ECG changes in children Pediatric Cardiac Centre Bratislava

ECG changes in children Pediatric Cardiac Centre, Bratislava 2020

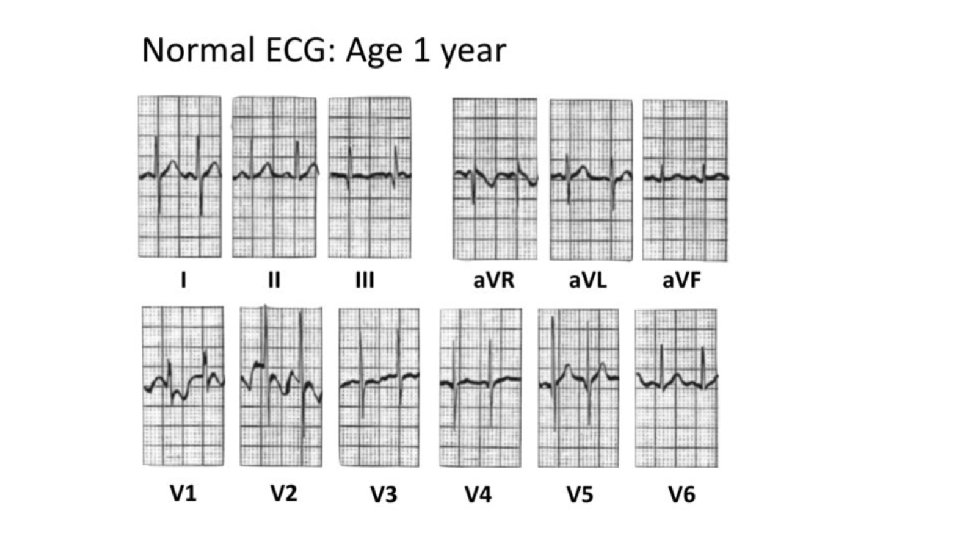
Pediatric ECG interpretation • At birth, the right ventricle is larger and thicker than the left ventricle, reflecting the greater physiological stresses placed upon it in utero (pumping blood through the relatively highresistance pulmonary circulation). • This produces an ECG picture with right ventricular hypertrophy : marked rightward axis, dominant R wave in V 1 and T-wave inversions in V 1 -3. • PR interval, QRS duration are shorter than in adults due to the smaller cardiac size. • Heart rates are much faster in neonates and infants, decreasing as the child grows older.

Common findings on the pediatric ECG • • • Heart rate >100 bpm Rightward QRS axis > +90° T wave inversions in V 1 -3 (“juvenile T-wave pattern”) Dominant R wave in V 1 RSR’ pattern in V 1, V 2 Respiratory sinus arrhythmia PR interval < 120 ms and QRS duration <80 ms Slightly peaked P waves (< 3 mm in height is normal if ≤ 6 months) Slightly long QTc (≤ 490 ms in infants ≤ 6 months)
 Regular : RR intervals of equal")
Pediatric ECG description 1. Heart action a. ) Regular : RR intervals of equal durations b. ) Nepravidelná : RR intervals of different durations (regularly irregular / irregularly irregular) in chiildren respiratory arrhythmia very common
 Sinus : atrial depolarization starts from SA")
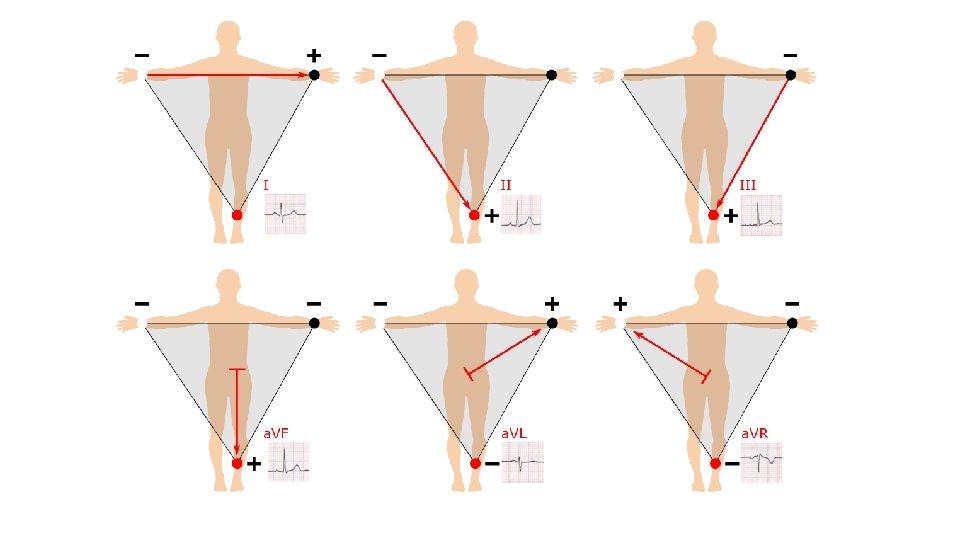
Pediatric ECG description 2. Rhythm a. ) Sinus : atrial depolarization starts from SA node: • P wave preceding each QRS complex, with a constant PR interval • P wave positive in leads I, III, a. VF • P wave negative in a. VR, biphasic in V 1
 Non-sinus • Atrial rhythm – P waves present, different morphology • Junctional")
b. ) Non-sinus • Atrial rhythm – P waves present, different morphology • Junctional rhythm – P waves hidden in narrow QRS complexes • Idioventricular rhythm – absent P waves, wide QRS complexes
 Heart rate (bpm) < 1 day 123 (93154) 6")
Age Heart rate Age (bpm) Heart rate (bpm) < 1 day 123 (93154) 6 -11 months 134 (109 -169) 1 -2 days 123 (91159) 1 -2 years 119 (89 -151) 3 -6 days 129 (91166) 3 -4 years 108 (73 -137) 1 -3 weeks 148 (107182) 5 -7 years 100 (65 -133) 1 -2 months 149 (121179) 8 -11 years 91 (62 -130) 3 -5 months 141 (106186) 12 -15 years 85 (60 -119) 3. Rate • 25 mm/s paper speed (1 small □ = 0. 04 s): 300 / number of large □ between R waves = beats per minute number of small □ x 0. 04 = X 60 : x = beats per minute • 50 mm/s paper speed (1 small □ = 0. 02 s): 600 / number of small □ between R waves = beats per minute number of small □ x 0. 02 = X 60 : x = beats per minute

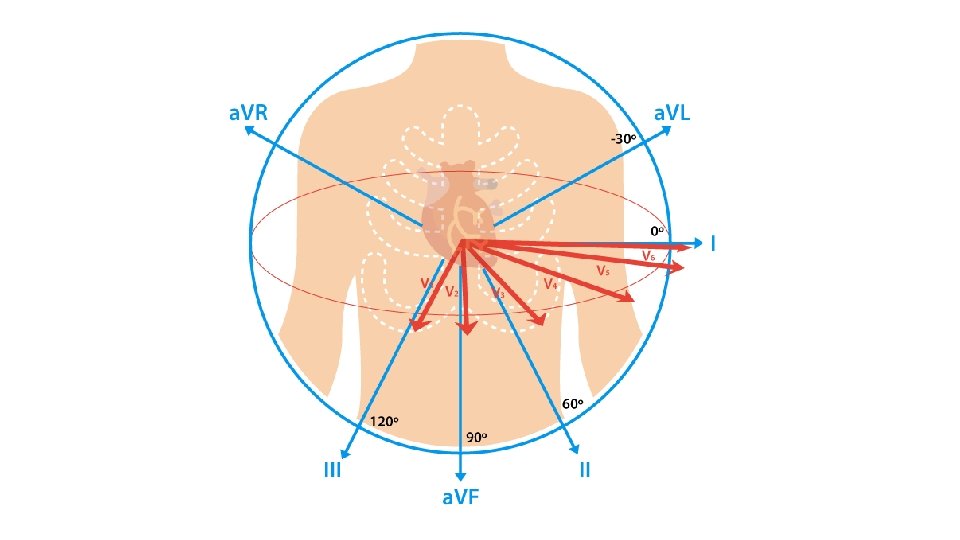
4. Heart axis • Normal QRS axis varies with age: 1 week – 1 month: + 110° (range +30° to +180°) 1 month – 3 months: + 70° (range +10° to +125°) 3 months – 3 years: + 60° (range +10° to +110°) Over 3 years: + 60° (range +20° to +120°) Adult: + 50° (range -30° to 105°) I a a. VF – according to lead I and a. VF Initial Right Axis on ECG is normal and resolves after the first 6 months of life

5. P wave • • • The first positive wave on ECG Represents atrial depolarization duration: <0. 12 s morphology: monophasic in II, biphasic in V 1 orientation positive in I, II, a. VF, negative in a. VR, biphasic in V 1 amplitude: 2. 5 mm in limb leads / < 1. 5 mm in chest leads Zvod II normal Right atrial enlargement – P pulmonale (pulmonary hypertension) (amplitude > 2. 5 mm) Left atrial enlargement - P mitrale mitral stenosis) Duration > 0. 12 s)
 voltage • High QRS complexes : ventricular hypertrophy, conduction")
6. QRS complex a. ) voltage • High QRS complexes : ventricular hypertrophy, conduction disorders (BBB´s, WPW) • Nízke QRS komplexy: pericarditis, myocarditis, hypothyreoidism, hypothermia, pericardial / pleural effusion emphysema, newborns b. ) duration • < pre-school age: < 0. 08 s • older children: not more than 0. 1 s c. ) morphology • presence of δ-wave: WPW syndrome • r. SR´ configuration in V 1, V 2 : RBBB • „M-shaped“ QRS in V 5, V 6 : LBBB

Q wave • • • septum depolarization depth: < 25% of QRS width <0. 04 s present in leads I, (III), V 5 -V 6 abnormalities: - Q wave present in right chest leads (i. e. V 1 ) – severe right ventricular hypertrophy - absent Q waves in left chest leads (LBBB) - abnormally deep Q wave (ventricular hypetrophy due to volume overload) - abnormally deep and wide Q waves (ischemia, fibrosis)
 LV hypertrophy b. ) RV hypertrophy – normal in children")
Ventricular hypertrophy a. ) LV hypertrophy b. ) RV hypertrophy – normal in children < 1 year High R waves in I, III, a. VF, V 5 -V 6 Deep S waves in V 1 -V 2 ↑R/S in V 6 and ↓ R/S in V 1 Q waves in V 5/V 6 ≥ 0. 5 m. V High positive T waves ± ischemic changes High R waves in V 1 -V 2, av. R Deep S kmity in I, V 5/V 6 ↑R/S in V 1 amd R/S < 1 in V 6 (if > 1 y. o. ) q. R in lead V 1 R´ configuration with R´ > 1. 5 m. V (infants) or > 1 m. V (older) ± ischemické zmeny

7. ST segment – normal ST segment is isoelectric pathological changes : • abnormalities present in ≥ 2 leads • ST depressiom > 0. 05 m. V • myocardial ischemia, severe ventricular hypertrophy, digitalis, hypo. K+ • abnormalities present ≥ 2 leads • ST elevation : > 0. 10 m. V • ischemia, pericarditis, early repolarization syndrome

T wave • The precordial T-wave configuration changes over time: ü For the first week of life, T waves are upright throughout the precordial leads. ü After the first week, the T waves become inverted in V 1 -3 (= the “juvenile T-wave pattern”) ü This T-wave inversion usually remains until ~ age 8; thereafter the T waves become upright in V 1 -3. ü However, the juvenile T-wave pattern can persist into adolescence and early adulthood (= “persistent juvenile T waves”). Tall peaked T waves Hyperkalaemia LVH (volume overload) Benign early repolarisation Flat T waves Normal newborns, hypothyreoidism, hypokalaemia, digitalis, pericarditis, myocardial ischemia

8. Normal durations PQ interval – depends on age and heart rate: • Pre-school age: 0. 07 – 0. 16 s • Older children: 0. 09 – 0. 18 s • prolonged: AV block I. degree, myocarditis, some CHD (Ebstein anomaly, ASD), digitalis, hyper. K+ • shortened : preexcitation QRS ocmplex – depends on age • prolonged: LBBB/RBBB, preexcitation, intraventricular block, ventricular arrhythmias

QT interval / QTc interval • depends on heart rate • we use Bazett formula (QTc corrected to heart rate): QTc = measured Qred. T / (√R–R interval) • mostly lead II or V 5 • 3 measurements, average value • normal values: Infants < 6 mesiacov : < 0. 49 sec Children > 6 mesiacov = < 0. 44 sec Women : 0. 37 - 0. 45 sec Men: 0. 36 - 0. 43 sec Prolonged QTc : hypocalcemia, myocarditis, long QT syndrome, head injuries, drugs Shortened QTc : hypercalcemia, digitalis, congenital form of short QT syndrome

Healthy 2 -year-old boy: • • SR 110 bpm dominant R wave in V 1 -3 RSR’ cofingurarion (morphology of incomplete RBBB) in V 1 Juvenile T-wave pattern in V 1 -3
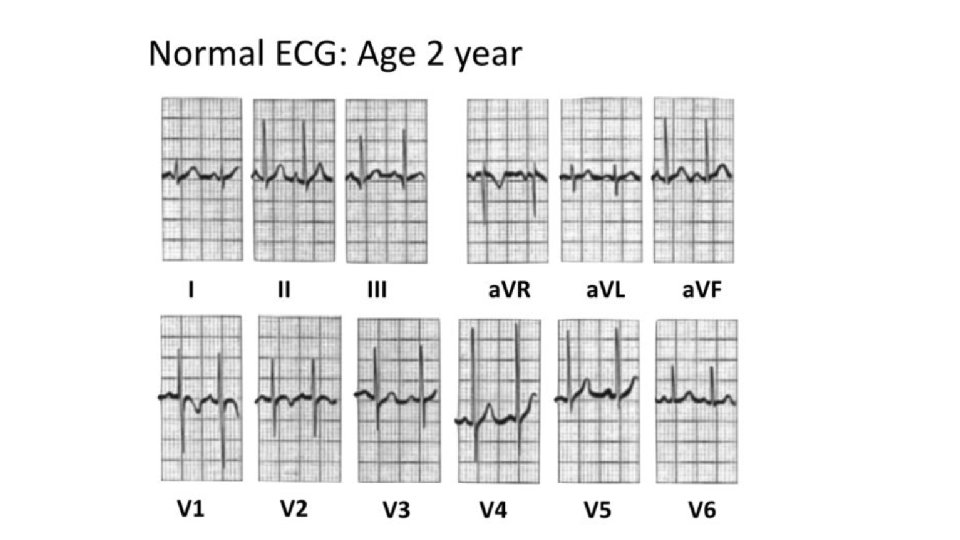

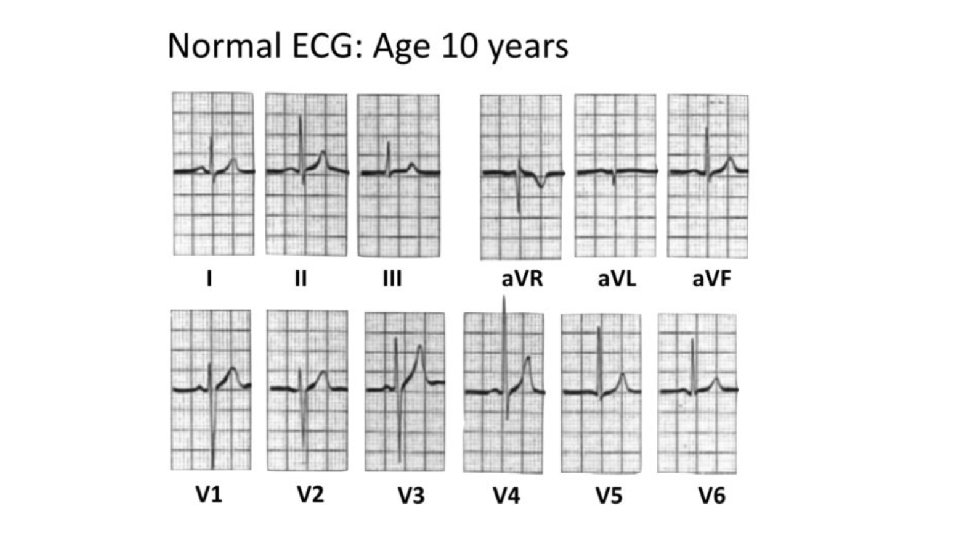
Right ventricular dominance in newborns and infants is being replaced by left ventricular dominance and ECG in 3 -5 y. o. children is starting to be similar to that in adult patients.
- Slides: 23