ECG Dr Bernhard Arianto Purba M Kes AIFO

ECG Dr. Bernhard Arianto Purba, M. Kes. , AIFO

Textbooks • • • Guyton, A. C & Hall, J. E. 2006. Textbook of Medical Physiology. The 11 th edition. Philadelphia: Elsevier. Saunders: 918 -930, 961 -977. Brooks, G. A. & Fahey, T. D. 1985. Exercise Physiology. Human Bioenergetics and Sts Aplications. New York : Mac Millan Publishing Company: 122 -143. Foss, M. L. & Keteyian, S. J. 1998. Fox’s Physiological Basis for Exercise and Sport. 4 th ed. New York : W. B. Saunders Company: 471 -491. Astrand, P. O. and Rodahl, K. 1986. Textbook of Work Pysiology, Physiological Bases of Exercise. New York : Mc. Graw—Hill. Braunwald, Pauci, et al. 2008. Harrison's PRINCIPLES OF INTERNAL MEDICINE. Seventeenth Edition. New York : Mc. Graw—Hill: Chapter 332, 333, 338. Jardins, Terry Des. 2002. Cardiopulmonary Anatomy & Physiology. The 4 th edition. USA: Delmar, A Division of Thomson Learning Inc.
")
ELECTROCARDIOGRAPHY (ECG)

ECG
 is a time-varying signal")
A Brief introduction to ECG • • The electrocardiogram (ECG) is a time-varying signal reflecting the ionic current flow which causes the cardiac fibers to contract and subsequently relax. The surface ECG is obtained by recording the potential difference between two electrodes placed on the surface of the skin. A single normal cycle of the ECG represents the successive atrial depolarisation/repolarisation and ventricular depolarisation/repolarisation which occurs with every heart beat. Simply put, the ECG (EKG) is a device that measures and records the electrical activity of the heart from electrodes placed on the skin in specific locations

What the ECG is used for? • • Screening test for coronary artery disease, cardiomyopathies, left ventricular hypertrophy Preoperatively to rule out coronary artery disease Can provide information in the precence of metabolic alterations such has hyper/hypo calcemia/kalemia etc. With known heart disease, monitor progression of the disease Discovery of heart disease; infarction, coronal insufficiency as well as myocardial, valvular and cognitial heart disease Evaluation of ryhthm disorders All in all, it is the basic cardiologic test and is widely applied in patients with suspected or known heart disease
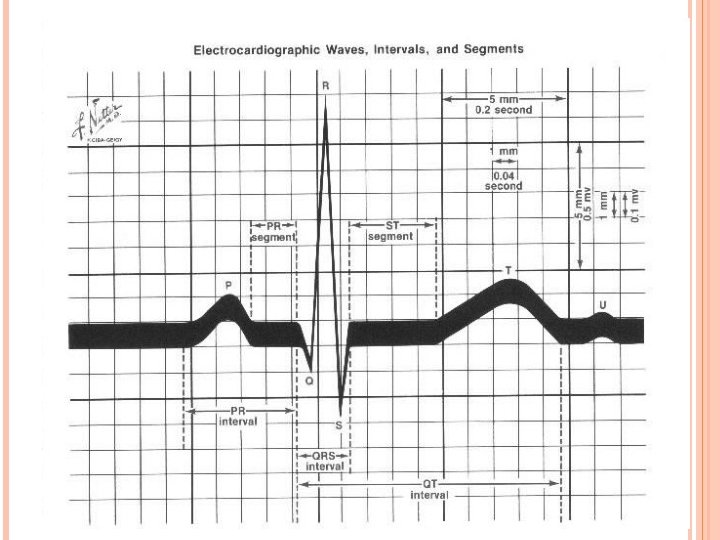

Each small box = 1 mm =. 04 Sec. 5 small boxes = 1 large box = 0. 2 Sec.

MEASURING ECG commonly measured via 12 specifically placed leads
")
Lead Configurations for ECG Measurement n n n Bipolar Leads Augmented Leads Chest (V) Leads

Bipolar Leads: lead I + _

Bipolar Leads: lead II + _

Bipolar Leads: lead III + _

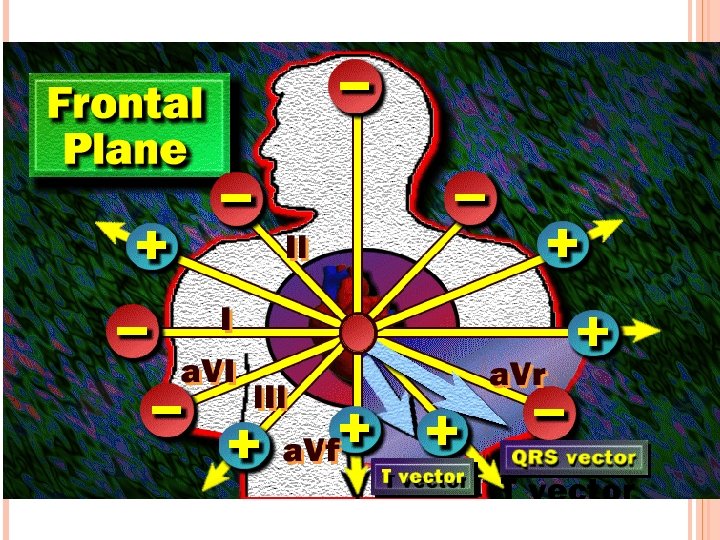
ECG Limb Leads

Augmented Leads: a. VR + _

Augmented Leads: a. VL + _

Augmented Leads: a. VF + _

ECG Augmented Limb Leads
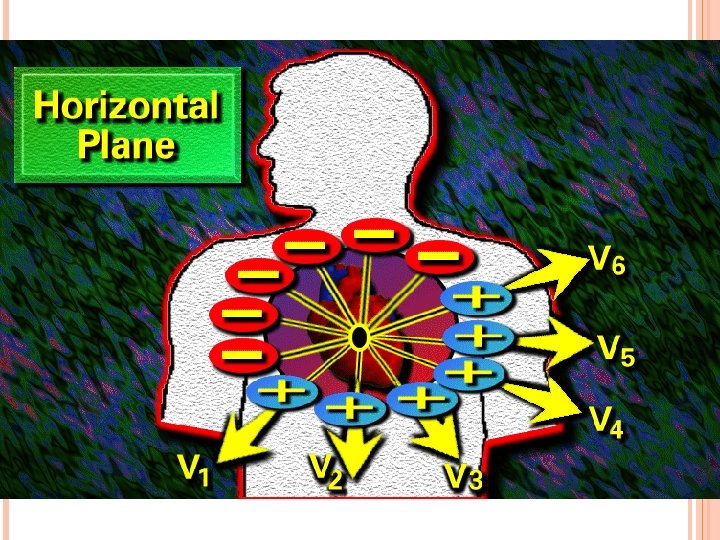

Unipolar Chest Leads v 1: fourth intercostal space, at right sternal margin. v 2: fourth intercostal space, at left sternal margin. v 3: midway between v 3 and v 4: fifth intercostal space, at mid clavicular line. v 5: same level as v 4, on anterior axillary line. v 6: same level as v 4, on mid axillary line.
 + _")
Unipolar Chest Leads (cont. ) + _

ECG Precordial Leads
 H M V 9 V 8 V 7")
Current Lead Placement Conventions (22 Electrodes) H M V 9 V 8 V 7 V 3 R V 6 R V 5 RV 4 R I E 6 R I 5 R 3 R E Current clinical conventions may use 22 different leads
 RA (white) RL (green) LA (black) LL (red)")
ECG Lead Color Codes C (brown) RA (white) RL (green) LA (black) LL (red)

Surface Cardiac Potentials taken at t = to suggests an equivalent dipole located within the heart

Eindhoven’s Triangle -very crude solution to inverse problem using bipolar limb leads: _ lead I + RA _ LA _ lead III + + LL

NORMAL HEARTBEAT AND ATRIAL ARRHYTHMIA Normal rhythm Atrial arrhythmia AV septum

Ventricular depolarization
")
Ventricular depolarization (cont’d)
")
Ventricular depolarization (cont’d)

Ventricular repolarization - + + -+ + - - + - +- + - + + -+ + +

Lead I

Lead II

Lead III
 Lead III")
Limb Leads Lead I (bipolar) Lead III

a. VR

a. VL

a. VF

Unipolar Lead a. VR a. VL a. VF

Normal values Intrinsicoid deflection < 0. 05” QT segment Men < 0. 39” Wo < 0. 40” ST segment Std: > 1 mm Pre : > 2 mm PR interval 0. 12 -0. 20” P wave 00. 8 -0. 11” U wave QRS duration 0. 06 -0. 10” T wave

Precordial leads V 6 V 1 V 2 V 3 V 4 V 5

Horizontal vs Vertical heart

Horizontal vs Vertical heart

Clockwise vs Counter clockwise rotation 4 1 1 3 3 24 2 4 4 2 2 11 3 3 Viewed from below the heart looking towards the apex in vertical heart

P wave V 1
")
Atrial Enlarge ment Left atrial enlargement P mitral Wide and notch Biphasic with (-) terminal component V 1
 Right atrial enlargement Tall and peaked P wave V 1")
Atrial Enlarge ment (cont’d) Right atrial enlargement Tall and peaked P wave V 1

Electrical axis q. RS = +3 Lead I q. RS = +1 a. VF

The QRS Bundle of His LBB Anterosuperior division Posteroinferior division RBB

The QRS vectors: • Initial depolarization • Terminal depolarization • S-T segmen • Re-polarization 4 2 3 V 1 1 V 6

Myocardial injury Electrical forces are directed away from a injured area A Normal B Minimal C Subendocard D Transmural E Subepicard

Myocardial injury ST segment deviated towards the surface of injured tissue A Normal B Minimal C Subendocard D Transmural E Subepicard

Myocardial infarction Zones of myocardial infarction: • Necrosis • Injury • Ischaemia 4 3 2 1 3 1 22 1 3 4
 ECG parameters of myocardial infarction: • Necrosis • Injury • Ischaemia")
Myocardial infarction (cont’d) ECG parameters of myocardial infarction: • Necrosis • Injury • Ischaemia 4 2 1 3 V 1 V 6
 Phases of myocardial infarction: • Hyperacute phase - Slope elevation of")
Myocardial infarction (cont’d) Phases of myocardial infarction: • Hyperacute phase - Slope elevation of the ST sement - Tall widened T wave - Increased ventr. activation time • Fully evolved phase - Pathological Q wave - Coved, elevated ST segment - Inverted symetrical T wave • Old infarction - Pathological Q wave - ST segment and T wave return to normal
 2 1 V 2 V 3 3")
Myocardial Localization of infarcted areas infarction (cont’d) 2 1 V 2 V 3 3 II, III, a. VF I a. VL V 4 V 5 V 6

Right ventri cular hyper trophy 4 2 3 V 1 1 V 6

Left ventri cular hyper trophy Diatolic overload 4 2 3 V 1 1 V 6

Left ventri cular hyper trophy Systolic overload 4 2 3 V 1 1 V 6

RBBB 4 3 V 1 1 2 V 6

LBBB 4 3 2 V 1 1 a 1 b V 6

QT interval Prolonged QTc • Hypocalcemia • Acute rheumatic carditis Shortened QTc • Hypercalcemia • Digitalis effect • Hyperthermia • Vagal stimulation Normal QT does not exclude the diagnosis of QTc= QT R-R • Acute myocardial infarction • Acute myocarditis of any causes • Sympathetic stimulation • Procain effect

Atrial Septal Activation Disturbances of impulse formation Sinus rhythms • Sinus arrythmia • Sinus tachycardia • Sinus bradycardia Ectopic atrial rythms • Atrial extrasystole • PAT • Atrial fibrilation • Atrial flutter AV nodal rythms • AVn extrasystole • Paroxysmal AVn tachycardia • Idionodal tachycardia Ventricular rhytms • V-extrasystole • V-tachycardia • V-flutter • V-fibrilation • Idioventricular tachycardia

Arrhyth mias Disturbances of impulse conduction A-V block S-A block Reciprocal rythms WPW syndrome (Wolf-Parkinson-White) LGL syndrome (Lawn-Ganong-Levin)

Arrhyth mias 2 nd disorders of rythms A-V dissociation Atrial escape Aberrant ventricular conduction AVn escape Ventricular escape

Arrhyth mias Diagnostic approach To be continued next week Insyaa Allah

Arrhyth mias 4 2 3 V 1 1 V 6

Arrhyth mias 4 2 3 V 1 1 V 6

Arrhyth mias 4 2 3 V 1 1 V 6

Arrhyth mias 4 2 3 V 1 1 V 6

Arrhyth mias 4 2 3 V 1 1 V 6

Electrocardiogram The Waves P wave atrial depolarization duration 0. 11 s amplitude < 3 mm detects atrial function SA node

Electrocardiogram The Waves QRS Complex ventricular depolarization duration 0. 10 s detects ventricular function Q wave first downward stroke R wave first upward stroke S wave any downward stroke preceded by an upward stroke T wave ventricular repolarization

Intervals and Segments PR segment end of P wave to start of QRS measures time of depolarization through AV node PR interval start of P wave to start of QRS measures time from start of SA conduction to end of AV node conduction normal 0. 12 -0. 20 s

Intervals and Segments ST segment end of QRS complex to start of T wave measures start of ventricular repolarization elevated in MI’s ST interval end of QRS to end of T wave represents complete time of ventricular repolarization QT interval start of QRS to end of T wave duration of ventricular systole < 1/2 of the RR interval

Intervals and Segments Intervals the timing for depolarizations/repolarizations can be interpreted from the EKG P-R 0. 12 -0. 2 sec measures the time between the start of atrial depolarization and the start of ventricular depolarization a long P-Q interval is a sign of AV node dysfunction QT interval, about 0. 4 sec start of QRS to end of T wave QRS 0. 08 -0. 1 sec wider with ventricular dysfunction ST segment (don’t worry about time) elevated with acute MI

Electrocardiogram The waves more on the QRS note that the Q or the R or the S wave is not always present name according to direction of first deflection, second, etc Q waves are often absent lead V 1 no Q small R large S lead V 2 no Q large R small S

Heart Rate defined as beats per minute easy way to estimate rate find an R wave on a thick line count off on the thick lines 300, 150, 100, 75, 60, 50 until you reach another R wave 75 100 150 300 in our example the middle R wave falls on the dark line the next R falls just before the 75, so estimate about 80 bpm

Heart Rate Normal Sinus Rhythm heart rate between 60 -100 bpm pacing by SA node. QRS after every P wave rhythm is regular Sinus Tachycardia heart rate > 100 bpm p wave is there but hidden by the T wave regular QRS rhythm Sinus Bradycardia heart rate < 60 bpm QRS after every P wave regular rhythm

Wave Abnormalities ST segment elevation ischemia Q wave in some leads may indicate ischemia and necrosis T wave inversion late sign of necrosis and fibrosis

Rhythm Abnormalities Atrial Fibrillation multifocal areas in atria firing no p waves and irregular heart rate
 AV Block AV node cannot conduct impulse p")
Rhythm Abnormalities Complete (3 rd degree) AV Block AV node cannot conduct impulse p waves and QRS not connected irregular heart rate

Rhythm Abnormalities Premature Ventricular Contractions ventricles pace early heart beat large QRS

Rhythm Abnormalities Ventricular Tachycardia rapid ventricular pacing rapid, regular rate wide QRS

Rhythm Abnormalities Ventricular Fibrillation multifocal ventricular beats irregular won’t last long

Axis -90 QRS AXIS + — 180 0 another name for the vector of depolarization an axis is measured in degrees the axis is measured by adding the positive deflection and subtracting the negative deflection overall + is left axis direction overall - is right axis direction for lead one most of the QRS is positive, therefore it has a leftward axis if an MI caused the QRS to be mostly negative the lead would have a rightward axis +90

Axis -90 — 180 0 +90 + QRS AXIS lead II positive on left leg negative on right arm looking at the tracing we see that the QRS is mostly positive what does this mean?

Axis -90 — 180 0 +90 + QRS AXIS lead III positive on left leg negative on left arm looking at the tracing we see that the QRS is mostly positive what does this mean?

Axis -90 QRS AXIS lead I leftward axis lead II downward axis from this we can see that a normal QRS axis lies somewhere in between 0 and +90 degrees + — 180 0 +90 + remember that infarction will cause the axis to shift rightward (>+90) and that hypertrophy will shift the axis upward (between 0 and -90)

The Anatomy of the Heart The Blood Supply to the Heart • Coronary circulation meets heavy demands of myocardium for oxygen, nutrients • Coronary arteries (right, left) branch from aorta base • Anastomoses (arterial interconnections) ensure constant blood supply • Drainage is to right atrium • Great, middle cardiac veins drain capillaries • Empty into coronary sinus

Blood Supply to the Heart • Arteries include the right and left coronary arteries, marginal arteries, anterior and posterior interventricular arteries, and the circumflex artery • Veins include the great cardiac vein, anterior and posterior cardiac veins, the middle cardiac vein, and the small cardiac vein

SA node activity and atrial activation begin. SA node Time = 0 Stimulus spreads across the atrial surfaces and reaches the AV node Elapsed time = 50 msec There is a 100 -msec delay at the AV node. Atrial contraction begins. AV bundle Elapsed time = 150 msec Bundle branches The impulse travels along the interventricular septum within the AV bundle and the bundle branches to the Purkinje fibers. Elapsed time = 175 msec The impulse is distributed by Purkinje fibers and relayed throughout the ventricular myocardium. Atrial contraction is completed, and ventricular contraction begins. Elapsed time = 225 msec Purkinje fibers

Coronary Circulation

Coronary Circulation

Coronary Circulation Figure 20. 9 a, b

Coronary Circulation Figure 20. 9 c, d

HOLTER MONITOR Technology • 5 electrodes • 2 -3 leads • Derived 12 lead available • Digital or analog recording • Digital transmission to analyzer • Requires removal of Holter monitor to scan recording

HOLTER MONITOR Uses: • Patients experiencing daily symptoms • Precise quantification of arrhythmias Positives: • 24 -48 hours full disclosure available • Heart rate and AF burden graphs • Arrhythmia counts (ex. , 10 PVCs per hour)

- Slides: 100