conducted with aberration ✦ a fascicles or bundle branch is refractory ✦ wide QRS 3. Non-conducted ✦ ✦ the AV node was still refractory; P wave will be close to the T wave no QRS complex
Atrial Tachycardia
AV Nodal Reentrant Tachycardia Figure 14 -6 ✦ ✦ ✦ Rapid recirculating impluse in the AV node area (140 -250 beats/min) No P waves (hidden in QRS complex) or may be just before or after the QRS complex Negative P waves in lead II
Atrial Flutter ✦ Sawtooth; F waves (easiest seen in II, III, & a. VF) ✦ Atrial rate of about 300 bpm ✦ Ventricular rate 150, 100 or 75 beats/min ✦ 2: 1, 3: 1 and 4: 1
Atrial Fibrillation ✦ ✦ No organized depolarization in atria. Irregular “f waves” can range from looking almost like P waves to a flat line. Atrial rate is about 600 bpm Normal QRS w/ ventricular rate ~110 -180 but random & irregular
Junctional Rhythm
Accelerated Junctional Rhythm
WPW
First Degree AV Block
2 nd Degree AV Block, Type 1
2 nd Degree AV Block, Type 2
2 rd Degree AV Block
Premature Ventricular Contractions ✦Characteristics 1. Premature and occur before the next normal beat 2. Wide (> 0. 12 ms) and the T wave is usually opposite of the QRS 3. Bizarre looking ✦ PVCs usually precede a P wave. ✦ A nonsinus P wave may follow the PVC
PVC ✦ Unifocal (monomorphic) PVCs ✦ same appearance in the same lead ✦ small focus ✦ normal and diseased hearts
PVC ✦ Polymorphic (multifocal and multiform) PVCs ✦ different appearance in the same lead ✦ multiform = different coupling intervals ✦ multifocal = same coupling intervals ✦ usually diseased hearts Multiform
Idioventricular Rhythm
Couplet
Triplet
Bigeminy and Trigeminy
Ventricular Tachycardia. . . more than three PVCs
Torsades de Pointes
Ventricular Fibrillation Note the course and fine waves