ECG DYSRHYTHMIAS Nancy Lin RN MSN Reading Assignment





 Detects electrical activity of heart ¢ Components of an ECG waveform ¢")










 Atrial depolarization b) Atrial repolarization c)")

































 Channel Blockers Dec. fast sodium influx to cardiac cells ¢")





 channel blocker that blocks calcium")

. Wong’s Nursing care of infants and")
- Slides: 62
ECG/ DYSRHYTHMIAS Nancy Lin, RN, MSN
Reading Assignment ¢ Wong’s l ¢ Lewis l ¢ Cardiac dysrhythmias: pp. 1311 -1313 EKG’s: CH 36 Adams & Urban: Pharmacology Antidysrhythmics CH 40
SLO’s ¢ ¢ ¢ Relate electrocardiogram changes to common cardiac problems. Discuss conduction system and electrocardiographic monitoring in pediatric and adult clients. Introduction to assessment of normal and abnormal cardiac rhythm and appropriate treatment in pediatric and adult clients. Compare and contrast nursing and collaborative management of pediatric and adult clients with common dysrhythmias. Discuss nursing management of pediatric and adult patients with central venous access.
Lecture Content EKG’s ¢ Cardiac Rhythms ¢ Pacemakers ¢ Defibrillation/Cardioversion ¢ Central Venous Access ¢
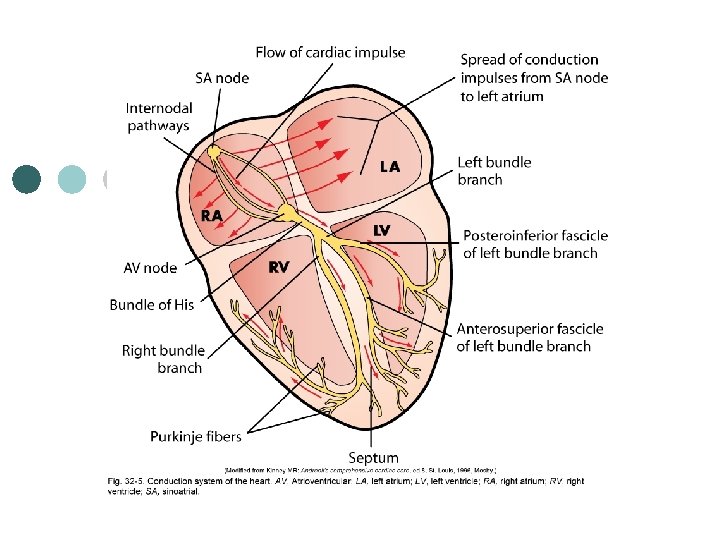
Conduction System of the Heart ¢ http: //highered. mcgrawhill. com/sites/0072495855/student_vie w 0/chapter 22/animation__conducting _system_of_the_heart. html
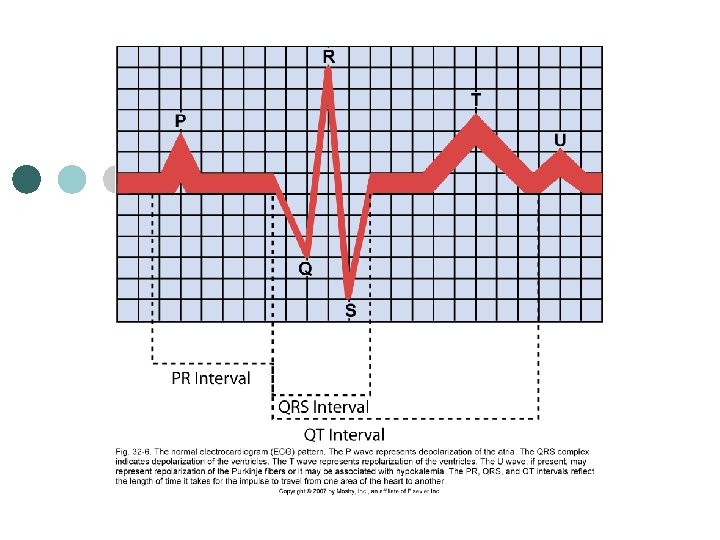
Electrocardiogram (ECG) Detects electrical activity of heart ¢ Components of an ECG waveform ¢ P wave l P-R interval l QRS complex l ST segment l QT interval l T wave l
P Wave ¢ P wave Begins with firing of SA node l Depolarization of atria l • atrial contraction. ¢ PR interval l time period for impulse to spread through atria, AV node, bundle of His & Purkinje fibers.
QRS Complex ¢ Depolarization from AV node throughout ventricles l ¢ ventricular contraction QRS interval l time it takes for depolarization
ST Segment ¢ Time between ventricular depolarization & repolarization
T wave Ventricle repolarization ¢ U wave ¢ l may represent repolarization of Purkinje fibers or assoc. with _______
Principle of ECG Formation
Calculating HR From ECG Count # of QRS complexes in 1 minute. ¢ Count # of R-R intervals in 6 seconds & multiply that # by 10. ¢
The ECG Paper
Intrinsic Rates of Conduction System SA node ¢ AV node ¢ Bundle of His, Purkinje fibers ¢
Rhythm analysis ¢ ¢ ¢ ¢ Basic rules that can be followed to identify a patient's heart rhythm. What is the rate? Is it regular or irregular? Are P waves present? Are QRS complexes present? Is there a 1: 1 ratio between P waves and QRS complexes? Is the PR interval constant?
Questions to Consider 1. What is the dominant rhythm and/or dysrhythmia? ¢ 2. What is the clinical significance of the findings? ¢ 3. What is the treatment for the particular rhythm? ¢
Self Assessment ¢ A QRS complex represents: a) Atrial depolarization b) Atrial repolarization c) Ventricular depolarization d) Ventricular repolarization
Pediatric ECG ¢ Normal pediatric ECG: l an ECG that contains a P wave, a QRS complex normal for age and less than or equal to 0. 08 second, and a T wave.
Dysrhythmias Caused by disorders of impulse formation ¢ Cause of a dysrhythmia influences treatment of patient. ¢ Common causes: Cardiac conditions Other conditions ¢
Dysrhythmias ¢ In children Occur with CHD l Follow surgical repair of CHD l Cardiomyopathy l Cardiac tumors l Metabolic & electrolyte imbalances l Genetic etiology l
Dysrhythmias ¢ Naming of most cardiac rhythms begin with the site that the impulse originated.
Normal Sinus Rhythm Originates in SA node ¢ Follows normal conduction pattern of cardiac cycles ¢ Rhythm: Regular ¢ Rate: 60 -100 bpm ¢ QRS normal ¢ P Wave – visible before each QRS complex ¢ P-R interval: normal (<5 small squares) ¢
Normal Sinus Rhythm ¢ ¢ ¢ ¢ 1, P wave 2, PR interval 3, QRS complex 4, ST segment 5, T wave 6, QT interval Isoelectric (flat) line
Sinus Bradycardia ¢ ¢ ¢ ¢ Conduction pathway same as in NSR SA node fires at a rate <60 beats/minute May be normal in Rhythm – Regular Rate – Less than 60 beats per minute QRS Duration – Normal P Wave – visible before each QRS complex P-R Interval – Normal Usually benign & often caused by pts on Beta blockers
Sinus Tachycardia ¢ ¢ ¢ Rate: >100 beats/minute QRS Duration – Normal P Wave – Visible before each QRS complex P-R Interval – Normal Impulse generating heart beats are nl, but are occurring at faster pace than nl. Seen during exercise.
Premature Atrial Contraction ¢ ¢ ¢ Contraction originating from an ectopic focus Ectopic signal originates in left or right atrium & travels across atria by an abnormal pathway, creating a distorted P wave. Clinical Associations ECG Characteristics Clinical Significance Treatment
Paroxysmal Supraventricular Tachycardia ¢ ¢ ¢ ¢ ¢ Dysrhythmia originating in an ectopic focus anywhere above bifurcation of bundle of His Paroxysmal: abrupt onset & termination Some degree of AV block may be present Can occur in presence of Wolff-Parkingson-White (WPW) syndrome Rhythm: Regular or sl irregular Rate – 100 -300 beats per minute QRS Duration – usually normal P Wave – often buried in preceding T wave PR interval – may be shortened or nl
Atrial Flutter ¢ ¢ ¢ ¢ An atrial tachydysrhythmia Recurring, regular, sawtooth-shaped flutter waves Originates from a single ectopic focus in right atrium. Atrial Rate – about 250 -300 beats per minute QRS Duration – usually normal P Wave – Replaced with multiple F (flutter) waves, usually 2: 1, but sometimes 3: 1 P-R interval: not measurable Atrial flutter with a 4: 1 conduction (four flutter [F] waves to each QRS complex)
Atrial Fibrillation ¢ ¢ ¢ ¢ ¢ Total disorganization of atrial electrical activity due to multiple ectopic foci resulting in loss of effective atrial contraction. May be chronic or intermittent Most common dysrhythmia in US Rhythm – irregularly irregular Atrial Rate – 350 to 600 beats/min, can be slower QRS duration – usually normal P Wave – not distinguishable as atria are firing off all over P-R interval – not measurable The atria fire electrical impulses in irregular fashion causing irregular heart rhythm
First-Degree AV Block ¢ Every impulse is conducted to ventricles but duration of AV conduction is prolonged. After impulse moves through AV node, it is usually conducted normally through ventricles. Rhythm – regular Rate – normal QRS Duration – normal P Wave – Ratio 1: 1 P Wave Rate – Normal P-R interval – prolonged Z(>5 small squares) ¢ First-degree AV heart block with a PR interval of 0. 40 seconds. ¢ ¢ ¢ ¢
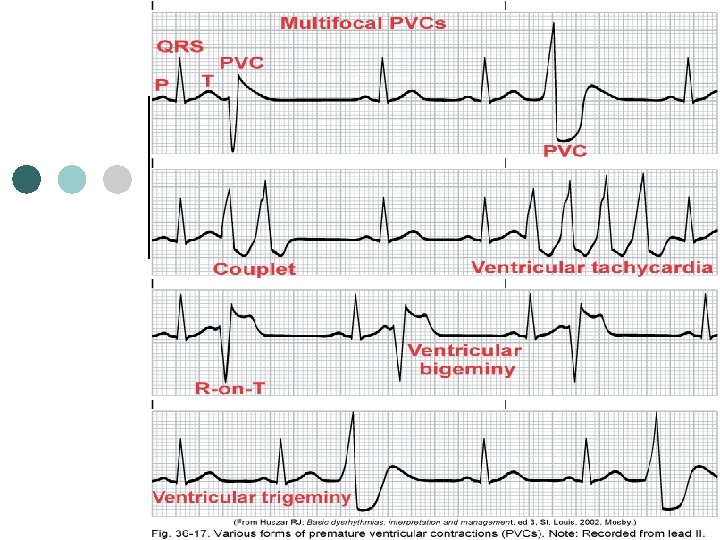
Premature Ventricular Contraction ¢ ¢ ¢ ¢ A contraction originating in an ectopic focus in the ventricles Premature occurrence of a QRS complex, which is wide & distorted in shape Multifocal PVCs: PVCs that are initiated from different foci appear different in shape from each other Unifocal PVCs: PVCs that appear to have same shape Ventricular bigeminy: when every other beat is a PVC Ventricular trigeminy: when every 3 rd beat is a PVC Couplet: two consecutive PVCs Three or more PVCs: Ventricular tachycardia
Premature Ventricular Contractions Clinical Associations ¢ ECG Charcteristics ¢ Clinical Significance ¢ Treatment ¢
Ventricular Tachycardia ¢ ¢ ¢ ¢ A run of three or more PVCs occur Different forms of VT exist, depending on QRS configuration Monomorphic VT Polymorphic VT May be sustained (lasts >30 sec) or nonsustained (<30 sec) Development of VT is an ominous sign A life threatening dysrhythmia
Ventricular Tachycardia ¢ ¢ Clinical Associations: ECG Characteristics: Ventricular rate 150 -250 beats/min. Rhythm: reg or irregular. AV dissociation may be present, with P waves occurring independently of QRS complex P wave usually buried in QRS complex PR interval: not measurable QRS: distorted, duration >12 sec R-R interval: may be irregular or regular
Ventricular Tachycardia ¢ Clinical Significance: Stable or unstable Sustained VT will cause severe dec. in CO Results: Dysrhythmia must be treated quickly Ventricular fibrillation may develop
Ventricular Tachycardia Treatment: - Identify & treat precipitating causes
Ventricular Tachycardia ¢ ¢ ¢ VT without a pulse is a life-threatening situation Treated in same manner as ventricular fibrillation CPR & defibrillation: 1 st line of Rx, followed by administration of epinephrine if defib unsuccessful.
Ventricular Fibrillation A severe derangement of heart rhythm ¢ Irregular undulations of varying shapes & amplitude ¢ Firing of multiple ectopic foci in ventricle ¢ Mechanically ventricle is simple “quivering”, no effective contraction, no CO occurs. ¢ Clinical Associations: • ECG Characteristics: HR not measurable Rhythm irregular & chaotic P wave: not visible PR & QRS interval not measurable. ¢
Ventricular Fibrillation Clinical Significance: results in an unresponsive, pulseless & apneic state Pt will die if not rapidly treated. • RX: Immediate CPR & ACLS measures w/use of defib & drug therapy. • This patient needs to be defibrillated!!! QUICKLY ¢
Asystole ¢ ¢ ¢ ¢ ¢ Total absence of ventricular electrical activity No ventricular contraction Pts are unresponsive, pulseless & apneic Lethal dysrhythmia Requires immediate treatment Poor prognosis Rhythm – flat Rate – 0 beats per minute QRS Duration – none P Wave - none
Asystole ¢ Clinical Associations: ¢ Clinical Significance: ¢ Treatment: Carry out CPR!!! Intubation Transcutaneous pacing IV therapy with epinephrine & atropine
Pulseless Electrical Activity Electrical activity can be observed on ECG, but there is no mechanical activity of ventricles & patient has no pulse. ¢ Poor prognosis ¢ Most frequent causes: ¢ Treatment: correct underlying cause. ¢
Defibrillation ¢ Most effective method of terminating VF & pulseless VT.
Defibrillation ¢ ¢ Monophasic: deliver energy in one direction Biphasic: deliver energy in two directions delivers successful shocks at lower energies & w/fewer post shock ECG abnormalities output measured in joules (watts/sec)
Synchronized Cardioversion
Implantable Cardioverter. Defibrillator
Pacemakers ¢ Indications ¢ Patient monitoring
ECG Changes Associated With Acute Coronary Syndrome ¢ ST segment, T wave, and Q wave changes associated with myocardial ischemia (A), injury (B), and infarction (C).
Resource ¢ ECG Simulator www. skillstat. com
Antidysrhythmics ¢ Used for l ¢ Prevention & Rx of cardiac rhythm disorders Classifications Group I drugs l Group III drugs l Group IV drugs l
Group I: Fast (Sodium) Channel Blockers Dec. fast sodium influx to cardiac cells ¢ Drug response ¢ Three groups: IA IB IC ¢
Group I-A Drugs ¢ Procainamide l l l Most widely used Reduces automaticity Slows electrical conduction & delays repolarization in atria, ventricles & Purkinje fibers Indicated for: ______________ Given IV or PO Side effects
Group I-B Drugs ¢ Lidocaine Major use in abolishing ventricular dysrhythmias l Administered IV l Contraindicated in _______ l Benefits l Adverse effect l
Group II: Beta-Blockers Decrease conduction velocity, automaticity & recovery time. ¢ Slows conduction through AV node ¢ Examples ¢ More frequently prescribed ¢
Group III: Prolong Repolarization ¢ ¢ Used in emergency treatment of ventricular dysrhythmias when other antidysrhythmics are ineffective. Examples Increase refractory period & prolong action potential duration (delay repolarization) Can significantly prolong QT interval & pose risk for ventricular dysrhythmias
Group III Drugs ¢ Amiodarone Most frequently used l Dec. automaticity l Prolongs AV conduction l Given IV or PO l Pregnancy safety category: D l Has serious adverse effects l ¢ Indicated for life-threatening VF & VT
Group IV: Calcium Channel Blockers Examples ¢ Slow (calcium) channel blocker that blocks calcium influx → ↓ excitability & contractility of myocardium. ↑ refractory period of AV node → ↓ ventricular response. ¢
Group IV Drugs ¢ Diltiazem l Indications l Adverse effects
References Hockenberry, M. J. & Wilson, D. (2015). Wong’s Nursing care of infants and children (10 th ed. ). St. Louis, MO: Mosby. Lewis, S. , Heitkemper, M. & Dirksen, S. (2014). Medical Surgical Nursing: Assessment and Management of Clinical Problems (9 th ed. ). St. Louis, MO: Mosby