EBUS in staging lung cancer Vincent Ninane SaintPierre

EBUS in staging lung cancer Vincent Ninane, Saint-Pierre Hospital, Brussels, Belgium

Pre-operative mediastinal staging of NSCLC l Purpose : to exclude – Involvement of mediastinal contralateral side (N 3 disease) – (Extensive) involvement of the ipsilateral side (N 2 disease) medical management
 CT scan Sensitivity Specificity Accuracy FDG-PET 65%")
Non-invasive Mediastinal Staging (15 studies; 719 patients) CT scan Sensitivity Specificity Accuracy FDG-PET 65% 89% (range: 20 -86) (range: 67 -100) 80% 92% (range: 43 -90) (range: 79 -100) 75% (range: 52 -79) 90% (range: 78 -100) Vansteenkiste Eur Respir J 2001; 17: 802 -20

Invasive Mediastinal Staging l Before PET introduction – Nearly all cases (low performance of CT scan) – Or enlarged lymph nodes on CT scan l After PET introduction – Positive hot spots (inflammatory processes) – Additional situations (PET + N 1 tumors, mediastinal lymph nodes > 16 mm on CT scan, low SUV tumors, central tumors) De Leyn et al. Eur J Cardiothorac Surg. 2007 Jul; 32: 1 -8.

Comparison of characteristics of invasive tests Detterbeck et al. Chest 2003; 123: 167 S-175 S

Accuracy of standard cervical mediastinoscopic biopsies in LC Source Years No of patients sensitivity specificity 14 papers 83 -99 5687 0. 81 1. 00 PPV 1. 00 NPV 0. 91 prevalence 0. 37 Mediastinoscopy is the gold standard ! Toloza et al. Chest 2003; 123: 157 S-166 S

Guidelines : invasive intrathoracic staging Royal College of Radiologists 1999 Mediastinal sampling if enlarged LN (> 1 cm) ACCP 2003 l. Extensive infiltration: TTNA or EUS-NA or TBNA l. CT enlarged discrete LN : mediastinoscopy l. PET + LN : mediastinoscopy l. CT normal LN : mediastinoscopy l. PET – LN : mediastinoscopy ASCO 2003 NICE 2005 Biopsy if enlarged LN (>1 cm) on CT (even PET -) Or PET + LN Histo/cytological sampling if enlarged LN (>1 cm) on CT Or PET + LN (PET - enlarged LN should not be controlled) ACCP 2007 l. Extensive infiltration : radiographic assessment l. CT enlarged discrete LN (PET + or -) : invasive or minimally invasive l. Central tumor or N 1 : mediastinoscopy (needles 2 nd choice) l. Peripheral stage I tumor and PET + mediastinum : mediastinoscopy (needles 2 nd choice)

Factors associated with increased diagnostic yield during needle aspiration lymph node size l number of aspirates l histological in addition to cytological samples; rapid on-site sample evaluation l real-time imaging control of aspiration l Mehta et al. J Bronchology 2000; 7: 268 -272; Morrissey et al. Thorax 3; 48: 632 -7; Chin et al. Am J Respir Crit Care Med 2002; 166: 377 -381.

Endobronchial ultrasound • Miniaturized probes • ultrasound catheters • Radial transducer at the tip • Rotation at 400 revolutions/mn (rpm) • Olympus : 20 MHz (dia 2. 5 mm)

EBUS and CT scan of area 4 R lymph node

Ultrasound-guided needle aspiration of LN l randomized controlled study – TBNA with/without EBUS – 200 patients with enlarged mediastinal LN – group A (subcarinal LN) vs group B (others) l yield of both groups TBNA EBUS-TBNA Group A (%) 74 Group B (%) 58 86 (NS) 84 (S) Overall (%) 71 Herth et al. Chest 2004; 125, 322 80 (S)

Ultrasound puncture bronchoscope l Convex probe with a frequency of 7. 5 MHz – Linear transducer that scans parallel to the insertion direction of bronchoscope – Contact with/without balloon inflated with saline Ultrasound scanner l Doppler mode l Bronchoscope : outer diameter of 6. 7 mm, direction of view is 30° toward oblique, channel diameter of 2. 0 mm l Dedicated 22 -gauge needle l

EBUS : our experience Nb of procedures 2003 2004
 l Anesthesia of")
EBUS-TBNA : Methods l Outpatient basis l Conscious sedation (iv midazolam) l Anesthesia of the airways l O 2 (2 L/min; nasal prongs) l Transcutaneous hemoglobin saturation and cardiac rhythm monitoring
 l Adapter Valve")
Attach the accessories of endoscope l Suction valve (MAJ-207 or 209) l Adapter Valve (MAJ-1414) l Syringe with the extension tube for the balloon l Balloon (MAJ-1351)

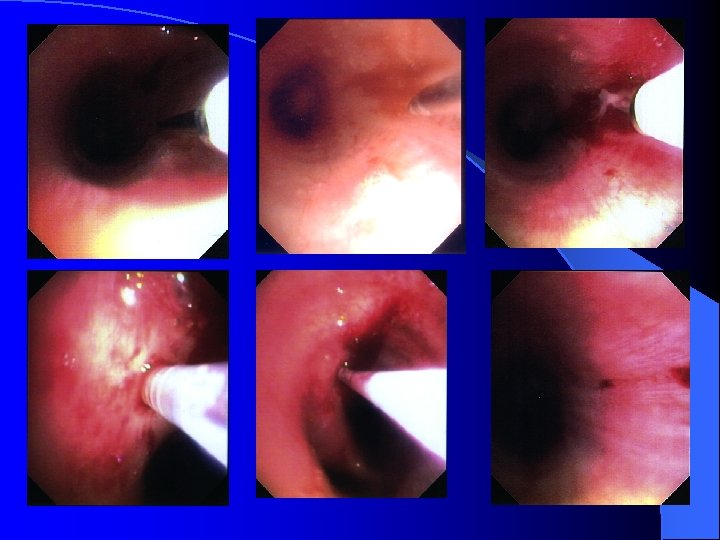
Endoscopic view l To check the position under Endoscopic view. l And switch to Ultrasonic view.

Check the aspiration needle l Check the needle slider is pulled back completely. l Check the tip of needle whether it completely disappear from the distal end of the sheath. Needle slider Sheath

Check the vessels l Check the vessel by Power Doppler function.

Push & pull the needle in LN l Repeat pushing and pulling the needle in order to get enough specimen.

Pull back the needle The needle is pulled back completely. l Check bleeding on Endoscopic view. l

Technical aspects l Order of EBUS examination and sampling – Examination : from distally to proximally l Detection of lymph nodes down to a size of 2 -3 mm – Sampling : because of the risk of contamination from N 3 to N 2 stations l and finally N 1, for diagnostic purpose only l

EBUS-EUS complementarity 1 6 EUS EBUS 7 8 9 9

Technical aspects : sampling l Accessible lymph node for punction : short diameter 5 mm l Optimal number of aspirations per lymph node station : 3 Lee HS et al. Chest 2008 Feb 8. [Epub ahead of print]

Technical aspects l Cytopathological specimens – aspirated material smeared onto glass slides l air-dried and also fixed in 70% alcohol – Catheter and needle flushed with one millilitre of Na. Cl 0. 9 % l material collected for cytological examination – in some cases, tissue cores Results : positive (tumor cells), negative (lymphocytes or lymphoid tissue), inadequate (blood only, bronchial epithelial cells, cartilage) l Benefit of ROSE (rapid on-site sample evaluation) not studied l

EBUS-TBNA : Tolerance and Complications l Tolerance under local anaesthesia – Cough is frequent (active smokers, open tracheostomy) l Complications – Only mild bleeding – Pneumothorax (1/~500 examinations) – Bacteremia and other infectious complications ?

EBUS-TBNA in mediastinal lymph node staging Studies Indication Nb of patients Sensitivity Accuracy NPV Yasufuku 2004 CT enlarged 70 96 97 92 Yasufuku 2005 CT enlarged 108 95 96 90 Herth 2006 CT enlarged 502 94 94 Herth 2006 Normal CT 100 92 Bauwens 2008 PET increased uptake 106 95 Herth 2008 Normal CT and PET 97 89 (8/9) 96 97 91 98

Meta-analysis of endoscopic ultrasound Silvestri 199632 Gress 199731 Williamsi 199916 Fritscher-Ravens 200030 Wiersema 200129 Wallace 200128 Larsen 200227 Fritscher-Ravens 200326 Kramer 200425 Wallace 200424 Savides 200415 Eloubeidi 200522 Le Blanc 200521 Larsen 200520 Caddy 200519 Annema 2005 -JAMA 18 Tournoy 200523 Annema 200517 0, 2 0, 4 18 studies Pooled sensitivity : 8 studies with abnormal CT Pooled sensitivity : 90% 4 studies with normal CT Pooled sensitivity : 58% Sensitivity and 1 specificityof EUS-FNA in the assessment of LN metastases (N 2/N 3). Error bar = 95% IC. 0, 6 Sensitivity Micames et al. Chest. 2007; 131: 539 -548 83% 0, 8 1 0 0, 2 0, 4 0, 6 1 -specificity 0, 8

Guidelines : invasive intrathoracic staging Royal College of Radiologists 1999 Mediastinal sampling if enlarged LN (> 1 cm) ACCP 2003 l. Extensive infiltration: TTNA or EUS-NA or TBNA l. CT enlarged discrete LN : mediastinoscopy l. PET + LN : mediastinoscopy l. CT normal LN : mediastinoscopy l. PET – LN : mediastinoscopy ASCO 2003 NICE 2005 Biopsy if enlarged LN (>1 cm) on CT (even PET -) Or PET + LN Histo/cytological sampling if enlarged LN (>1 cm) on CT Or PET + LN (PET - enlarged LN should not be controlled) ACCP 2007 l. Extensive infiltration : radiographic assessment l. CT enlarged discrete LN (PET + or -) : invasive or minimally invasive l. Central tumor or N 1 : mediastinoscopy (needles 2 nd choice) l. Peripheral stage I tumor and PET + mediastinum : mediastinoscopy (needles 2 nd choice)
 Positive (N 2 -N 3) T 1 N 0")
CT scan Negative (N 0) Positive (N 2 -N 3) T 1 N 0 Sq. CC ALL Surgical treatment a OTH ERS Tissue confirmation Medscopy – + EBUS/EUS (FNA) b – + Multimodality treatment De Leyn et al. Eur J Cardiothorac Surg. 2007 Jul; 32: 1 -8. EBUS/EUS : minimally invasive procedure (a) but lower negative predictive value than mediastinoscopy (b)
 a Tissue confirmation Medscopy – Surgical treatment")
PET/PET-CT Negative Positive (N 2 -N 3) a Tissue confirmation Medscopy – Surgical treatment + b EBUS/EUS (FNA) c – + Multimodality treatment De Leyn et al. Eur J Cardiothorac Surg. 2007 Jul; 32: 1 -8. a : PET N 1 +; central tumors; low tumoral FDG uptake; LN size 1. 6 cm EBUS/EUS : minimally invasive procedure (b) but lower negative predictive value than Medscopy (c)

EBUS-TBNA in combination with EUS-NA l Complementary methods l Combined approach – Same results as routine mediastinoscopy Herth et al. Am J Respir Crit Care Med 2005; 171: 1164/Vilman et al. Endoscopy 2005; 37: 833/ Wallace et al. JAMA 2008; 299: 540

EBUS-EUS complementarity 1 6 EUS EBUS 7 8 9 9

EBUS for restaging the mediastinum Number sensitivity specificity accuracy 83 70% 100% 75% CT restaging : 44 RR; 39 SD 143 N 2 stations assessed Krasnik et al. ERS Munich 2006

Initial and post-induction invasive mediastinal staging Initial Mediastinoscopy EBUS/EUS Post-induction Limitations Remediastinoscopy technically difficult; Accuracy decreased EBUS/EUS False negative EBUS/EUS incomplete staging by EBUS/EUS Mediastinoscopy False negative EBUS/EUS incomplete staging by EBUS/EUS False negative EBUS/EUS
")
Training of EBUS l No recommendation for linear EBUS – Recommendations (ACCP and ATS/ERS) for radial probes (RP) l l ERS/ATS : 40 RP supervised procedures and 25 RP procedures per year to maintain competency Centers candidates for linear EBUS – Critical number of patients (maintenance of competency) – Multidisciplinary lung cancer clinic – Limited number of practitioners should acquire the expertise in each center Bolliger C et al. Eur Respir J 2002; 19: 356//Sheski FD et al. Chest 2008; 133: 264

General conclusions : invasive mediastinal staging Mediastinoscopy is the gold standard l Initial staging l – EBUS is safe and accurate and will reduce the need for mediastinoscopy as well as cost – Combined EBUS and EUS may be a superior approach l Restaging : the best combination (stagingrestaging) needs to be assessed
- Slides: 38